
Abstract
Several companies offer anatomically shaped breast implants but differences among manufacturers are often misunderstood. The shell texture is a crucial parameter for anatomically shaped implants to prevent rotation and to decrease the risk of capsular contracture, even though concerns have recently been raised concerning the complications associated with textured breast implants. The aim of this study was to characterize differences in terms of texture, cell adhesion, shape, and stiffness between some commonly used anatomically shaped implants from three different manufacturers.
Methods
Five commercially available anatomically shaped breast implants from 3 different manufacturers (Allergan, Mentor, and Sebbin) were used. Scanning electron microscopy, X-ray microtomography, and scanning mechanical microscopy were used to characterize the shell texture. Human fibroblast adhesion onto the shells was evaluated. 3D models of the implants were obtained using CT-scan acquisitions to analyze their shape. Implant stiffness was evaluated using a tractiometer.
Results
Major differences were observed in the topography of the textures of the shells, but this was not conveyed by a statistically significant fibroblast adhesion difference. However, fibroblasts adhered better on anatomically shaped textured implants than on smooth implants (p < 0.01). Our work pointed out differences in the Biocell® texture in comparison with older studies. The 3D analysis showed significant shape differences between the anatomically shaped implants of the 3 companies, despite similar dimensions. Implant stiffness was comparable among the 3 brands.
Conclusions
Each texture had its specific topography, and this work is the first description of Sebbin anatomic breast implant texturation. Moreover, major discrepancies were found in the analysis of the Biocell® texture when comparing our results with previous reports. These differences may have clinical implications and are discussed. This study also highlighted major shape differences among breast implants from different manufacturers, which is quite counterintuitive. The clinical impact of these differences however needs further investigation.
No Level Assigned
This journal requires that authors assign a level of evidence to each submission to which Evidence-Based Medicine rankings are applicable. This excludes Review Articles, Book Reviews, and manuscripts that concern Basic Science, Animal Studies, Cadaver Studies, and Experimental Studies. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The latest generation of anatomically shaped breast implants has a highly cohesive silicone gel filling, allowing them to remain form stable in their pocket, as well as a textured shell containing a low-bleed barrier.
Shell texture is crucial for anatomically shaped implants to prevent rotation. Breast implant texture was also shown to decrease the risk of capsular contracture and rotation [1–4]. However, concerns have recently been raised concerning the complications associated with textured breast implants, such as late seromas [5, 6], double capsule [5, 7], or even anaplastic large cell lymphoma (ALCL) [6, 8–10]. Shell topographies and their mode of interaction with the host remains poorly described, despite the large range of different textures available on the market.
Various planning methods exist [11–14] to determine :
-
(1)
The vertical/horizontal position of the implant in relation to the nipple
-
(2)
The optimal tissue coverage of the lower pole
-
(3)
The position of the expected post-operative inframammary fold
Some surgeons based their decision on implant dimensions such as the length of the ventral curvature or LVC.
In the manufacturers’ catalogs, the ranges of anatomically shaped breast implants are typically organized under the form of a “matrix”, which at a given footprint (width/height) involves various available projections. For a given manufacturer, each base/projection couple is associated with a single volume and a single LVC.
Breast implants, anatomically shaped as well as round, are likely to need replacement during a patient’s lifetime (ruptures, capsular contracture, poor cosmetic results, etc.). When inserting implants in such secondary cases but also in primary ones it is important for surgeons to understand the characteristics of different manufacturer’s anatomical implants. Can we e.g., replace the anatomical implant from one manufacturer for that of another; with the only argument that these implants are “anatomically-shaped” if they have equal or very close dimensional characteristics (height, width, projection) ?
The aim of this ex vivo experimental work was to analyze differences among the anatomically shaped implants from different manufacturers in terms of shell texturing and interaction with human fibroblasts, three-dimensional (3D) shape, and stiffness.
