
Abstract
Purpose
Extracorporeal shockwave therapy (ESWT) has become a common practice for treating knee osteoarthritis (OA). However, the effectiveness and safety of this treatment are still questionable. This meta-analysis is aimed at determining the degree of pain reduction and functional outcome after ESWT for knee OA.
Methods
We systematically searched MEDLINE, EMBASE, and other online databases. The articles comparing the outcomes between ESWT and controls were included in the analysis.
Results
Nine studies with 705 patients were included. The pooled data revealed significantly lower pain scores in the ESWT groups than in the control groups within two weeks of treatment and six months after treatment (visual analogue scale, − 1.59, p = 0.0003, 95% confidence interval (CI) − 2.45 to − 0.72 at 2 weeks; − 1.12, p = 0.005, 95% CI − 1.89 to − 0.34 at 6 months). The ESWT group also had better functional outcomes four to six weeks post treatment (Western Ontario and McMaster Universities Osteoarthritis Index, − 11.96, p = 0.003, 95% CI − 19.76 to − 4.15). No rebound pain was noted for up to 12 months.
Conclusion
Using ESWT to treat knee OA may reduce pain and improve functional outcomes. The effect may last six months to one year. More prospective studies are needed to investigate the settings for ESWT to optimize treatment results.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) is a common disease that results in disability among older people, and the prevalence is increasing [1]. The burden of knee OA on individuals, health systems, and social care systems is considered by many to be a public health crisis [2]. In addition to its significant negative impact on health-related quality of life [3], knee OA may partially account for increased mortality [4]. Most risk factors are comorbid conditions related to reduced levels of physical activity [4], which highlights the importance of knee OA treatment and early rehabilitation.
There are several kinds of treatments for knee OA, which vary from pharmacotherapy to physiotherapy or surgery. Low-impact aerobic exercise and weight control are essential [5, 6]. Acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used for disease control. However, serious adverse events, including gastrointestinal ulcers, bleeding, toxicity, and cardiovascular side effects, are always of concern [7]. In addition to oral medications, intra-articular injections of corticosteroid, hyaluronic acid (HA), or platelet-rich plasma (PRP) are also common for treating knee OA. Corticosteroid injection may relieve pain in the short term [8]. The outcomes of intra-articular injection of HA and PRP are still much debated [9, 10]. Other conventional therapies, such as acupuncture, moxibustion, cupping therapy [11], and laser therapy [12], are used for treating knee OA physically, but their effectiveness for long-term pain control is still questioned. Nevertheless, surgical intervention might be the final choice for severe knee OA that cannot be solved by any of the methods mentioned above [13]. Recently, extracorporeal shockwave therapy (ESWT) was reported to have good results for treating knee OA [14]. It provided another alternative for the treatment of knee OA.
Extracorporeal shock waves represent a nonsurgical and noninvasive intervention using acoustic high-pressure waves generated by electrohydraulic, electromagnetic, piezoelectric, or ballistic/radial methods [15,16,17]. This method causes interstitial and extracellular responses leading to tissue regeneration [18]. Experimental studies in animal models showed that ESWT was effective in treating disabling pain associated with primary knee OA [19, 20]. Some studies have demonstrated that ESWT protects against articular cartilage degradation and improves subchondral bone remodeling in rats [19]. Another study showed the immunochemical effect of ESWT on reducing the progression of OA [20]. Clinical outcomes of ESWT for treating human knee OA have been reported, but the results are controversial [14, 21,22,23,24,25,26,27]. Some articles have indicated that ESWT may be effective and safe [14, 16, 21, 25, 26]. Another report showed that ESWT may increase vascular activity at the target site and improve function in chronic stroke patients with OA [23]. However, some articles have reported no benefits after ESWT treatment [16]. The optimal energy level and length of treatment period have also not been established [16, 21].
To determine the effectiveness of ESWT, we conducted a meta-analysis (MA) to compare the clinical outcomes of ESWT with those of conventional therapies for treating knee OA.
