
Abstract
Purpose
Anterior cruciate ligament (ACL) injury represents one of the most common diagnoses in orthopaedic sports medicine. In the past, anatomic knowledge about the different bundles within the cruciate ligaments triggered new treatment concepts, such as double-bundle ACL reconstruction. Recently, besides complete tearing, partial ACL ruptures and bundle augmentation became a focus. However, only little is known regarding rotational stability of the knee with an isolated torn postero-lateral (PL) bundle. Therefore, the aim of the present study was the torsiometric analysis of tibio-femoral restraint patterns of the PL-insufficient knee joint.
Methods
Fresh human whole body cadavers were enrolled. After diagnostic arthroscopy to ensure the structural integrity of the cruciate ligaments, knee joints underwent torsiometry at 0°, 30°, and 90° degree flexion. Then stepwise the PL bundle and the anteromedial (AM) bundle were arthroscopically resected, while torsiometry of the PL- as well as of the ACL-deficient knee joints was repeated. An area under the curve (AUC) was calculated. All statistical analyses were conducted using a p-value of 0.05 as level of significance.
Results
The comparison of charged and equilibrated curves during internal rotation revealed significant results at low flexion (30° flexion) angles between the ACL intact versus PL absent conditions (p = 0.04). In addition, charged and equilibrated curves during external rotation at 90° flexion, thus high angles, resulted in a significant difference when comparing the ACL-intact with the PL-deficient condition (p = 0.01).
Conclusions
In the present cadaver study using the Torsiometer tool we found a distinct destabilization of the rotational restraints in full knee extension only after total ACL resection. In contrast, no significant findings resulted after an isolated dissection of the PL bundle during internal deflection. Nevertheless, a significant loss of stability was found during unstressed external deflection after isolated PL bundle dissection. Therefore patients, undergoing PL augmentation might benefit regarding rotational instability patterns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anterior cruciate ligament (ACL) injury represents one of the most common diagnoses in orthopaedic sports medicine [1–5]. Reconstruction techniques have still remained precarious in restoring native knee kinematics due to insufficient rotational stability [6–8].
Anatomic studies have clearly sub-classified multiple anatomical and at least two functional ACL bundles. The antero-medial (AM) and the postero-lateral (PL) bundle have been attributed to diverse stabilizing effects [9, 10]. From the anatomical point of view the AM bundle, being under tension during knee flexion, is supposed to restrict anterior-posterior (AP) translation. In contrast the PL bundle is thought to restrict tibio-femoral rotation [11–13]. Komzak et al. recently evaluated the function of the AM and PL bundles in AP and rotational movement of the knee following single and double bundle ACL repair [14]. They concluded that double bundle repair decreases AP laxity as well as increases rotational stability compared to single-bundle reconstruction [15]. Besides complete tearing, partial ACL ruptures became a focus in the recent past. In the context of double-bundle reconstruction, several authors have reported on ACL augmentation techniques, aiming for the isolated reconstruction of the torn bundle [16] since this is considered to restore AP as well as rotational stability [17].
However, only little is known regarding the influence of an isolated torn PL bundle on rotational stability of the knee, although several authors have reported on devices for assessment of knee stability [18, 19]. In this context, we recently introduced the Torsiometer, a device for the evaluation of the tibio-femoral rotation [20]. The Torsiometer allows for a highly reliable dynamic measurement of internal, external and total rotation and enables the examiner to analyse deflection and torque patterns restraining rotational motion.
Therefore, the aim of the present study was to evaluate the impact of PL bundle insufficiency on tibio-femoral rotation performing a torsiometric analysis.
Material and methods
Specimen
In total 22 knee joints of 11 fresh human whole body cadavers were enrolled. The mean age was 47 ± five years; there were six male and five female donors. The mean body weight was 77 ± 7 kg. Informed consent was given in all cases, either by the donor in life or by a next of kin.
Inclusion criteria were external and internal integrity of the knee, i.e. intact skin, no fractures, no radiological signs of osteoarthritis (OA), no signs of previous knee surgeries, full passive range of motion, clinically intact lateral and medial collateral ligaments (LCL/MCL) and cruciate ligaments (ACL/PCL). To exclude osseous pathologies like previous fractures as well as presence of OA, a computed tomography (CT) scan of each knee was performed prior to the experiments and read by an expert musculoskeletal radiologist (S.K.).
