
Abstract
Hepatic perfusional changes are common in response to, or as a result of, a multitude of pathological processes. These can be neoplastic, inflammatory, fibrotic, or ischemic in origin, to name a few. The liver, having a dual blood supply, is a unique organ to study using contrast-enhanced CT and MRI imaging due to its varied appearance on multiphasic imaging. Knowledge of the CT and MRI appearance of hepatic perfusional changes, in addition to the clinical presentation, can often result in an accurate differential diagnosis. Many of the conditions that cause these changes in hepatic blood flow result in similar appearances on imaging. As a result, it is important that radiologists be aware of common pitfalls when dealing with hepatic perfusional changes to prevent misdiagnosis or delayed diagnosis. As such, this review will focus on some of the various causes of hepatic perfusional changes and how to accurately identify and diagnose them based on their CT and MRI appearance.
Graphic abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The liver is a unique organ, in that it has a dual blood supply from both the portal vein (75%) and hepatic artery (25%) [1]. These supply systems are not independent of one another and have many connections throughout the liver’s structure [1, 2]. The response of this dual supply system to different liver pathologies can result in a unique imaging appearance of perfusional changes on computed tomography (CT) and magnetic resonance imaging (MRI). These perfusional changes result from alterations in blood flow either directly as a result of the liver pathology or as a secondary response to the liver insult.
Both CT and MR are useful in the assessment of the vasculature of the liver, as well as any alterations in the blood flow in the form of perfusional changes that may occur within this system. The use of rapid image acquisition allows for the hepatic parenchyma to be observed in multiple phases (arterial, portal venous, and delayed) following the injection of intravenous contrast [1]. The appearance of the liver on dynamic contrast-enhanced imaging varies based on increases, decreases, or reversals of flow through both vascular supply systems [2]. These changes can occur due to neoplastic and non-neoplastic processes that can be visualized on cross-sectional imaging.
This pictorial review aims to outline various common and uncommon pathologies that can result in these hepatic perfusional changes, as well as to describe and highlight common pitfalls and tips that can aid radiologists in identifying and accurately diagnosing these conditions.
Vascular etiologies
Nutmeg liver
Nutmeg liver refers to the appearance of the liver on cut sections and on dynamic contrast-enhanced cross-sectional imaging. A nutmeg liver arises in conditions that elevate hepatic venous pressures and can be seen secondary to congestive hepatopathy from congestive heart failure or constrictive pericarditis. In addition, it can be seen secondary to true hepatic venous occlusion in the setting of Budd–Chiari syndrome and hepatic veno-occlusive disease (discussed below). Radiologically, a nutmeg liver manifests as heterogenous peripheral enhancement in the arterial and portal venous phases before becoming isoattenuating in the delayed phase on CT [3] (Fig. 1). Similar findings are seen on MRI, with heterogeneous peripheral enhancement on the arterial and portal venous phases, with more homogeneous enhancement seen in the delayed phase. This mottled appearance of the liver is due to hepatic venous congestion, which prevents contrast from diffusing normally through the hepatic sinusoids [3]. The hypoattenuating regions on CT and hypointense regions on MRI seen in the arterial and portal venous phases indicate decreased portal venous blood flow and ischemia [3]. As well as sharing similar enhancement characteristics as CT, MR imaging also allows for the visualization of abnormal signal intensity of the background liver parenchyma seen on the non-enhanced MR sequences, particularly T2-weighted images and diffusion-weighted imaging (DWI) [4]. Regions of abnormal increased signal intensity will be seen on these sequences in the periphery of the liver. The distribution will correspond to the regions of abnormal enhancement [4].