Methods
This study was accomplished using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist.
Eligibility criteria
We collected articles with the following inclusion criteria: (1) the study dealt with knee OA patients treated with ESWT, (2) the study contained a comparison of ESWT and other treatments or placebo controls, (3) pain relief and functional outcomes were primary outcomes of the study, and (4) the study was a randomized controlled trial or cohort study.
Information source and search
We systematically searched MEDLINE via PubMed (2007~2018), EMBASE via OVID (2007~2018), and the Cochrane Central Register of Controlled Trials (CENTRAL) (2014~2017) without any restriction in language for published original articles. We used a search strategy of free text terms and MeSH terms relevant to ESWT, knee, and OA. We searched for the following terms: “extracorporeal shock wave therapy” [MeSH Terms]+OR+“shock wave therapy” [MeSH Terms]+OR+“ESWT” [MeSH Terms])+AND +(“Osteoarthritis” [MeSH Terms] +OR+“OA” [MeSH Terms])+AND +(“knee” [MeSH Terms]). The reference lists of the relevant articles were also searched for any other associated studies.
Study selection
After screening the titles and abstracts of the identified articles, we obtained the full-text article of any potentially included study for further assessment. Studies that did not meet all criteria were excluded. The methodological quality of each included article was assessed by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. The searching of relevant studies and processing of paper exclusions were executed by two authors (C.-K.H., C.-J.C.) independently. Data extraction and article appraisal were conducted by two authors (C.-K.H., T.-W.T.). When discrepancies occurred, consensus was reached via discussion within the review team.
Data collection process
We extracted the data from the articles and contacted the authors of the studies for any missing data or further information. From eligible articles, we collected data on study characteristics (sample size, number of treatment groups, study design, follow-up duration), participant demographics (sex, age, baseline of disease severity), interventions (type, dose, intensity, and duration of treatment), and outcome measures (baseline and follow-up results), as well as information needed to assess the risk of bias and methodological quality of the study.
Statistical analysis
We summarized the outcomes by using variance-weighted means. We evaluated the presence of heterogeneity with the use of a standard χ2 test (with a level of significance of p = 0.01) and the I2 statistic. An I2 statistical value of more than 50% indicated substantial heterogeneity. We used random-effects analysis to compare trials showing heterogeneity and fixed-effects analysis to compare trials without heterogeneity. We calculated the mean difference or relative risk for all outcomes. The meta-analysis was carried out using the RevMan 5 software package (Cochrane Collaboration, Oxford, UK).
Results
Study selection
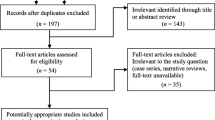
We found 57 potentially relevant articles in the initial search of the various databases. All of the articles were screened by reading the titles and abstracts. After removing the duplicates and non-eligible studies, we found nine articles fulfilling the predefined selection criteria for our analysis (Fig. 1).

Flow chart of the search for articles and trial assessment
Characteristics of the included articles
These nine studies represented a total of 705 participants. Of these patients, 332 received ESWT for treatment of knee OA, and the remaining373received a control treatment. The length of follow-up time in the studies ranged from four to 48 weeks. The sample sizes ranged from 18 to 126 patients. Two studies assessed patients with knee OA over Kellgren-Lawrence (K-L) grade I [22, 23]. One study included K-L grade II knee OA only [25]. Three studies analyzed patients with knee OA over K-L grade II [16, 26, 27]. One study included patients with Altman III knee OA [24]. The severity of knee OA was not available in two studies [14, 21].
The outcomes were measured by several scales. Seven articles reported using the visual analogue pain scale (VAS) [16, 22,23,24,25,26,27]. Seven articles reported the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) for pain and functional outcomes [14, 16, 21, 22, 25,26,27]. The characteristics and methodological quality of the included studies are shown in Table 1. Baseline characteristics were not reported completely in two studies, which could potentially bias the results and limit the generalizability of the findings [24, 25]. Table 2 shows the detailed management of the ESWT and control groups.