The integrity of the cruciate ligaments was clinically approved by the Lachman and the pivot-shift test [21]. A further inclusion criterion was the arthroscopically proven absence of OA as well as the structural integrity of the cruciate and collateral ligaments, the posterolateral corner as well as the anterolateral capsule.
Study protocol
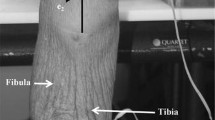
To break the rigor mortis, each cadaveric leg underwent ten cycles of passive maximum knee flexion and extension movements. The lower limb was attached to the Torsiometer, that was validated elsewhere [20]. In brief, the Torsiometer consists of two rigs, connected by a hinge adjusted to the height of the knee joint to enable free knee flexion movements. Two bicortical 4.5-mm Schanz screws (Synthes, Solothurn, Switzerland) were used to create solid conditions between the limb and the device itself (see Fig. 1). Consecutively, the diagnostic arthroscopy was performed.

Bird’s eye view of the study setting. The lower limb is attached to the torsiometer. The torsiometer consists of two rigs, connected by a hinge adjusted to the height of the knee joint to enable free knee flexion movements
Before each measurement cycle started, the device was calibrated with the tibia in a neutral zero position with the second toe pointing forward and performing a full extension movement allowing for free tibial rotation to be able to find the position with the lowest predefined tension. The knee joint is known to have six degrees of freedom during movement. In the method used in the presented study fixing the femur resulted in a single rotational centre in the femur so that measuring AP translation and rotation of the tibia at fixed angles of knee flexion is reasonable. A manual torque was applied via the lever arm to the shank and the corresponding forces as well as rotational angles were registered with a frequency of 33.3 Hz (approximately 360 measuring points/cycle) and counted using the Labview 8.0 software package (National Instruments, Austin, Texas, USA).
Measurements of the ACL intact knee joints were repeated at 0°, 30°, and 90° flexion. The maximum deflection range for the intact ACL knee joint was used as reference value for all further measurements. The applied torque was limited to 10 Newton metres (Nm) in order to prevent nonphysiologic load and consecutive structural tissue damage. Every measurement cycle started with internal rotation up to the end point of 10 Nm, followed by a release back to the zero position. Subsequently, the deflection during external rotation was performed in the same manner. The measurements were divided into four torque patterns: (1) charged internal rotation, (2) equilibrated internal rotation (back to zero position), (3) charged external rotation and (4) equilibrated external rotation (back to zero position).
After the first measurement cycle performed on ACL intact knees, the PL bundle was resected through standard antero-lateral and antero-medial arthroscopic portals using an arthroscopic basket forceps (WideBiter Punch Tip, Arthrex, Naples, USA) and a shaving instrument (Full Radius Resector, Arthrex, Naples, USA). The same measurements as described above were repeated at 0°, 30°, and 90° flexion in the PL-resected knee joints.
Finally the remaining AM bundle was resected and the measurements were repeated at 0°, 30°, and 90° flexion.
In order to assess intra-observer reliability, each measurement was repeated three times. The senior author (C.K.) performed all surgical interventions.
Data processing
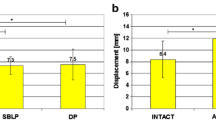
For later analysis, the combinations of the two values in terms of rotation angle and torque moment were transformed into the physical units radiant (rad) and Nm. The value pairs of each measuring point (rad/Nm) generate a graph with an appropriate area under the curve (AUC). The AUC represents the applied physical work in joules (J) and was used to analyse the different restraint situations. The value pairs were assessed for internal and external rotation in 0°, 30° and 90° knee flexion. Figure 2 exemplarily demonstrates an AUC. In addition, the maximum deflection value examining the ACL intact knee was compared to both ACL insufficient knee conditions (PL resected, ACL resected) and deflection degrees comprising the differences of the expended energy expressed in the AUC between the charged and the equilibrated torque curve.