Methods
Five silicone gel-filled highly cohesive anatomically shaped breast implants with a textured shell and a low-bleed barrier were studied. They consisted of two Allergan brand implants with Biocell® texturing (Irvine, California, USA), one Mentor brand implant with Siltex® texturing (Santa Barbara, California, USA), and two Sebbin brand implants (Boissy l’Aillerie, France). The implants were all less than 2 years old and were therefore all within their period of use. A summary of the theoretical dimensions of these implants is presented in Table 1.
Texturing Analysis
Scanning Electron Microscopy
A 2-cm2 shell sample was taken from each of the A1, M1, and S1 implants at the level of the upper pole. These samples were carefully cleaned with ethanol and observed under a scanning electron microscope (SEM) to analyze the texture. The acceleration voltage of the primary electronic beam was 5 keV. The intensity of the primary electronic beam was I = 10–11 A, the working distance was 25 mm.
X-ray Microtomography
Three-mm diameter samples from the A1, M1, and S1 shell were obtained with a hole punch. Each sample was imaged in a high-resolution micro-CT (Skyscan 1172, Bruke, Billerica, USA) with a voxel resolution of 2.94 µm. Techniques for the X-ray beam were set at 40 kV and 60 µA (LAMIH Laboratory, Valenciennes, France).
Scanning Mechanical Microscopy
Polymer replicas were made from the A1, M1, and S1 shell samples. A scanning mechanical microscope was used to provide data on the local elevations of the texture within an orthonormal system z (x, y). The built-in sensor was a diamond cone with a tip radius equal to 1 μm, corresponding to the lateral resolution, while the vertical resolution was 0.01 μm (FEMTO Laboratory, Besançon, France).
Cell Adhesion Analysis
A cell adhesion analysis was performed on the shell samples for the A1, M1, and S1 implants, as well as a smooth shell sample (SEBBIN, Boissy l´Aillerie, France). Disks with an area of 1 cm2 were cut out from each shell with a hole punch in sterile conditions. The samples were placed in wells of cell culture plates.
The test was performed using the human BJ dermal fibroblast cell line (ATCC® CRL-2522™). These fibroblasts were cultured in DMEM medium supplemented with 10 % fetal calf serum (v/v), 2 mM of glutamine, 100 U/ml of penicillin, and 100 µg/ml of streptomycin. Cells were maintained at the pre-confluent state. The cells were detached from the culture flask by a brief trypsin treatment, numbered after inactivation, and finally centrifuged. The cells were stained with calcein AM using the Vybrant® kit (Life Technologies, Grand Island, NY, USA).
Fibroblasts (200,000) were seeded on each sample as well as in wells without shell samples (control) and cultured for 1 h at 37 °C.
After an hour of cell culture, the non-adhesive cells were removed by rinsing. Calcein fluorescence was used to calculate the number of adherent cells by spectrofluorimetry (excitation at 494 nm and emission at 517 nm).
After fixation for 15 min with a 3 % (m/v) paraformaldehyde solution, adherent cells were observed by confocal laser scanning. The experiments were performed three times in duplicate. All numerical data from the adhesion tests were analyzed by the GraphPad INSTAT3 ® software (San Diego, California, USA).
Three-Dimensional Analysis
As part of this three-dimensional (3D) analysis the implants were divided into 2 groups by dimension equivalency among the brands, determined on the basis of the manufacturers’ specifications: width, height, and projection (Table 1).
Each implant underwent a computed tomography (CT) acquisition with millimetric thin slices (Brilliance 64 CT-scan, Philips Medical Systems, Best, The Netherlands). Based on these CT acquisitions, the implants were reconstructed in 3D by semi-automatic segmentation [15, 16] using dedicated software (itk-SNAP, University of Pennsylvania, USA). The 3D reconstructions of the implants from different manufacturers were subsequently analyzed in terms of sizes and shapes. Implant 3D models were superimposed 2 by 2 using a 3D matching technique. The differences of projection of the upper pole were measured at the level of the upper third of the height of the implants. We also determined the standard deviation of the distances between a point of the surface of an implant to the surface of the other implant (“point-to-surface distance”) to quantify the global differences in shape between an implant and another. To analyze and compare the local differences between 3D models, a color-coded system was used.