A 56-year-old patient with a case of nutmeg liver. Axial and coronal contrast-enhanced CT images in the portal venous phase show heterogenous peripheral enhancement of the liver parenchyma, with otherwise patent vasculature (a–c) (arrows). Follow-up CT shows resolution of the heterogeneous enhancement pattern shown in the previous images with return of the normal homogenous enhancement of the liver parenchyma (d)
Budd–Chiari syndrome
Budd–Chiari syndrome (BCS) occurs due to impediment of hepatic venous or IVC outflow [5] (Fig. 2). In the acute stage, the characteristic pattern of enhancement in the portal venous phase is a mottled appearance of the liver parenchyma with central enhancement and peripheral hypoenhancement (nutmeg liver) [5]. The lack of enhancement in the periphery is due to stasis or reversal of flow within the portal vein and sinusoidal pathways with non-opacification of the hepatic veins. In the arterial phase, there is more central hepatic enhancement that is most pronounced within the caudate lobe [5]. On the portal venous and delayed phase images, there is reduced enhancement centrally with progressive accumulation of contrast in the periphery (flip–flop sign). This enhancement pattern is seen on both CT and MRI. As well, in the setting of BCS, the hepatic parenchyma can show decreased T1 signal centrally with a slight increase in intensity on T2-weighted sequences [5]. In the chronic stage, hepatic parenchymal atrophy with relative sparing of the caudate lobe and intrahepatic collaterals are often visible on both CT and MR [5]. In addition, regenerative nodules may be seen on cross-sectional imaging. As well, compensatory enlargement of the hepatic artery gradually develops in the chronic stage, while the stasis within the portal vein may produce secondary portal venous thrombosis [5]. There are a number of acquired causes of BCS, including sepsis, oral contraceptive use, sickle cell disease, antiphospholipid syndrome, and tumor invasion. Concurrent portal vein thrombosis may also be seen. As well, there are some congenital causes of BCS, including hepatic vein or IVC webbing, absence of the suprahepatic IVC (Fig. 3), and interruption of the diaphragm.

A 59-year-old patient with Budd–Chiari syndrome. Contrast-enhanced CT images in the portal venous phase show inhomogeneous mottled appearance of the liver parenchyma with preserved central enhancement and peripheral geographic regions of hypoenhancement due to reversal of flow in the portal vein with non-enhancement of the occluded hepatic veins (a–c) (arrows). An occluded right hepatic vein is best seen on the coronal image (c star)

A 61-year-old patient with Budd–Chiari syndrome and absence of the suprahepatic IVC. Axial and coronal contrast-enhanced CT images of the liver in the portal venous phase show patchy parenchymal enhancement with poor visualization of the hepatic veins (a, b) (arrows). A truncated IVC with no suprahepatic segment is noted (b star). Axial and coronal contrast-enhanced MRI images show similar patchy enhancement as CT (c, d) (arrows). A truncated IVC with no suprahepatic segment is also noted (d star)
Hepatic veno-occlusive disease
Hepatic veno-occlusive disease (HVOD), which has been more recently called hepatic sinusoidal obstruction syndrome (HSOS), occurs secondary to occlusion of the sublobular hepatic veins or central veins of hepatic lobules leading to sinusoidal congestion with postsinusoidal portal hypertension [6]. This is distinguished from BCS in that the large hepatic veins remain patent. Radiologically, it is characterized by inhomogeneous enhancement of the liver parenchyma with patchy hypoattenuation in the portal venous phase (nutmeg liver) [6] (Fig. 4). On MR, patchy areas of increased signal intensity on T2-weighted imaging can be seen. Additional features include hepatomegaly, ascites, and gallbladder wall edema [6]. HVOD can be seen secondary to toxic injury to liver sinusoids in the setting of graft-versus-host disease in patients post stem-cell transplant, oral contraceptives, radiation therapy, chemotherapy, as well as in response to certain naturally occurring toxins. Distinguishing HVOD from BCS can be challenging on imaging alone, with the main distinction being small but patent large hepatic veins. However, the relevant clinical history and, in some cases, tissue sampling are needed to make the distinction [6].