Example of an area under the curve (AUC). The value pairs of each measuring point (rad/Nm) generate a graph with an appropriate AUC, which represents the applied physical work in joules (J). Graphic display of the aligned curves related to ACL intact (solid line), PL resected (broken line) and ACL resected (dotted line) values
Statistical analysis
Statistical analysis was performed using R 2.11.1 (R Foundation for Statistical Computing, Vienna, Austria) and PASW 18.0 (SPSS® Inc., Chicago, IL). Data are given as mean ± standard error. For measuring the physical work expended, the AUC was calculated using the trapezoidal rule. Differences in the work between different ACL conditions were determined using paired sample t-tests. To analyse intra-observer reliability the Pearson correlation coefficient was calculated. All statistical analyses were conducted using a p-value of 0.05 as level of significance.
Results
Torques and corresponding AUCs
Internal rotation
Torsiometric analysis of the intact ACL in internal rotation in 0° flexion revealed an AUC of 1.22 ± 0.19 J for the charged and of 0.97 ± 0.17 J for the equilibrated deflection. After resection of the PL bundle an AUC of 1.16 ± 0.21 J (charged, p = 0.41) and of 0.88 ± 0.16 J (equilibrated, p = 0.1) resulted. Total resection of the ACL revealed an AUC for the charged internal deflection of 0.97 ± 0.13 J (p = 0.01) versus the equilibrated internal deflection of 0.67 ± 0.18 J (p = 0.001). Low flexion of the knee only led to slight changes. AUC of the intact ACL accounted for 1.1 ± 0.11 J in the charged and 0.88 ± 0.16 J in the equilibrated internal deflection. Resection of the PL-bundle effected no changes of the AUC, neither in the charged (p = 0.16) nor the equilibrated situation (0.97). Total resection of the ACL effected no significant changes as well (charged, p = 0.91; equilibrated, p = 0.44). Torsiometry of the knee under a flexion of 90° resulted in significant higher AUC. The torque of the intact ACL was 1.82 ± 0.27 J in the charged and 1.43 ± 0.2 J in the equilibrated internal deflection. Resection of the PL bundle revealed an AUC of 1.86 ± 0.3 in the charged and a significantly lower AUC of 1.33 ± 0.19 (p = 0.08) in the equilibrated internal deflection. The total resection of the ACL did not effect lower torques (charged, 1.87 ± 0.4 J; equilibrated, 1.35 ± 0.34 J). For more details see Table 1, and for details regarding statistical significance see Table 2.
External rotation
AUCs of external deflection in 0° flexion accounted for 1.28 ± 0.1 J (charged) and for 1.01 ± 0.16 J (equilibrated) in ACL intact knee joints. Significantly lower torques were found for equilibrated external deflection after resection of the PL bundle (0.87 ± 0.12 J; p = 0.03). Total resection of the ACL revealed significantly lower torques as well (0.74 ± 0.16 J; p = 0.01). No significant changes were noticed for low flexion of 30°, neither for the charged nor the equilibrated situation (for more details see Table 1).
For high flexion of 90°, significant results were found for the comparison of the intact ACL and the PL resected knee joint under charged conditions (p = 0.03) as well as under equilibrated conditions (p = 0.07) (for more details see Table 1).
Charged vs. equilibrated deflection
When comparing the charged and equilibrated curves during internal rotation, significant results were found at low flexion (30° flexion) angles between the ACL intact versus PL resected condition (p = 0.04). For the comparison of charged and equilibrated curves during external rotation at high 90° flexion angles, significant findings resulted when comparing the ACL intact with the PL resected condition (p = 0.01). For all other comparisons regarding charged versus equilibrated as well as the different ACL conditions, no further significant findings resulted. The results for the comparison of the differences between the charged and equilibrated curves are summarized in Table 1.
The intraobserver reliability was 0.98, which is considered to be high.
Discussion
In the presented cadaver study a hieratic two-dimensional model for rotational knee restraints was created enabling mechanical elimination of AP translation. For quantification of the rotational restraints an AUC was calculated [10, 22]. The main findings of our study were that during full knee extension only the total ACL resection led to a destabilization of the rotational restraints. In contrast, no significant findings resulted after an isolated dissection of the PL bundle during internal deflection. Nevertheless, a significant loss of stability was found during equilibrated external deflection after isolated PL bundle dissection.