Implant Stiffness Analysis
The implant stiffness test was performed using a tractiometer (Lloyd Instruments, Bognor Regis, UK). The implants were positioned flat. The system was programed to penetrate a 25-mm diameter probe from a distance of 20 mm at the maximum projection point of the implant (Fig. 1). The penetration resistance force, (reaction to compression) was measured automatically in Newtons (N) but within the limits of the elastic deformation [17].The test was conducted 3 times on each implant, and the average of these three tests was noted.

Implants stiffness test
Results
Texturing Analysis
(Scanning electron microscopy, X-ray microtomography, scanning mechanical microscopy)
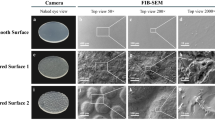
Figure 2 shows the images obtained by scanning electron microscopy.

Scanning electron microscopy images of A1, M1, and S1 shells
Figure 3 shows the images obtained using X-ray microtomography.

X-ray microtomography images of A1, M1, and S1 shells
The Allergan Biocell® texturing for the A1 implant shows irregular cuboid open wells (Figs. 2, 3) with sizes varying between 100 and 400 μm (average size 195 μm, SD = 77 µm) and depths between 100 and 200 μm. The density of these wells amounts to 12/mm2. The Mentor Siltex® texturing for the M1 implant is in a nodular form with nodule sizes between 50 and 300 µm and variations of altitude between peak and valleys of 250–300 µm.
The texturing of the textured Sebbin anatomically shaped implant is characterized by the presence of irregular wells with diameters between 150 and 600 µm (264 μm average diameter, SD = 90 µm) and depths between 100 and 200 μm. The density of these wells amounts to 7/mm2. Each well had the particularity to present raised edges thus forming domes more or less open at their top.
Cell Adhesion Analysis
The results of the cell adhesion test are shown in the Fig. 4. The adhesion tests with fibroblasts are a classic and a reliable method. We could confirm in the present study that the fibroblasts adhered better on the textured shells than on the smooth ones (p < 0.01). The data suggested a better adhesion for the A1 and S1 textures compared to M1. However, this difference was not statistically significant. Confocal microscopy analysis confirmed the results obtained with the adhesion tests: the cells were more numerous on the textured prostheses where the fibroblasts formed cellular aggregates that appeared to be more numerous in the location of the wells (Fig. 5).

Fibroblast adhesion test. Fluorescence is measured through an arbitrary unit (AU)

Fibroblast adhesion test. Confocal microscopy image
Three-Dimensional Analysis
The measurements performed on the three-dimensional models showed that the difference between actual and theoretical dimensions (width, height, and projection), did not exceed 3.2 % for all of the manufacturers.
Figure 6 shows a sagittal view of the A1, M1, and S1 3D reconstructions. Figure 7 shows a view of the superimposition of the implants by pairs. Figure 8 shows a 3D mapping of the differences between A2 and S2. Table 2 shows the point-to-surface distances among implants with equivalent dimensions from different manufacturers.

Sagittal view of the 3D models of A1, M1, and S1

Superimposition of the implants by pairs

S2 implant with a color mapping representing its distance to the A2 implant. Biggest differences are located at the upper pole where S2 is 11 mm more projected than A2
The upper pole of A1 was less projected than that of M1 and S1, with differences reaching, respectively, 10.4 mm and 9.5 mm. The same observations were made about the A2 and S2 implants. M1 and S1 had more similar shapes except for the upper edge of the implant, less projected on S1 than on M1 (Fig. 8; Table 2).