Outcomes of ESWT for knee OA
Most studies demonstrated decreased VAS scores and improvement in functional outcomes four to six weeks after ESWT for knee OA. Three studies provided data from 6 months after treatment, and two provided data from 12 months after treatment. The long-term results were controversial. (Fig. 2a and b).

Outcomes of a visual analogue scale (VAS) and b Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) after extracorporeal shockwave therapy (ESWT) in the included studies
Immediate results (within 2 weeks)
Three of the 9 included studies provided data on pain level (VAS) within two weeks of ESWT. Three studies showed that ESWT significantly decreased the VAS score [16, 22, 24]. The pooled data revealed a significantly lower VAS level in the ESWT group than in the control groups within two weeks of ESWT (− 1.59, p = 0.0003, 95% confidence interval (CI) − 2.45 to − 0.72, random-effects model) (Fig. 3a).

Comparison of visual analogue scale (VAS) (a) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (b) between the extracorporeal shockwave therapy (ESWT) groups and control groups 2 weeks post treatment
Two articles reported immediate functional outcomes (WOMAC) within 2 weeks of ESWT. One study showed significantly more improvement in the WOMAC level in the ESWT group than in the alprostadil-treated group [22], but the other study only showed slightly better WOMAC levels in the ESWT group than the laser group [21]. The pooled data only showed a trend towards lower WOMAC scores in the ESWT group within 2 weeks of ESWT. No significant difference between the ESWT and control groups was found (− 10.28, p = 0.31, 95% CI − 29.98 to 9.42, random-effects model) (Fig. 3b). Lack of more data made the results controversial in this time point.
Short-term results (4–6 weeks post intervention)
Four of the nine included studies provided data on pain level (VAS) within four to six weeks of ESWT. Two studies showed that the ESWT groups had significantly greater decreases in the VAS level than the control groups [22, 25]. The other two studies showed controversial results [23, 26]. The pooled data revealed a trend favoring the use of ESWT in the VAS score results (− 1.54, p = 0.07, 95% CI − 3.22 to 0.14, random-effects model) (Fig. 4a). However, HA injection seemed to have similar pain reduction with ESWT. After the exclusion of hyaluronic acid injection group, the pooling data showed that ESWT had greater reduction of VAS than the control groups. (− 2.45, p < 0.001, 95% CI − 2.96 to − 1.95, fixed-effects model, not shown in the figure).

Comparison of visual analogue scale (VAS) (a) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (b) between the extracorporeal shockwave therapy (ESWT) groups and control groups 4 to 6 weeks post treatment
Five articles reported short-term functional outcomes (WOMAC) within four to six weeks of ESWT. Four studies showed significantly more improvement in WOMAC levels after ESWT [14, 21, 22, 25]. One article stated that ESWT and hyaluronic acid injection had equal WOMAC scores [26]. The pooled data showed a significantly greater decrease in the WOMAC scores within four to six weeks of ESWT than that in the control groups (−11.96, p = 0.003, 95% CI: −19.76 to −4.15, random-effect model) (Fig. 4b).
Long-term results (6–12 months post intervention)
Three of the 9 included studies provided data on pain level (VAS) at 6 months following ESWT. Two studies showed that the effect of ESWT on pain reduction was better than in the controls [22, 24], and the other study also had a trend favouring ESWT [27]. The pooled data revealed a significantly greater decrease in the VAS level of the ESWT group than of the control group at six months post intervention (− 1.12, p = 0.005, 95% CI − 1.89 to − 0.34, random-effects model) (Fig. 5a).

