
Abstract
Purpose
Cross-sectional diameter of 7 mm or more of graft in anterior cruciate ligament reconstruction is arguably the single most important factor determining the success of the operation. Pre-operative anthropometric parameters have been reported to correlate with diameter of quadrupled hamstring graft, which is the most popular graft choice today. We conducted this prospective study to determine the value of some anthropometric measurements to predict the length of harvested semitendinosus and gracilis tendons and quadrupled hamstring graft diameter. We also assessed the reliability of the mathematical equation in accurately predicting the graft diameter.
Methods
Height, weight, BMI and thigh length of 160 patients who underwent primary ACL reconstruction was measured before surgery. Using multivariate logistic regression analysis length of harvested semitendinous and gracilis tendons along with quadrupled graft diameter were correlated to height, weight, BMI and thigh length.
Results
Ninety-six percent had graft diameter of 7 mm or more. Height and thigh length were found to be most strongly correlating to both the length of harvested tendons and the quadrupled graft diameter (p ≤ 0.001, r = 0.25–0.39). Patients with height less than 147 cm were found to be at highest risk for inadequate graft diameter (less than 7 mm). Although the anthropometric parameters were found to be significantly related to height and thigh length, the strength of association is moderate. The mathematical equation for prediction of graft diameter using height was found to inaccurately over-predict the graft diameter in 33.1 % of cases, assessed using Bland-Altman plot.
Conclusion
Anthropometric parameters, especially height and thigh length, can serve as a guide to plan hamstring graft diameter and length before ACL reconstruction. But, it is not advisable to rely on mathematical equations for absolute values of graft parameters as there is risk of over-estimating hamstring length or graft thickness.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The quadrupled hamstring autograft has gained popularity for the anterior cruciate ligament (ACL) reconstruction procedure due to fewer incidences of patello-femoral problems that are encountered in bone–patella tendon–bone grafts (BPTB) [1–6]. The quadrupled semitendinosus and gracilis tendon graft provides comparable stiffness and tensile properties in addition to better cosmesis and excellent clinical outcome when compared to BPTB [1–6]. Although recent studies also show that there is no difference in functional outcomes and laxity when using either type of graft in female patients or when used for revision surgery, the choice of graft may depend on surgeon preference with hamstring graft being more popular among the two [7, 8]. The normal ACL is about 11 mm in thickness in an adult, and for reconstruction a graft no less than 7 mm is recommended, as the graft strength is known to be related to the cross-sectional diameter and revision surgery rate [9, 10]. However, unlike BPTB, the semitendinosus and gracilis tendon diameter can neither be consistent nor controlled during harvest. With the increasing demand of patients involved in sports and heavy activities, alternative choice of graft, fixation technique or additional post may be required in situations where hamstring graft is found to be inadequate. Studies in the past have thus attempted to predict pre-operatively the adequacy of such quadrupled hamstring graft. Pre-operative parameters such as age, gender, height, weight, BMI, leg length, thigh circumference, etc., have been reported to be of predictive value in a variety of studies but there is poor consensus [11–18]. Magnetic resonance, 3D tomography, and USG have also been employed to improve the accuracy of pre-operative prediction of hamstring tendon graft harvest data [19–21]. Few studies have reported height of the patient to correlate with graft diameter and length and also derived a mathematical equation to predict the adequacy of graft, but reproducibility of this has not been proved [11–13, 16, 18]. Moreover, with the graft diameters being measured in value increments of 0.5 mm during sizing, the reliability of these mathematical equations, which are based on continuous numeric data, needs to be questioned. Few studies have looked at the length of hamstring tendon at harvest, but either for triplication of semitendinosus or for double bundle ACL reconstruction [22, 23]. We conducted this prospective study to determine the value of these anthropometric measurements in our population to predict the length of harvested tendons and quadrupled hamstring graft diameter. We also assessed the reliability of a mathematical equation in accurately predicting the graft diameter.