The point of maximum projection was placed at 33 % of the implant height for M1 and S1 but at 25 % for A1 (Fig. 6). These differences were similarly found for the A2 and S2 implants. They, however, were not conveyed by a difference in the measure of the LVC, the latter being 105 mm for A1, 103 mm for M1, and 105 mm for S1. LVC were 97 mm for S2 and 100 mm for A2.
Implant Stiffness Analysis
The results of the stiffness test are shown in Fig. 9. The stiffness of the A1, M1, S1, and S2 implants was substantially equal; whereas the A2 implant was significantly less firm.

Measurement of the stiffness of the implants using a tractiometer in Newton (N)
Discussion
Texturing Analysis
Scanning electron microscopy, X-ray microtomography, and scanning mechanical microscopy are reliable methods for the analysis of the surface of breast implants [2, 18–22]. The goal of shell texturation is to decrease the risk of rotation and capsular contracture [23, 24]
Whereas Allergan and Sebbin textures are obtained using calibrated salt crystals, the Mentor Siltex® texture is obtained through a negative-contact imprint of polyurethane foam [25]. Pore size is critical and is involved in the strength of attachment of ingrown fibrous tissue.
We found for the Mentor Siltex® texturing a characteristic nodular appearance, consistent with other data from the literature [19, 26, 27].The Allergan and Sebbin implant surfaces were more typical of salt texturing techniques, even if they presented very different aspects.
The cuboid appearance of the pores from the Biocell® texture had already extensively been described [18–21, 26–29]. The depth of the open pores is consistent with previous works, however the mean size of the Biocell® wells measured in the present study (195 µm,) was significantly lower than previous experimental studies. Indeed, in 2001, Danino et al. described pores of sizes ranging from 600 to 800 µm on the Biocell® texture [20, 21]. But more recently, and to support our findings, in 2009, Barr et al. observed pore sizes ranging from 200 to 500 µm. This was in agreement with the findings of Valencia-Lazcano et al. who found in 2013 pore sizes between 235 and 522 microns [26]. As others, Maxwell et al. [27] with scanning electron microscopy images, also showed wells of reduced size compared to Danino’s first report, in agreement with the hypothesis of a decrease of well size over time.
Based on this first report, these differences could be explained by a change in the caliber of crystals, and the process would have been changed between 2001 and 2014 after the change of production site (Ireland to Costa Rica). The clinical relevance of these findings, especially the smaller size of the wells of Biocell® texturing comparing to older studies, is unknown. If the pore size of the Biocell® texture (and not pores depth) has changed between 2001 and more recent publications, it may have biomechanical consequences. One can speculate that recent personal clinical experience from one of the authors (PH) using Allergan implants has been an increased non-adhesion, rotation [24, 30–33] or double capsule frequency [24, 30, 31, 33, 34]. Earlier publications with older generations of Allergan anatomical implants have reported a very low frequency of rotational (0.42 %) problems [23, 24, 35]. Moreover Giot et al. [22] showed that mechanical shear stress (directly related to pores size and their design) is a major factor in double capsule development. But another hypothesis has to be formulated: a mistake or a misjudgment in Danino’s first description. Indeed, as we already stated through our measurements (consistent with other authors), the pore dimensions were found to be lower than his findings. Our work is a good illustration of the necessity to verify previous statements. To answer this question, further studies are needed to compare texturation of anatomic implants before and after the moving of Allergan’s production site.
For capsular contracture many factors are involved, besides the implant shell texturation which could not be the single explanation: bacterial colonization [36], surgical approaches [37–39], biomechanical behavior of the capsule [40], previous irradiation…
Regarding the texturing of the Sebbin® anatomically shaped implants and their particular “open dome” texture, this is, to our knowledge, the first description. Despite the fact that both the Sebbin texture and the ALLERGAN Biocell® texture are obtained with salt crystals, one can observe very different aspects in the texture, most probably reflecting different manufacturing processes.