These results are in contrast to the work published by Monaco et al. who used a navigation system to measure the subsequently performed resection of the PL-, AM-bundle as well as the lateral collateral ligament (LCL) and the corresponding motion patterns [23]. They reported no increased rotation after PL bundle or total ACL resection performing full extension. This result is interesting since it is known that knee extension as well as knee flexion stresses both bundles. Our results show that the total ACL resection affects the internal rotation restraint during full extension in both the charged and equilibrated deflection. However, we only found significant changes during high knee flexion (90°) and internal rotation for the equilibrated deflection after partial ACL dissection (PL-resected).
In this context also the results of Christel et al. have to be mentioned, who examined the contribution of each ACL bundle to the Lachman test in a cadaver study with a low number of only six specimens [24]. They concluded that the AM bundle significantly contributes to tibial translation during the Lachman test, whereas the PL bundle’s effect is negligible. The authors described that a divided PL bundle had a greater effect on increasing internal rotation of the tibia than the AM bundle even though this contribution was relatively low. Their results coincide with our findings at least in reference to the total ACL resection affecting the internal rotation restraint during full extension in both the charged and equilibrated deflection. However, Christel et al. concluded that isolated PL bundle tears cannot be detected by the Lachman test only since the PL bundle most likely contributes resistance to the pivot shift [24]. For low flexion angles significantly less energy is needed to be able to perform similar deflection grades. The energy expended during internal rotation significantly dropped with the loss of the PL bundle, especially comparing the measurements during 0° and 30° degree knee flexion. Our results during 30° and 90° degree flexion are in accordance with the studies of Furman et al. and Nielsen et al. who also described a decreased restraint in internal rotation in case of partially dissected ACL as well as after total ACL resection [25, 26].
Similar results were also achieved by Komzak et al. who reported in their cadaver study on AM bundle controlling AP and rotational stability to a greater extent than the PL bundle [15]. They performed KT-1000 arthrometer analysis for AP translation and a rolimeter analysis for measuring rotational movements for intact, AM- or PL-bundle insufficient or complete ACL deficient knees. They concluded that the impact of the AM bundle on the AP translation is greater than of the PL bundle in all knee joint flexion angles (30°, 60° ,90°). Thus the PL bundle does not resist the rotational stability more than the AM bundle with the result that the rotational stability is more sufficiently controlled by both ACL bundles as compared to one bundle. The same author group published a clinical study in 2012 (46) on the question whether the PL bundle influences rotational movement more than the AM bundle in ACL reconstruction, examining patients following ACL single and double bundle reconstruction, respectively, performing KT-1000 arthrometer and rolimeter measurements [14]. They reported for the double-bundle reconstruction group that rotation was as much controlled by the AM bundle as in the single bundle group but to a greater extent compared to the PL bundle in the double-bundle technique. The authors also stated that AP translation and rotational stability during internal rotation, not in external rotation, was increased more for the double bundle than for single bundle technique.
These results are in accordance with the presented findings since we described no significant rotational destabilization after PL bundle in internal deflection [14]. From the clinical point of view our findings in terms of distinct rotational destabilization of the knee joint during full extension, only for complete ACL resection without significant findings for the only PL bundle absent situation in internal rotation, emphasize that in case of an ACL rupture either partial or complete patients would rather benefit from the single-bundle technique.
Limitations
For the presented study distinct limitations have to be mentioned. The presented human cadaver approach reflects the complex course of motion of the knee joint and corresponding restraint patterns only partially. Muscular tension and neuromuscular interaction is missing in this experimental setup. Therefore, the complex three-dimensional course of motion of a pivot shift manoeuver was reduced to a hieratic two-dimensional course of motion for measurement of specific rotational restraints. The rotational restraint was measured especially with respect to the two bundles of the ACL.
Another important drawback is the cadaveric nature of our study. Although we used fresh cadavers that underwent a distinct course of mobilization for breaking rigor mortis, it cannot be excluded that our results are influenced by increasing tissue laxity. However, the next step in order to assess the biomechanical role of the different ACL bundles has to be the in vivo analysis.