Material and methods
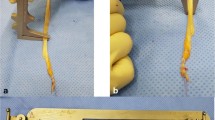
After obtaining institutional review committee approval and informed written consent we included 160 patients in our study during the period from 2010 to 2012. All patients had isolated ACL injury and no revision cases were included. We obtained anthropometric measurements including height, weight, and thigh length (anterior superior iliac spine; ASIS to medial joint line) preoperatively and length of semitendinosus, gracilis and quadrupled hamstring graft diameter were measured during the surgery. Both semitendinosus and gracilis tendon were harvested by a single surgeon from the ipsilateral limb through standard vertical incision of 3 cm length at the distal attachment of the tendons and harvested in identical fashion. The lengths of the tendons were measured using a standard mathematical metal scale after removing all muscle fibres and final trimming of the tendons. The ends were whip-stitched with polyester suture and both tendons were doubled up at the middle to obtain a four-strand graft. The graft was passed through the Smith & Nephew sizing cylinder of 0.5 mm increments and the minimum diameter that allowed smooth passage of the entire graft completely was taken as the graft diameter. The femoral tunnel was of the same diameter as that of the graft which was drilled via antero-medial portal for anatomic single bundle ACL reconstruction. Both femur and tibial end fixation techniques were the same in all cases.
Statistical analysis
BMI for patients was calculated by standard formula using height and weight. Single linear regression was applied to obtain correlation coefficients (Pearsons r) of the anthropometric data and identify the relationship to the intra-operative measurements of the graft lengths and diameter. Multiple stepwise regression analysis was performed to exclude confounding variables and explain variance to obtain a predictive equation for the diameter and length outcome.
We also obtained the predicted value of ACL diameter for our patients according to the formulae in literature, and the agreement of the values of predicted to true graft diameter was studied using Bland-Altman plot. The error rate for predictive accuracy was also calculated. All data were analysed using commercial statistical package SPSS (Version 16, SPSS Inc, Chicago, IL) for MS-Windows. A p-value ≤ 0.05 was considered statistically significant during the analysis.
Results
This prospective study included 160 subjects of both gender. All patients included were beyond skeletal maturity. The means and SD of pre-operative anthropometric data included height (169.1 ± 6.9 cm), weight (69.2 ± 11.7 kg), BMI (24.1 ± 3.5) and thigh length (51.5 ± 3.5 cm) (Table 1). After harvest and preparation the measurements of hamstring tendons were: gracilis length (27.5 ± 2.8 cm), semitendinosus length (29.2 ± 3.0 cm) and quadrupled graft diameter (7.7 ± 0.6 mm). Ninety-one (56.9 %) had graft diameter more than or equal to 8.0 mm, whereas 64 (40.0 %) and 5 (3.1 %) had graft diameter of 7–8 mm and less than 7 mm, respectively (Table 2). We used the equation derived by Tuman et al. which was Graft diameter = 2.4 + 0.03 (height in cm) and calculated the expected graft diameter for our patients. More than 95 % patients were predicted to have graft diameter of above 7.0 mm, which on comparison to the true diameter measured during surgery revealed that about 33 % had diameter less than the predicted diameter by at least 0.5 mm (Table 3).
Assessment of correlation coefficients revealed moderate association between height, weight, and thigh length of subjects to the quadrupled graft diameter although BMI had no statistical significant relationship (Table 4, Fig. 1). On multiple stepwise regression analysis weight and thigh length also fell out of favour and only height showed a significant association to the graft diameter in our study population and the following equation was derived for our sample: Graft diameter (mm) = 2.14 + 0.033 (height; cm), which closely matches the one derived by Tuman et al. Using this equation we calculated that our patients with height less than 147 cm are at risk of quadrupled graft diameter of less than 7 mm.

Correlations of quadrupled hamstring diameter to height (r = 0.358, p <0.001), weight (r = 0.245, p < 0.002), thigh length (r = 0.253, p = 0.001) and BMI (r = 0.087, p = 0.272); (N = 160)
Similarly, the gracilis and semitendinosus graft lengths were also assessed using single linear and multiple regression analysis (Table 4, Fig. 2), and a predictive equation was calculated. However, in all these equations the strength of association is only moderate (R² < 0.20) as only 20 % of variance is explained by the parameter. Both gracilis and semitendinosus showed moderate association with height and thigh length with R² being 0.195 and 0.186 for the combined equation as follows:

Correlation of semitendinosus length to height (r = 0.398, p <0.001) and thigh length (r = 0.350, p < 0.001), and gracilis length to height (r = 0.385, p <0.001) and thigh length (r = 0.386, p < 0.001); (N = 160)
The predicted graft diameter as calculated from the mathematical equation of Tuman et al. was compared to the true graft diameter obtained at the time of surgery, and Bland-Altman graph was plotted (Fig. 3). The correlation coefficient was 0.8279 (p < 0.001) and the slope of the graph was 0.5123 (p < 0.001) showing strong agreement between the two values. As the true graft values can only be calculated in increments of 0.5 mm the predicted values were corrected to next largest graft size assuming that the graft will easily pass through only the sizing cylinder of the next size (e.g. 7.34 mm predicted graft will pass through size 7.5 mm cylinder). This was then compared to the true graft values for each and 33.1 % of grafts were found to have size smaller than the predicted diameter. The equation could not predict graft size less than 7 mm or more than 8.0 mm (Table 3).