A 60-year-old patient with history of HIV, Syphilis, prior renal transplant and elevated LFTs. Axial contrast-enhanced CT in the portal venous phase shows patchy enhancement of the liver parenchyma (a arrows). Incidental liver cyst also noted (star). Axial and coronal T2-weighted MR shows patchy geographic regions of increased signal intensity in the periphery of the liver (b, c) (arrows). There is mottled enhancement in the periphery of the liver on the axial T1-weighted post-contrast image (d arrows). The areas of enhancement show no mass-like features and demonstrate a feathery appearance on both CT and MRI. The overall appearance is suggestive of HVOD, which was pathologically proven
Portal vein thrombosis
Portal vein thrombosis (PVT) most often occurs in the setting of existing liver cirrhosis and portal hypertension [7] (Fig. 5). In the setting of PVT, there is increased peripheral enhancement in the arterial and early portal phases on CT and MRI before returning to iso-density/iso-intensity in the portal venous phase [7]. These are known as transient hepatic enhancement differences (THEDs) and are seen in conditions that result in reduced portal flow leading to compensatory flow from the hepatic arteries. Compression of the liver parenchyma by masses or normal structures such as diaphragmatic slips can reduce portal venous flow focally and result in THEDs as well [7]. Occasionally, occlusion of segmental branches of the portal veins occurs, which is often embolic in nature, frequently seen after bowel surgery or in cases of septic thrombophlebitis affecting mesenteric veins. In the presence of a perfusional abnormality, it is crucial to look for tubular filling defects in the liver to assess for occluded portal venous branches and to differentiate them from dilated bile ducts (Fig. 5d, e). One of the challenges with characterizing PVT is distinguishing bland from tumor thrombus, both of which can be seen in the setting of malignancy such as hepatocellular carcinoma (HHC). The main distinguishing feature is the presence of enhancement within the intraluminal thrombus and/or extension of the enhancing thrombus beyond the vessel wall. Chronically, a thrombosed portal vein undergoes cavernous transformation, which appears as a conglomerate of collateral vessels that bypass the region of occlusion [7]. Cavernous transformation can occur within days of PVT but it does not alter the THED enhancement pattern mentioned previously [7].

A 73-year-old patient with Doppler ultrasound showing complete occlusion of the expanded portal vein with no flow evident (a star). Axial contrast-enhanced CT imaging in the arterial phase shows increased peripheral geographic patches of relative hyperenhancement in segments of the liver previously supplied by the portal vein in keeping with THEDs (b arrows). The late portal venous phase shows more homogeneous enhancement throughout the liver parenchyma (c). Segmental occlusion of the portal vein leads to the appearance of patchy peripheral enhancement in the arterial phase (THEDs) that predominates in the right lobe of the liver (d arrows) with return to isoattenuation in the portal venous phase (e); an occluded segmental portal vein branch is also noted (e arrow). Cavernous transformation becomes evident with the appearance of vessels that bypass the occlusion within the portal vein in the arterial and portal venous phases (f, g) (stars) with the THEDs still present (arrows)
Hepatic infarction
Hepatic infarction is relatively uncommon due to the dual blood supply of the liver and the large number of collaterals that exist within its structure [8]. Liver infarction can occur if both the hepatic arterial supply and the portal venous flow are compromised. However, most cases are seen secondary to acute portal venous flow compromise. Radiologically, hepatic infarcts appear as geographic and often wedge-shaped areas of non-enhancing hepatic parenchyma in the arterial phase on both CT and MRI [1] (Fig. 6). There can also be small regions of reduced enhancement and hypoattenuation in the portal venous phase [1]. Relatively low T1 signal intensity and high T2 signal intensity can also be seen on MRI. There are a number of possible causes of hepatic infarction, which include occlusive causes such as bland or tumor thrombus, embolic disease, vasculitis (polyarteritis nodosa), sickle cell disease, and iatrogenic/post-operative occlusion as seen in cases of liver transplant. Non-occlusive causes include trauma, shock, hypercoagulable state, and eclampsia [8]. Some of the mimics of hepatic infarction include a true liver mass or abscess, as well as focal hepatic fatty infiltration.