Conclusion
The dogma of the specific restraints which is attributed to the AM and the PL bundle has to be seen as a simplified model which is adequate to develop scientific questions and hypotheses [27–30]. Although we observed a significant loss of stability during unstressed external deflection after isolated PL bundle dissection, no significant findings resulted after an isolated dissection of the PL bundle during internal deflection. Based on our experimental cadaver study a clinical recommendation regarding advantages of either single bundle or double bundle ACL reconstruction cannot be made.
References
Gianotti SM, Marshall SW, Hume PA, Bunt L (2008) Incidence of anterior cruciate ligament injury and other knee ligament injuries: A national population-based study. J Sci Med Sport 12(6):622–627. doi:10.1016/j.jsams.2008.07.005
Bjordal JM, Arnly F, Hannestad B, Strand T (1997) Epidemiology of anterior cruciate ligament injuries in soccer. Am J Sports Med 25(3):341–345
Bradley JP, Klimkiewicz JJ, Rytel MJ, Powell JW (2002) Anterior cruciate ligament injuries in the National Football League: epidemiology and current treatment trends among team physicians. Arthroscopy 18(5):502–509. doi:10.1053/jars.2002.30649
Ireland ML (1999) Anterior cruciate ligament injury in female athletes: epidemiology. J Athl Train 34(2):150–154
Mountcastle SB, Posner M, Kragh JF Jr, Taylor DC (2007) Gender differences in anterior cruciate ligament injury vary with activity: epidemiology of anterior cruciate ligament injuries in a young, athletic population. Am J Sports Med 35(10):1635–1642. doi:10.1177/0363546507302917
Li X, Xu CP, Song JQ, Jiang N, Yu B (2013) Single-bundle versus double-bundle anterior cruciate ligament reconstruction: an up-to-date meta-analysis. Int Orthop 37(2):213–226. doi:10.1007/s00264-012-1651-1
Muller B, Hofbauer M, Wongcharoenwatana J, Fu FH (2013) Indications and contraindications for double-bundle ACL reconstruction. Int Orthop 37(2):239–246. doi:10.1007/s00264-012-1683-6
Suomalainen P, Kannus P, Jarvela T (2013) Double-bundle anterior cruciate ligament reconstruction: a review of literature. Int Orthop 37(2):227–232. doi:10.1007/s00264-012-1680-9
Petersen W, Zantop T (2007) Anatomy of the anterior cruciate ligament with regard to its two bundles. Clin Orthop Relat Res 454:35–47. doi:10.1097/BLO.0b013e31802b4a59
Zantop T, Herbort M, Raschke MJ, Fu FH, Petersen W (2007) The role of the anteromedial and posterolateral bundles of the anterior cruciate ligament in anterior tibial translation and internal rotation. Am J Sports Med 35(2):223–227. doi:10.1177/0363546506294571
Markolf KL, Mensch JS, Amstutz HC (1976) Stiffness and laxity of the knee—the contributions of the supporting structures. A quantitative in vitro study. J Bone Joint Surg Am 58(5):583–594
Takeda Y, Xerogeanes JW, Livesay GA, Fu FH, Woo SL (1994) Biomechanical function of the human anterior cruciate ligament. Arthroscopy 10(2):140–147
Butler DL, Noyes FR, Grood ES (1980) Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. J Bone Joint Surg Am 62(2):259–270
Komzak M, Hart R, Okal F, Safi A (2012) Does the posterolateral bundle influence rotational movement more than the anteromedial bundle in anterior cruciate ligament reconstruction?: a clinical study. J Bone Joint Surg (Br) 94(10):1372–1376. doi:10.1302/0301-620X.94B10.28673
Komzak M, Hart R, Okal F, Safi A (2013) AM bundle controls the anterior-posterior and rotational stability to a greater extent than the PL bundle—a cadaver study. Knee 20(6):551–555. doi:10.1016/j.knee.2013.03.012
Papalia R, Franceschi F, Zampogna B, Tecame A, Maffulli N, Denaro V (2014) Surgical management of partial tears of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc 22(1):154–165. doi:10.1007/s00167-012-2339-1