Cell Adhesion Analysis
The adhesion tests with fibroblasts are a classic and a reliable method [19, 26]. Surface texturation is supposed to decrease capsular contracture and implant rotation by the size of the pores [25].The marked shell texture differences between the three manufacturers observed by scanning electron microscopy were not obviously conveyed in the cell adhesion test. Indeed, if the results suggested a slightly better adhesion of the Biocell® and Sebbin textures when compared to the Siltex® texture, this was not statistically significant for the amount of analyzed samples. Siltex® texture is supposed to be less aggressive than Biocell® but there are still no clinical differences between the two texturations [32]. As expected and in contrast, we found a statistically significant increased adhesion of fibroblasts on the textured shells compared to the smooth shells.
Valencia-Lazcano et al. [26] characterized, using confocal microscopy, the Siltex® and Biocell® textures as well as the smooth shells from the Mentor and Allergan brands while studying the adhesion of human fibroblasts with a very similar protocol for cell adhesion. These authors also found poor adhesion to the smooth shells compared to the textured shells and no strong differences between textured implants [19, 26, 29]. Cell adhesion and cellular ingrowth are not only related to the topology of the shell surface but are most certainly multifactorial [2, 4, 26]. Even if cell adhesion is correlated with tissue adherence, it is not possible to make far-reaching conclusions with respect to how this affects the clinical adhesion of implants to surrounding tissue. Microtexturation has not been studied in this work, and further studies are needed to determine the advantages of this type of texturation.
Three-Dimensional Analysis
The three-dimensional analysis confirmed a good correlation between the manufacturer’s data and the actual dimensions (width, height, and projection) of the implants. This is of value for implant selection and the preoperative planning process.
This analysis was only performed on 5 implants and there could obviously be other implants in the manufacturer’s range that differ in actual and stated dimensions. However, the accurate correlation in the examined samples indicates that manufacturers accurately state their implant dimensions.
On the other hand, and this finding was very surprising, we found major shape differences between implants from different manufacturers despite very close-stated dimensions on width, height, and projection.
These differences may have direct clinical and esthetic implications because it has been shown that anatomical implant shapes are generally maintained once they are implanted [41, 42] and there are no major clinical differences between implant shape between horizontal and vertical position [27, 41]. It explains how two anatomical implants with equivalent dimensions can have so different volumes. The differences mainly concern the filling of the upper pole of the implants, with notable shape differences in the Allergan implants when compared to the Mentor and Sebbin implants (up to 1 cm projection difference for the devices analyzed in this study). The shapes of the Sebbin and Mentor implants seemed to be closer, with the differences in this case being rather localized on the upper end of the implant. The maximum projection point of the Allergan implants is placed significantly lower than that of the Mentor and Sebbin implants.
As for the studied implants, the LVC (used by some surgeons, for preoperative planning methods) were surprisingly similar between one brand and another.
In the case of implant replacement, this study indicates that it is appropriate to use an implant from the same manufacturer to reproduce the same shape of the breast. On the contrary, the use of an implant of another manufacturer may allow for adjustment in the shape of the breast, particularly at its upper pole, and if needed to improve symmetry. There is, in our opinion, not enough information available about dimensions in the manufacturers’ catalogs to easily evaluate these local shape differences and this work is a first step to clearly demonstrate these differences.
It is acknowledged that this study is not an in vivo examination of implant shapes. It could obviously also be argued that even form stable implants have a certain plasticity and that the actual shape of the implant alters somewhat once implanted, something that naturally also would influence the clinical outcome. This factor is apparent during capsular contracture and even if form stable highly cohesive silicone implants resist deformation much more than low cohesive fillers, they can still be deformed if the capsular activity is strong.
Implant Stiffness Analysis
To the best of our knowledge, there no standardized tests to accurately measure the stiffness of the silicone gel-filled breast implants. Methods exist to quantify the cohesivity of filling gels, but this setting alone does not quantify the stiffness of the implants which also depends on other aspects such as the nature of the shell or the degree of filling (% of shell volume).