Bland-Altman plot of the predicted graft diameter to actual graft diameter. Correlation R = 0.8279 (p < 0.001); Slope = 0.5123 (p < 0.001); Intercept = 7.47 (p < 0.001)1); (N = 160)
Discussion
Quadrupled hamstring graft is the most commonly utilized substitute for ACL reconstruction. Knowing the diameter and lengths of the hamstring graft pre-operatively can be helpful in surgical planning. Anthropometric data like age, gender, height, weight, BMI, leg length, thigh circumference and parameters like sporting activity have been studied in the past and different authors have reported differences in each of these factors as having predictive value for quadrupled graft diameter (summary in Table 5). We provide a review of the analysis of these parameters from previous studies and also aim to extrapolate the value of these in our population.
We included 160 adult patients of both gender with isolated ACL tears undergoing primary ACL reconstruction only in our study. Hamstring tendons measurements showed means as follows; gracilis length (27.5 ± 2.8 cm), semitendinosus length (29.2 ± 3.0 cm) and quadrupled graft diameter (7.7 ± 0.6 mm). Ninety-one (56.9 %) had graft diameter more than or equal to 8.0 mm, whereas 64 (40.0 %) and 5 (3.1 %) had graft diameter of 7–8 mm and less than 7 mm, respectively (Table 2).
Using the equation by Tuman et al. for predicting graft diameter, more than 95 % of patients were predicted to have graft diameter of above 7.0 mm [11]. On comparison to the true diameter measured during surgery it was noted that about 33 % had diameter less than the predicted diameter by at least 0.5 mm (Table 3).
Moderate association (R² up to 0.128) was found to height, weight, and thigh length of subjects to the quadrupled graft diameter although BMI had no statistical significant relationship (Table 4, Fig. 1). On multiple stepwise regression analysis however weight and thigh length also fell out of favour and only height (p < 0.001) showed a significant association to the graft diameter in our study.
Similarly, the gracilis and semitendinosus graft lengths were also assessed using single linear and multiple regression analysis (Table 4, Fig. 2) and a predictive equation was calculated. However, in all these equations the strength of association is only moderate (R² < 0.20) as only 20 % of variance is explained by any of these parameters.
Although predicted graft diameter using height as suggested by equation from Tuman et al. showed strong agreement with the actual graft diameter among our patients we found it to be unreliable. As the clinical values are only possible in increments of 0.5 mm, the actual graft size in 33.1 % subjects were found to be less than predicted diameter. The equation also could not predict sizes of less than 7 mm or above 8 mm, which shows its limited importance in cases beyond usual 7–8 mm sized grafts.