Yagi M, Kuroda R, Nagamune K, Yoshiya S, Kurosaka M (2007) Double-bundle ACL reconstruction can improve rotational stability. Clin Orthop Relat Res 454:100–107. doi:10.1097/BLO.0b013e31802ba45c
Alam M, Bull AM, Thomas R, Amis AA (2013) A clinical device for measuring internal-external rotational laxity of the knee. Am J Sports Med 41(1):87–94. doi:10.1177/0363546512469874
Mayr HO, Hoell A, Bernstein A, Hube R, Zeiler C, Kalteis T, Suedkamp NP, Stoehr A (2011) Validation of a measurement device for instrumented quantification of anterior translation and rotational assessment of the knee. Arthroscopy 27(8):1096–1104. doi:10.1016/j.arthro.2011.02.034
Ahrens P, Kirchhoff C, Fischer F, Heinrich P, Eisenhart-Rothe R, Hinterwimmer S, Kirchhoff S, Imhoff AB, Lorenz SG (2011) A novel tool for objective assessment of femorotibial rotation: a cadaver study. Int Orthop 35(11):1611–1620. doi:10.1007/s00264-010-1159-5
Prins M (2006) The Lachman test is the most sensitive and the pivot shift the most specific test for the diagnosis of ACL rupture. Aust J Physiother 52(1):66
Gabriel MT, Wong EK, Woo SL, Yagi M, Debski RE (2004) Distribution of in situ forces in the anterior cruciate ligament in response to rotatory loads. J Orthop Res 22(1):85–89. doi:10.1016/S0736-0266(03)00133-5
Monaco E, Maestri B, Labianca L, Speranza A, Kelly MJ, D'Arrigo C, Ferretti A (2010) Navigated knee kinematics after tear of the ACL and its secondary restraints: preliminary results. Orthopedics 33(10):87–93. doi:10.3928/01477447-20100510-58
Christel PS, Akgun U, Yasar T, Karahan M, Demirel B (2012) The contribution of each anterior cruciate ligament bundle to the Lachman test: a cadaver investigation. J Bone Joint Surg (Br) 94(1):68–74. doi:10.1302/0301-620X.94B1.26562
Furman W, Marshall JL, Girgis FG (1976) The anterior cruciate ligament. A functional analysis based on postmortem studies. J Bone Joint Surg Am 58(2):179–185
Nielsen S, Ovesen J, Rasmussen O (1984) The anterior cruciate ligament of the knee: an experimental study of its importance in rotatory knee instability. Arch Orthop Trauma Surg 103(3):170–174
Messner K, Maletius W (1999) Eighteen- to twenty-five-year follow-up after acute partial anterior cruciate ligament rupture. Am J Sports Med 27(4):455–459
Bak K, Scavenius M, Hansen S, Norring K, Jensen KH, Jorgensen U (1997) Isolated partial rupture of the anterior cruciate ligament. Long-term follow-up of 56 cases. Knee Surg Sports Traumatol Arthrosc 5(2):66–71
Steckel H, Vadala G, Davis D, Musahl V, Fu FH (2007) 3-T MR imaging of partial ACL tears: a cadaver study. Knee Surg Sports Traumatol Arthrosc 15(9):1066–1071. doi:10.1007/s00167-007-0337-5
Yao L, Gentili A, Petrus L, Lee JK (1995) Partial ACL rupture: an MR diagnosis? Skelet Radiol 24(4):247–251
Acknowledgements
We would like to explicitly thank Fritz Seidl, MA Interpreting and Translating, for his excellent language copyediting.
Conflict of interest
This study has been supported by a grant from the Deutsche Arthrose-Hilfe e.V. (Frankfurt am Main, Germany).
There is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Stephan Lorenz and Philipp Ahrens contributed equally to this work.
Rights and permissions
About this article

Cite this article
Lorenz, S., Ahrens, P., Kirchhoff, S. et al. Dynamic quantification of tibio-femoral rotation in postero-lateral bundle insufficiency of the anterior cruciate ligament: a cadaver study. International Orthopaedics (SICOT) 39, 865–870 (2015). https://doi.org/10.1007/s00264-014-2537-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-014-2537-1