The test we designed was in our opinion a good tool to compare the stiffness of the implants in fixed experimental conditions. Unlike Mentor and Sebbin, Allergan offers 2 levels of gel cohesivity for its anatomical implants whose trade names are “TruForm 2″ (a softer gel) and “TruForm 3″ (a firmer gel). The test we have developed has shown a similar stiffness among the Allergan “TruForm 3″, Mentor, and Sebbin implants. Allergan “TruForm 2″ (previously named “soft touch”) implants are on the contrary significantly more supple. Results from other tests performed on the Allergan and Mentor anatomical implants have been published as gel compression fracture testing, gel elasticity testing (quantifying the ability of the gel to retain its shape under force), shell-gel peel testing (measuring the bond between the gel and the shell), or hydrophobicity testing [22].
The characterization of the mechanical properties of the silicone gel-filled breast implants remains in our opinion not sufficiently standardized, making comparison of the biomechanical analysis results of the different published studies difficult. Surgeons have mainly relied on imaging [41] or manual palpation and examination to judge the cohesivity of different implants. One example of such a test, is known as the ‘tilt test’ where the top of an anatomical implant is free hanging in the hand and then tilted upward while the examiner observes the stability of the upper pole of the implants [43]. An industry standard describing the degree of implant stability and cohesivity would be welcome to guide surgeons.
Conclusions
Our work highlighted major and significant differences in shell texture topographies among the different manufacturers, each texture having its own “microscopic signature”. However, we did not find statistically significant differences in cell adhesion among the different textures. We pointed out a smaller size of the open wells for the Biocell® texture when compared with data from earlier studies. For the first time this “change” is described, and it may have important clinical implications (rotation, double capsule…). Pore size dimensions should be evaluated with further studies comparing older, and more recent Allergan’s textured implants, in order to verify the reality of Danino’s findings or to confirm the modification of texture.
Our study also describes for the first time the texture of Sebbin anatomically shaped implants.
There are considerable differences in “anatomical shapes” (especially the projection of the upper pole) among manufacturers and this fact should be kept in mind when changing an implant from one manufacturer for another, despite similar dimensions, which is quite counterintuitive.
Further studies are needed to confirm the clinical consequences of the intermanufacturer differences observed in this experimental study.
References
Brown MH, Shenker R, Silver SA (2005) Cohesive silicone gel breast implants in aesthetic and reconstructive breast surgery. Plast Reconstr Surg 116(3):768–779
Barnsley GP, Sigurdson LJ, Barnsley SE (2006) Textured surface breast implants in the prevention of capsular contracture among breast augmentation patients: a meta-analysis of randomized controlled trials. Plast Reconstr Surg 117(7):2182–2190
Niechajev I, Jurell G, Lohjelm L (2007) Prospective study comparing two brands of cohesive gel breast implants with anatomic shape: 5-year follow-up evaluation. Aesthetic Plast Surg 31(6):697–710
Poeppl N, Schreml S, Lichtenegger F, Lenich A, Eisenmann-Klein M, Prantl L (2007) Does the surface structure of implants have an impact on the formation of a capsular contracture? Aesthetic Plast Surg 31(2):133–139
Hall-Findlay EJ (2011) Breast implant complication review: double capsules and late seromas. Plast Reconstr Surg 127(1):56–66