Comparison of visual analogue scale (VAS) (a) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (b, c) between the extracorporeal shockwave therapy (ESWT) groups and control groups six to 12 months post treatment
Two articles reported long-term functional outcomes (WOMAC) 6 to 12 months after ESWT. Kang et al. showed a significant improvement in WOMAC levels at six and 12 months after ESWT [22], and the results were also better than those of the control group. Ediz et al. [27] also showed a trend towards functional improvements after ESWT compared with baseline data. However, the results were only slightly better in the ESWT group than in the control group. Pooled data showed no significant difference between the ESWT and control groups in terms of WOMAC 6 and 12 months after treatment (− 8.27, p = 0.1, 95% CI − 18.12 to 1.58, at six months; − 7.10, p = 0.15, 95% CI − 16.79 to 2.59, at 12 months, random-effects model) (Fig. 5b and c).
Minor complications occurred after ESWT, such as transient soft tissue swelling and minor bruising. The patients had no clinically detectable neuromuscular, systemic, or device-related adverse effects after ESWT [14, 22, 24].One of the 82 patients treated with ESWT plus alprostadil experienced complications of painful bone marrow oedema [22].
Discussion
The most important finding of this meta-analysis was that ESWT was an effective treatment for knee OA. ESWT relieved knee pain immediately, within two weeks after treatment. The effect lasted for at least six months. ESWT also improved functional outcomes for patients with knee OA. The pooled results showed significantly improved WOMAC scores four to six weeks after ESWT. These trends continued for one year. There was no serious adverse effect reported in any of the included articles. ESWT can be considered a choice of treatment for patients suffering from knee OA.
ESWT first evokes compression during the positive phase and then tensile force as well as shear stress in the negative phase, which may lead to microbubbles in liquid molecules and may exert cavitational effects on the focal area of the treatment. These complex types of mechanical forces collectively stimulate biophysical effects on the target tissues [28]. Histologically, ESWT enhances subchondral bone anabolism and improves trabecular microarchitecture [19, 29]. According to immunohistochemical analysis, ESWT results in the decline of carboxy-terminal telopeptides of type II collagen (CTX-II) concentration and matrix metalloproteinases (MMP) expression of knee OA in rats, which indicates a decrease in cartilage catabolism [19]. Some studies have claimed that the IL-10 and TNF-alpha production of osteoarthritic chondrocytes returns to normal levels after ESWT [30]. A decreased level of cytokines, such as NO, IL-1, and IL-7, which mediate the inflammatory response, may also induce disease-modifying effects within the osteoarthritic joint [20]. Moreover, ESWT increases vascularization and osteogenesis, indicative of bone remodeling, by increasing BMP-2, VEGF, and von Willebrand factor (vWF) [29]. ESWT also reduced the ratio of calcitonin gene-related peptide (CGRP)–positive dorsal ganglion root neurons in an OA model, suggesting its involvement in joint pain sensation [31].
The pooled data of the immediate outcomes within two weeks of ESWT showed significantly decreased VAS levels and a trend towards functional improvement. These results suggest that ESWT not only reduces pain soon after treatment but also may improve physical function. A possible mechanism is that the pulse of energy from ESWT increases blood flow [25], relieves stiffness, and alters the transmission of pain signals [31]. More data were required to demonstrate the effect of ESWT in this time point.
Four to six weeks after ESWT, the pain continued to decrease, and functional outcome continued to improve. ESWT reduced pain greater than other controls and seemed equal to the effect of HA injection. At this time point, the functional results of the ESWT group were significantly better than those of the other treatment groups. The pooled WOMAC score decreased by − 11.96 in the patients treated with ESWT compared with the score of the controls. These outcomes indicate a significant improvement in the short-term results of ESWT. A 16.0% reduction of the total WOMAC score from baseline was associated with the highest degree of improvement in the transition scale category [32]. In the short-term data, four out of five studies showed over 16.0% reduction of the total WOMAC score of the ESWT patients compared with that of the controls, which indicated significant and obvious clinical improvement.
Six months after the initial treatment, we found a significant mean difference (− 1.12) in the VAS level from the pooled data of the ESWT groups compared with that of the other controls. This result confirms that ESWT has a better ability to alleviate pain than a control treatment after six months of therapy.