We found that the anthropometric characteristics of our population (mean of height, weight, BMI and graft diameters in our study; 169.1 ± 6.9 cm, 69.2 ± 11.7 kg, 24.1 ± 3.5 and 7.7 ± 0.6 mm) are well matched to previous similar studies [11–13, 15–18]. No study in the past has also shown a very strong correlation (R² < 0.20) with any of the parameters when multiple stepwise regression analysis was performed [11, 13, 16–18]. The most consistent parameter in most of these studies is the height [11–18]. In our data set we found the height to be significantly valuable (p < 0.001) in predicting the graft diameter but the strength of this correlation was moderate (R² = 0.128; explains 12.8 % variance in diameter due to height). Magnussen and colleagues studied 265 patients who underwent primary ACL reconstruction with hamstring autograft for risk factors associated with subsequent revision and found younger age and smaller graft diameter as greatest risk factor for early revision surgery [8]. They reported a revision rate of 13.6 % in patients with initial graft size of 7 mm or less in comparison to about 5 % with 7.5 mm or more [8]. When keeping 7 mm or less initial graft diameter as ‘at risk’ for revision in our regression equation we noted that our patients with height less than 147 cm were at risk of yielding final quadrupled autograft of less than 7 mm. Tuman et al. proposed the same threshold for height in their study which was followed up by Treme and colleagues, who further reduced the height for risk of graft less than 7 mm to 140 cm, although both mentioned that this remained more significant for females [11, 12]. Ma et al. [14] and Pinheiro et al. [17] also noted height to be a factor affecting graft diameter for both men and women although women had significantly smaller grafts in their study compared to men and they did not propose a threshold of height for inadequate graft. The findings of Boisvert et al. suggested a much taller population statistic with height less than 162.5 cm in women to be a risk for quadrupled graft less than 7 mm but they could not apply it in males; in contrast, Celiktas and colleagues [16, 18] proposed 155.2 cm as a height threshold for the men in their study. In Schwartzberg’s study only the height fell out of favour in predicting graft diameter, and although Loo et al. also rejected the predictive usefulness of height, theirs was an all Asian male population [13, 15]. Thus height probably still remains as the most consistent parameter to predict small hamstring graft and patients less than about 150 cm in most populations to be at highest risk.
Treme et al. prospectively evaluated the work of Tuman and colleagues to suggest weight and BMI explain about 40 % of variance in graft diameter. They suggested BMI less than 18 kg/m² was a risk factor for graft thickness less than 7 mm, but did not comment on multiple regression analysis [11, 12]. Also BMI of less than 18 kg/m² alone could not predict graft of less than 7 mm among 24 patients in their series. Boisvert et al. supported greater BMI predicting thicker graft diameter in males but not a lower BMI resulting in smaller graft [16]. Other studies have also mixed results with weight and BMI correlates to graft diameter and may not have clinical relevance in predicting graft diameter as BMI in fact cannot distinguish between lean muscle and fat.
The mean weight and thigh length of our data set (69.2 ± 11.7 kg, 51.5 ± 3.5 cm) although did have a significant correlation (p < 0.01), but we do not propose them to be of importance as they fell out of the equation in multiple stepwise regression analysis and only explained about 6 % (R² = 0.06) variance by themselves.
Adding to the list of other parameters like leg length, thigh circumference and thigh length, which have been varyingly reported in past literature, our study also showed significant (p < 0.001) correlation to graft thickness but again the independent strength of this association was weak (R² = 0.064).
Hamstring tendon length becomes important when (1) triplicated tendon is required in order to increase graft diameter, (2) longer graft length is needed for augmenting fixation by a post, (3) single bundle augmentation is planned using only one of the hamstring tendons, (4) combined reconstructions for multi-ligament injury is to be considered, or (5) double bundle ACL reconstruction is required [22–25]. Few studies have correlated anthropometric parameters to length of hamstring tendons with ACL graft length of about 8–10 cm (4 cm intra-articular and 2–3 cm on either side in femur and tibia tunnel) being necessary for stable fixation during surgery and good tendon to bone contact for healing [12, 13, 22, 23]. To increase diameter of graft triplication of either tendon may be required and length of 24–30 cm of harvested tendons is necessary.
In our study the mean length of ST and gracilis tendons were 29.2 ± 3.0 and 27 ± 2.8 cm, respectively. We found that for ST and gracilis length, height and thigh length (ASIS to MJL) are important predictors (p < 0.001, R² = 0.12–0.15) with the following regression equations:
We are able to suggest that this puts patients with height less than 171.1 cm and with thigh length less than 33.1 cm at risk for shorter hamstring tendon which could allow either tendon to be triplicated if diameter of quadrupled graft is inadequate. This supports the previous studies by Treme et al. and Schwartzberg who also reported that the graft length is related to leg length and height [12, 13].