Mazzocchi M, Dessy LA, Carlesimo B, Marchetti F, Scuderi N (2010) Late seroma formation after breast surgery with textured silicone implants: a problem worth bearing in mind. Plast Reconstr Surg 125(4):176e–177e
Colville RJI, McLean NR, Cross PA (2003) Double capsule or capsule within a capsule: is there a difference? Br J Plast Surg 56(7):724
Brody GS, Deapen D, Taylor CR, Pinter-Brown L, House-Lightner SR, Andersen JS et al (2015) Anaplastic large cell lymphoma occurring in women with breast implants: analysis of 173 cases. Plast Reconstr Surg 135(3):695–705
Mazzocchi M, Dessy LA, Corrias F, Scuderi N (2012) A clinical study of late seroma in breast implantation surgery. Aesthetic Plast Surg 36(1):97–104
Santanelli di Pompeo F, Laporta R, Sorotos M, Di Napoli A, Giovagnoli MR, Cox MC et al (2015) Breast implant-associated anaplastic large cell lymphoma: proposal for a monitoring protocol. Plast Reconstr Surg 136(2):144e–151e
Héden P (2011) Breast augmentation with anatomic, high-cohesiveness silicone gel implants (European Experience). In: Spear S (ed) Surgery of the Breast: Principles and Art, 3rd edn. Wolters Kluwer/Lippincott Williams & Wilkins, Philadelphia, pp 1322–1345
Tebbetts JB, Adams WP (2006) Five critical decisions in breast augmentation using five measurements in 5 minutes: the high five decision support process. Plast Reconstr Surg 118(Supplement):35S–45S
Tebbetts JB (2002) A system for breast implant selection based on patient tissue characteristics and implant-soft tissue dynamics. Plast Reconstr Surg 109(4):1396–1409 discussion 1410–5
Hidalgo DA (2000) Breast augmentation: choosing the optimal incision, implant, and pocket plane. Plast Reconstr Surg. 105(6):2202–2216discussion 2217–8
Heimann T, Meinzer H-P (2009) Statistical shape models for 3D medical image segmentation: a review. Med Image Anal 13(4):543–563
Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, Gee JC et al (2006) User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. NeuroImage. 31(3):1116–1128
Kinney BM, Jeffers LLC, Ratliff GE, Carlisle DA (2014) Silicone gel breast implants: science and testing. Plast Reconstr Surg 134:47S–56S
Paek LS, Tétreault-Paquin JO, St-Jacques S, Nelea M, Danino MA (2013) Le microscope électronique à balayage environnemental est-il un outil pertinent pour l’analyse des capsules périprothétiques mammaires ? Ann Chir Plast Esthét. 58(3):201–207
Barr S, Hill E, Bayat A (2009) Current implant surface technology: an examination of their nanostructure and their influence on fibroblast alignment and biocompatibility. Eplasty. 9:e22
Danino AM, Basmacioglu P, Saito S, Rocher F, Blanchet-Bardon C, Revol M et al (2001) Comparison of the capsular response to the Biocell RTV and Mentor 1600 Siltex breast implant surface texturing: a scanning electron microscopic study. Plast Reconstr Surg 108(7):2047–2052
Danino A, Rocher F, Blanchet-Bardon C, Revol M, Servant JM (2001) A scanning electron microscopy study of the surface of porous-textured breast implants and their capsules. Description of the “velcro” effect of porous-textured breast prostheses. Ann Chir Plast Esthét. 46(1):23–30
Giot J-P, Paek LS, Nizard N, El-Diwany M, Gaboury LA, Nelea M et al (2015) The double capsules in macro-textured breast implants. Biomaterials 23(67):65–72
Hedén P, Jernbeck J, Hober M (2001) Breast augmentation with anatomical cohesive gel implants: the world’s largest current experience. Clin Plast Surg 28(3):531–552
Hedén P, Boné B, Murphy DK, Slicton A, Walker PS (2006) Style 410 cohesive silicone breast implants: safety and effectiveness at 5 to 9 years after implantation. Plast Reconstr Surg 118(6):1281–1287