Compared with other treatments, ESWT showed similar results in terms of pain and functional outcome in the long term (6 months to 1 year). Although there was a trend favouring better improvement among the ESWT groups, the difference in the pooled outcomes did not reach statistical significance. However, the pain improvement and functional outcomes after ESWT treatment were still better than those at baseline at six months and one year after ESWT. The results in the included articles show that ESWT may have better outcomes than sham procedures or ultrasound after six months and one year [24, 27] but have similar results to intravenous injection of the anti-inflammatory agent alprostadil [22].
In addition to conservative therapy, some studies used alternative treatments for the comparison groups. Li et al. [21] applied a calibrated laser device with five points on the medial side and four points on the lateral side on the 45 patients in their control group. The measured output energy was 0.2 J/point for a total dose of 20Jper treatment per knee. Compared with laser therapy, ESWT showed a greater effect on symptom relief and functional improvement at weeks six and 12 (P < 0.01) post treatment. In another study [26], the control group received intra-articular HA injection s(20 mg/2 mL) weekly for three weeks. Both the ESWT and HA groups had improved VAS scores, WOMAC scores, Lequesne index, 40-metre fast-paced walk test, and a timed stair climb test. However, there were no significant differences between the two groups.
According to the included articles, the ESWT protocol was set to 0.03~0.44 mJ/mm2 with 1000~4000 impulses per unit of time. These protocols yielded good functional outcomes and pain reduction. However, the optimal settings remained unclear. More studies are required to clarify this issue.
There are some limitations to our meta-analysis. First, we could only include published studies. There might be some nonpublished studies with negative results for ESWT. They might bias our results. Second, the size from each individual study was small, and some were not randomized controlled trials. However, after pooling the data from each study, this study was the largest scale meta-analysis to date. We evaluated the methodology of each study. The meta-analysis method partially diminished the bias and provided useful information in this study. The variety of treatment methods used in the control groups in each article might also have biased the results. In addition to sham ESWT, the other control treatments reported included ultrasound, laser therapy, anti-inflammatory medication, and hyaluronic acid injection. However, we believe that comparisons with other treatments are a better way to investigate the effect of ESWT rather than comparing it only with sham procedures. It helped us not overestimate the effect of ESWT on the treatment of knee OA.
In conclusion, this meta-analysis showed that using ESWT for treating knee OA reduced pain and improved functional outcomes. The effect may last six months to one year. More prospective studies with large sample sizes are needed to investigate the best ESWT settings for optimizing treatment results.
References
Sacks JJ, Luo YH, Helmick CG (2010) Prevalence of specific types of arthritis and other rheumatic conditions in the ambulatory health care system in the United States, 2001-2005. Arthritis Care Res 62(4):460–464. https://doi.org/10.1002/acr.20041
White PH, Waterman M (2012) Making osteoarthritis a public health priority. Am J Nurs 112(3 Suppl 1):S20–S25. https://doi.org/10.1097/01.NAJ.0000412647.18173.62