These variables have however been only assessed for accuracy by Treme and colleagues in their prospective study of 50 patients where they reported 6.7 % error rate in predicting graft diameter calculated by an equation suggested by a previous study by the same team [11, 13]. We obtained a mathematical equation of height with graft diameter which resembles quite closely the one derived from the data set of Tuman et al. and used it to predict the graft diameter for our set of patients. The mean of the predicted graft thickness (7.4 ± 0.2) had significant agreement with the actual graft thickness (7.7 ± 0.6) according to Bland-Altman plot (p < 0.001) (Figs. 3 and 4). All the predicted graft diameters were between 7 and 8 mm (Table 2) although we had 23 (14.3 %) patients who had graft diameter on either side of the range predicted by the equation. Five (3.1 %) patients had true graft thickness less than the safe limit of 7 mm even though their heights (152–164.5 cm) were more than the height at risk (147 cm). On further analysis we found that one-third (33.1 %) of the patients actually had graft size less than predicted. Thus even though there is agreement on the mean of graft thickness the equation is not able to predict the grafts at risk and may over-estimate graft size in up to one-third of patients when using height to determine actual value of graft diameter.

Correlation between true quadrupled graft diameter and predicted diameter (N = 160)
We did not include age, gender or sporting activity in our analysis as they have been repeatedly refuted as significant parameters in previous studies [12–16].
Conclusion
Anthropometric parameters are easy and relevant in planning hamstring graft in ACL reconstruction surgery. Height of the patient has repeatedly shown to be of importance in predicting graft thickness but the absolute graft diameter may be over-predicted by equations giving false sense of security to the surgeon. Any data set of patients which show correlation to a parameter is exclusive for that set and should not be extrapolated to all. A single, long, harvested hamstring tendon may possibly be adequate when considering single bundle reconstruction or performing combined reconstruction of multi-ligament injury. Tripled or quadrupled tendon would have a good diameter in itself making length of the tendon an important consideration. Short patients (less than 150 cm) are not only at risk of thinner graft but also shorter tendon length in situations where triplication of tendon or longer tail to augment fixation may be necessary. We recommend relying on height and to a lesser extent on thigh length only as a guide to surgical planning but not depend on mathematical equations in literature to give absolute values of hamstring length or graft thickness. There still remain a lot of parameters like ethnicity, growth pattern, diet and nutrition, etc. to be studied which will help us to predict accurately the characteristics of hamstring graft.
References
Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC (1999) Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 81:549–557
Pinczewski LA, Lyman J, Salmon LJ, Russell VJ, Roe J, Linklater J (2007) A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: a controlled, prospective trial. Am J Sports Med 35:564–574. doi:10.1177/0363546506296042
Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F (2004) Anterior cruciate ligament reconstruction: bone–patellar tendon–bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am 86:2143–2155
Maletis GB, Cameron SL, Tengan JJ, Burchette RJ (2007) A prospective randomized study of anterior cruciate ligament reconstruction: a comparison of patellar tendon and quadruple-strand semitendinosus/gracilis tendons fixed with bioabsorbable interference screws. Am J Sports Med 35:384–394. doi:10.1177/0363546506294361
Williams RJ III, Hyman J, Petrigliano F, Rozental T, Wickiewicz TL (2005) Anterior cruciate ligament reconstruction with a four-strand hamstring tendon autograft. Surgical technique. J Bone Joint Surg Am 87:51–66
Pichler W, Tesch NP, Schwantzer G et al (2008) Differences in length and cross-section of semitendinosus and gracilis tendons and their effect on anterior cruciate ligament reconstruction: a cadaver study. J Bone Joint Surg (Br) 90:516–519. doi:10.1302/0301-620x.90b4.19994
Kautzner J, Kos P, Hanus M, Trc T, Havalas V (2015) A comparison of ACL reconstruction using patellar tendon versus hamstring autograft in female patients: a prospective randomised study. Int Orthop 39:125–130. doi:10.1007/s00264-014-2495-7