Bobyn JD, Wilson GJ, MacGregor DC, Pilliar RM, Weatherly GC (1982) Effect of pore size on the peel strength of attachment of fibrous tissue to porous-surfaced implants. J Biomed Mater Res 16(5):571–584
Valencia-Lazcano AA, Alonso-Rasgado T, Bayat A (2013) Characterisation of breast implant surfaces and correlation with fibroblast adhesion. J Mech Behav Biomed Mater 21:133–148
Maxwell GP, Gabriel A (2014) The Evolution of Breast Implants: Plast Reconstr Surg. 134:12S–17S
Brohim RM, Foresman PA, Hildebrandt PK, Rodeheaver GT (1992) Early tissue reaction to textured breast implant surfaces. Ann Plast Surg 28(4):354–362
Abramo AC, De Oliveira VR, Ledo-Silva MC, De Oliveira EL (2010) How texture-inducing contraction vectors affect the fibrous capsule shrinkage around breasts implants? Aesthetic Plast Surg 34(5):555–560
Hammond DC, Migliori MM, Caplin DA, Garcia ME, Phillips CA (2012) Mentor Contour Profile Gel Implants: clinical Outcomes at 6 Years. Plast Reconstr Surg 129(6):1381–1391
Maxwell GP, Scheflan M, Spear S, Nava MB, Hedén P (2014) Benefits and limitations of macrotextured breast implants and consensus recommendations for optimizing their effectiveness. Aesthetic Surg J Am Soc Aesthetic Plast Surg. 34(6):876–881
Derby BM, Codner MA (2015) Textured silicone breast implant use in primary augmentation: core data update and review. Plast Reconstr Surg 135(1):113–124
Sampaio Góes JC (2010) Breast implant stability in the subfascial plane and the new shaped silicone gel breast implants. Aesthetic Plast Surg 34(1):23–28
Maxwell GP, Van Natta BW, Murphy DK, Slicton A, Bengtson BP (2012) Natrelle style 410 form-stable silicone breast implants: core study results at 6 years. Aesthetic Surg J Am Soc Aesthetic Plast Surg. 32(6):709–717
Góes JCS, Landecker A (2003) Optimizing outcomes in breast augmentation: seven years of experience with the subfascial plane. Aesthetic Plast Surg 27(3):178–184
Macadam SA, Clugston PA, Germann ET (2004) Retrospective case review of capsular contracture after two-stage breast reconstruction: is colonization of the tissue expander pocket associated with subsequent implant capsular contracture? Ann Plast Surg 53(5):420–424
Liu X, Zhou L, Pan F, Gao Y, Yuan X, Fan D (2015) Comparison of the postoperative incidence rate of capsular contracture among different breast implants: a cumulative meta-analysis. PLoS One 10(2):e0116071
Wiener TC (2008) Relationship of incision choice to capsular contracture. Aesthetic Plast Surg 32(2):303–306
Jacobson JM, Gatti ME, Schaffner AD, Hill LM, Spear SL (2012) Effect of incision choice on outcomes in primary breast augmentation. Aesthetic Surg J Am Soc Aesthetic Plast Surg. 32(4):456–462
Ben Amar M, Wu M, Trejo M, Atlan M (2015) Morpho-elasticity of inflammatory fibrosis: the case of capsular contracture. J R Soc Interface R Soc. 201:12
Calobrace MB, Capizzi PJ (2014) The Biology and Evolution of Cohesive Gel and Shaped Implants. Plast Reconstr Surg. 134:6S–11S
Nipshagen MD, Beekman WH, Esmé DL, de Becker J (2007) Anatomically shaped breast prosthesis in vivo: a change of dimension? Aesthetic Plast Surg 31(5):540–543
Tebbetts JB (2000) Patient acceptance of adequately filled breast implants using the tilt test. Plast Reconstr Surg 106(1):139–147 discussion 148–9
Acknowledgments
Per Hedén is a regular consultant for ALLERGAN for breast and face. None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Atlan, M., Bigerelle, M., Larreta-garde, V. et al. Characterization of Breast Implant Surfaces, Shapes, and Biomechanics: A Comparison of High Cohesive Anatomically Shaped Textured Silicone, Breast Implants from Three Different Manufacturers. Aesth Plast Surg 40, 89–97 (2016). https://doi.org/10.1007/s00266-015-0603-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-015-0603-8