Farr Ii J, Miller LE, Block JE (2013) Quality of life in patients with knee osteoarthritis: a commentary on nonsurgical and surgical treatments. Open Orthop J 7:619–623. https://doi.org/10.2174/1874325001307010619
Hochberg MC (2008) Mortality in osteoarthritis. Clin Exp Rheumatol 26(5 Suppl 51):S120–S124
Iwamoto J, Sato Y, Takeda T, Matsumoto H (2011) Effectiveness of exercise for osteoarthritis of the knee: a review of the literature. World J Orthop 2(5):37–42. https://doi.org/10.5312/wjo.v2.i5.37
Bliddal H, Leeds AR, Christensen R (2014) Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes Rev 15(7):578–586. https://doi.org/10.1111/obr.12173
Gutthann SP, García Rodríguez LA, Raiford DS (1997) Individual nonsteroidal antiinflammatory drugs and other risk factors for upper gastrointestinal bleeding and perforation. Epidemiology 8(1):18–24
Ayhan E, Kesmezacar H, Akgun I (2014) Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J Orthop 5(3):351–361. https://doi.org/10.5312/wjo.v5.i3.351
Glynn LG, Mustafa A, Casey M, Krawczyk J, Blom J, Galvin R, Hannigan A, Dunne CP, Murphy AW, Mallen C (2018) Platelet-rich plasma (PRP) therapy for knee arthritis: a feasibility study in primary care. Pilot Feasibility Stud 4:93–93. https://doi.org/10.1186/s40814-018-0288-2
Altman R, Hackel J, Niazi F, Shaw P, Nicholls M (2018) Efficacy and safety of repeated courses of hyaluronic acid injections for knee osteoarthritis: a systematic review. Semin Arthritis Rheum 48(2):168–175. https://doi.org/10.1016/j.semarthrit.2018.01.009
Zhang Y, Huang L, Su Y, Zhan Z, Li Y, Lai X (2017) The effects of traditional Chinese exercise in treating knee osteoarthritis: a systematic review and meta-analysis. PLoS One 12(1):e0170237. https://doi.org/10.1371/journal.pone.0170237
Huang Z, Chen J, Ma J, Shen B, Pei F, Kraus VB (2015) Effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthr Cartil 23(9):1437–1444. https://doi.org/10.1016/j.joca.2015.04.005
Steinhaus ME, Christ AB, Cross MB (2017) Total knee arthroplasty for knee osteoarthritis: support for a foregone conclusion? HSS J 13(2):207–210. https://doi.org/10.1007/s11420-017-9558-4
Lizis P, Kobza W, Manko G (2017) Extracorporeal shockwave therapy vs. kinesiotherapy for osteoarthritis of the knee: a pilot randomized controlled trial. J Back Musculoskelet Rehabil 30(5):1121–1128. https://doi.org/10.3233/BMR-169781
Schmitz C, Császár NBM, Milz S, Schieker M, Maffulli N, Rompe J-D, Furia JP (2015) Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions: a systematic review on studies listed in the PEDro database. Br Med Bull 116(1):115–138. https://doi.org/10.1093/bmb/ldv047
Imamura M, Alamino S, Hsing WT, Alfieri FM, Schmitz C, Battistella LR (2017) Radial extracorporeal shock wave therapy for disabling pain due to severe primary knee osteoarthritis. J Rehabil Med 49(1):54–62. https://doi.org/10.2340/16501977-2148
Ogden JA, Toth-Kischkat A, Schultheiss R (2001) Principles of shock wave therapy. Clin Orthop Relat Res 387:8–17. https://doi.org/10.1097/00003086-200106000-00003
Wang C-J (2012) Extracorporeal shockwave therapy in musculoskeletal disorders. J Orthop Surg Res 7(1):11. https://doi.org/10.1186/1749-799X-7-11
Wang C-J, Hsu S-L, Weng L-H, Sun Y-C, Wang F-S (2013) Extracorporeal shockwave therapy shows a number of treatment related chondroprotective effect in osteoarthritis of the knee in rats. BMC Musculoskelet Disord 14:44–44. https://doi.org/10.1186/1471-2474-14-44
Zhao Z, Ji H, Jing R, Liu C, Wang M, Zhai L, Bai X, Xing G (2012) Extracorporeal shock-wave therapy reduces progression of knee osteoarthritis in rabbits by reducing nitric oxide level and chondrocyte apoptosis. Arch Orthop Trauma Surg 132(11):1547–1553. https://doi.org/10.1007/s00402-012-1586-4