Mahmoud SS, Odak S, Coogan S, McNicholas MJ (2014) A prospective study to assess the outcomes of revision anterior cruciate ligament reconstruction. Int Orthop 38:1489–1494. doi:10.1007/s00264-014-2324-z
Hamada M, Shino K, Horibe S et al (2005) Changes in cross-sectional area of hamstring anterior cruciate ligament grafts as a function of time following transplantation. Arthroscopy 21:917–922
Magnussen RA, Lawrence JT, West RL et al (2012) Graft size and patient age are predictors of early revision after anterior cruciate ligament reconstruction with hamstring autograft. Arthroscopy 28:526–531. doi:10.1016/j.arthro.2011.11.024
Tuman JM, Diduch DR, Rubino LJ, Baumfeld JA, Nguyen HS, Hart JM (2007) Predictors for hamstring graft diameter in anterior cruciate ligament reconstruction. Am J Sports Med 35:1945–1949. doi:10.1177/0363546507304667
Treme G, Diduch DR, Billante MJ, Miller MD, Hart JM (2008) Hamstring graft size prediction: a prospective clinical evaluation. Am J Sports Med 36:2204–2209. doi:10.1177/0363546508319901
Schwartzberg R, Burkhart B, Lariviere C (2008) Prediction of hamstring tendon autograft diameter and length for anterior cruciate ligament reconstruction. Am J Orthop 37:157–159
Ma CB, Keifa E, Dunn W, Fu FH, Harner CD (2010) Can pre-operative measures predict quadruple hamstring graft diameter? Knee 17:81–83. doi:10.1016/j.knee.2009.06.005
Loo W et al (2010) Can we predict ACL hamstring graft sizes in the Asian male? A clinical relationship study of anthropometric features and 4-strand hamstring graft sizes. Malays Orthop J 4:9–12. doi:10.5704/MOJ.1007.001
Boisvert CB, Aubin ME, DeAngelis N (2011) Relationship between anthropometric measurements and hamstring autograft diameter in anterior cruciate ligament reconstruction. Am J Orthop 40:293–295
Pinheiro LF Jr, de Andrade MA, Teixeira LE, Bicalho LA, Lemos WG, Azeredo SA et al (2011) Intra-operative four-stranded hamstring tendon graft diameter evaluation. Knee Surg Sports Traumatol Arthrosc 19:811–815. doi:10.1007/s00167-010-1387-7
Celiktas (2013) Prediction of the quadruple hamstring autograft thickness in ACL reconstruction using anthropometric measures. Acta Orthop Traumatol Turc 47:14–18
Yasumoto M, Deie M, Sunagawa T, Adachi N, Kobayashi K, Ochi M (2006) Predictive value of 3-dimensional computer tomography measurement of semitendinosus tendon harvested for anterior cruciate ligament reconstruction. Arthroscopy 22:259–264
Bickel BA, Fowler TT, Mowbray JG, Adler B, Klingele K, Phillips G (2008) Preoperative magnetic resonance imaging cross-sectional area for the measurement of hamstring autograft diameter for reconstruction of the adolescent anterior cruciate ligament. Arthroscopy 24:1336–1341. doi:10.1016/j.arthro.2008.07.012
Erquicia J, Gelber PE, Doreste JL et al (2013) How to improve the prediction of quadrupled semitendinosus and gracilis autograft sizes with magnetic resonance imaging and ultrasonography. Am J Sports Med 41:1857–1863. doi:10.1177/0363546513479340
Schwartzberg RS (2014) Prediction of semitendinosus and gracilis tendon lengths and diameters for double bundle ACL reconstruction. Am J Orthop 43:E1–E6
Challa S, Satyaprasad J (2013) Hamstring graft size and anthropometry in south Indian population. J Clin Orthop Trauma 4:135–138. doi:10.1016/j.jcot.2013.09.005
Lorenz S, Ahrens P, Kirchhoff S, Wolf P, Hinterwimmer S, Obermeir A, Beirer M, Kirchhoff C (2015) Dynamic quantification of tibio-femoral rotation in postero-lateral bundle insufficiency of the anterior cruciate ligament: a cadaver study. Int Orthop 39:865–870. doi:10.1007/s00264-014-2537-1
Helito CP, Bonadio MB, Demange MK, da Mota E, Albuqerque RF, Pécora JR, Camanho GL, Angelini FJ (2015) Functional assessment of combined reconstruction of the anterior cruciate ligament and posterolateral corner with a single femoral tunnel: a two-year minimum follow-up. Int Orthop 39:543–548. doi:10.1007/s00264-014-2576-7
Conflict of interest
The authors declare that they have no conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Goyal, S., Matias, N., Pandey, V. et al. Are pre-operative anthropometric parameters helpful in predicting length and thickness of quadrupled hamstring graft for ACL reconstruction in adults? A prospective study and literature review. International Orthopaedics (SICOT) 40, 173–181 (2016). https://doi.org/10.1007/s00264-015-2818-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2818-3