Li W, Pan Y, Yang Q, Guo Z-G, Yue Q, Meng Q-G (2018) Extracorporeal shockwave therapy for the treatment of knee osteoarthritis: a retrospective study. Medicine 97(27):e11418. https://doi.org/10.1097/MD.0000000000011418
Kang S, Gao F, Han J, Mao T, Sun W, Wang B, Guo W, Cheng L, Li Z (2018) Extracorporeal shock wave treatment can normalize painful bone marrow edema in knee osteoarthritis: a comparative historical cohort study. Medicine 97(5):e9796. https://doi.org/10.1097/MD.0000000000009796
Cho SJ, Yang JR, Yang HS, Yang H-E (2016) Effects of extracorporeal shockwave therapy in chronic stroke patients with knee osteoarthritis: a pilot study. Ann Rehabil Med 40(5):862–870. https://doi.org/10.5535/arm.2016.40.5.862
Chen TW, Lin CW, Lee CL, Chen CH, Chen YJ, Lin TY, Huang MH (2014) The efficacy of shock wave therapy in patients with knee osteoarthritis and popliteal cyamella. Kaohsiung J Med Sci 30(7):362–370. https://doi.org/10.1016/j.kjms.2014.03.006
Lee J-H, Lee S, Choi S, Choi Y-H, Lee K (2017) The effects of extracorporeal shock wave therapy on the pain and function of patients with degenerative knee arthritis. J Phys Ther Sci 29(3):536–538. https://doi.org/10.1589/jpts.29.536
Lee J-K, Lee B-Y, Shin W-Y, An M-J, Jung K-I, Yoon S-R (2017) Effect of extracorporeal shockwave therapy versus intra-articular injections of hyaluronic acid for the treatment of knee osteoarthritis. Ann Rehabil Med 41(5):828–835. https://doi.org/10.5535/arm.2017.41.5.828
Levent (2018) <L.pdf>. doi:https://doi.org/10.31086/tjgeri.2018344054
Ji Q, Wang P, He C (2016) Extracorporeal shockwave therapy as a novel and potential treatment for degenerative cartilage and bone disease: osteoarthritis. A qualitative analysis of the literature. Prog Biophys Mol Biol 121(3):255–265. https://doi.org/10.1016/j.pbiomolbio.2016.07.001
Wang CJ, Sun YC, Wong T, Hsu SL, Chou WY, Chang HW (2012) Extracorporeal shockwave therapy shows time-dependent chondroprotective effects in osteoarthritis of the knee in rats. J Surg Res 178(1):196–205. https://doi.org/10.1016/j.jss.2012.01.010
Moretti B, Iannone F, Notarnicola A, Lapadula G, Moretti L, Patella V, Garofalo R (2008) Extracorporeal shock waves down-regulate the expression of interleukin-10 and tumor necrosis factor-alpha in osteoarthritic chondrocytes. BMC Musculoskelet Disord 9:16–16. https://doi.org/10.1186/1471-2474-9-16
Ochiai N, Ohtori S, Sasho T, Nakagawa K, Takahashi K, Takahashi N, Murata R, Takahashi K, Moriya H, Wada Y, Saisu T (2007) Extracorporeal shock wave therapy improves motor dysfunction and pain originating from knee osteoarthritis in rats. Osteoarthr Cartil 15(9):1093–1096. https://doi.org/10.1016/j.joca.2007.03.011
Hmamouchi I, Allali F, Tahiri L, Khazzani H, Mansouri LE, Ali Ou Alla S, Abouqal R, Hajjaj-Hassouni N (2012) Clinically important improvement in the WOMAC and predictor factors for response to non-specific non-steroidal anti-inflammatory drugs in osteoarthritic patients: a prospective study. BMC Res Notes 5:58–58. https://doi.org/10.1186/1756-0500-5-58
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Chi-Kun Hsieh, Zhao-Wei Liu, Chao-Jui Chang, and Ta-Wei Tai. The first draft of the manuscript was written by Chi-Kun Hsieh, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hsieh, CK., Chang, CJ., Liu, ZW. et al. Extracorporeal shockwave therapy for the treatment of knee osteoarthritis: a meta-analysis. International Orthopaedics (SICOT) 44, 877–884 (2020). https://doi.org/10.1007/s00264-020-04489-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-020-04489-x