A 44-year-old patient presented with hepatic infarction, which was determined to be secondary to Antiphospholipid Syndrome. The axial CT imaging in the portal venous phase at presentation shows a wedge-shaped region of non-enhancing liver parenchyma (a arrow). A follow-up CT 2 weeks later shows expansion of this region of non-enhancement to encompass the majority of the left lobe of the liver in the arterial (b) and portal venous phase (c) (arrows) with delayed enhancement of a wedge of parenchyma in the portal venous phase (c star). Axial T1 post-contrast MR imaging shows a larger region of hypointensity in the left lobe of the liver extending into the right lobe (d arrows). The follow-up CT 3 months later shows hepatic atrophy with scarring and the formation of corkscrew collaterals (e arrows)
Superior vena cava compression/obstruction
The hepatic hot spot sign occurs in the presence of superior vena cava (SVC) compression or obstruction. It is secondary to increased flow through collateral veins, usually the left portal vein via the paraumbilical and internal mammary veins [9]. This is referred to as ‘third inflow,’ which represent venous perfusion of the liver separate from the portal venous and arterial systems [10]. The hot spot sign presents as focal increased enhancement in segment IV of the liver in the arterial and early portal venous phases, specifically when contrast media is injected in an upper extremity vein [9] (Fig. 7). The classic location with involvement of segment IV of the liver should raise suspicion about possible SVC pathology and imaging of the chest may be required to further delineate the pathology. Interestingly, when contrast is injected via a lower extremity vein, relative hypoenhancement within segment IV of the liver will be observed [10]. In contrast, in cases of inferior vena cava (IVC) compression or obstruction, a reversed pattern of hepatic segment IV hyperenhancement/hypoenhancement is seen depending on upper versus lower extremity contrast injection [10].

A 72-year-old patient with axial contrast-enhanced CT images in the portal venous phase showing the appearance of the ‘Hot Spot’ sign due to SVC compression. There is geographical hyperenhancement in segment IV of the liver (a, b) (arrows). There is a large necrotic mass in the right upper lobe of the lung that is occluding the SVC (c star)
Hereditary hemorrhagic telangiectasia
Hepatic vascular abnormalities are the most commonly occurring abdominal abnormality seen in patients with Hereditary Hemorrhagic Telangiectasia (HHT) (also known as Osler–Weber–Rendu Syndrome) [11]. The vascular abnormalities primarily consist of dilated hepatic venules with a direct connection to arterioles, seen as a combination of large confluent vascular masses (≥ 1 cm) and telangiectasias (< 1 cm). Arteriovenous, arterioportal, and portovenous shunts will also be seen, with shunting potentially leading to portal hypertension and even cardiac failure [11]. Extensive shunting may also lead to biliary disease manifesting most severely as biliary necrosis [11]. On CT and MRI, the vascular abnormalities will be best visualized on arterial phase images, which will outline a prominent supplying hepatic arterial branch in the case of confluent vascular masses and telangiectasias. Hepatic perfusional changes, which are non-focal regions of heterogeneous enhancement, will best be seen in the arterial phase on both CT and MRI (Fig. 8a, b). HHT should be considered in the setting of markedly enlarged hepatic arteries, multiple large and small arterially enhancing lesions, and a relatively normal appearance of the liver parenchyma in the venous phase (Fig. 8c, d). In addition to the liver, vascular abnormalities can be seen in other organ systems including the lungs, central nervous system, gastrointestinal tract, skin, and mucous membranes.

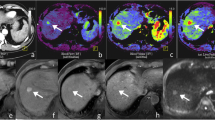
A 38-year-old patient with HHT. Axial and coronal contrast-enhanced CT images in the arterial phase show a 2.8 cm region of early arterial enhancement in the periphery of the liver (a, b) (stars) that has a large supplying artery (a arrow) and demonstrates early filling of portal venous branches (b arrows) due to arterioportal shunting secondary to a large confluent vascular mass. There is also a pulmonary AVM present in the left upper lobe with evidence of previous embolization (c arrow). The second case of HHT in a 49-year-old patient shows heterogeneously enhancing liver parenchyma with multiple hypervascular lesions in the arterial phase, in keeping with confluent vascular masses and telangiectasias (d arrows). 3D reconstruction of the aorta and its branches shows multiple vascular malformations along primarily branches of the replaced right hepatic artery seen arising from the SMA (e arrows)
Neoplastic etiologies
Benign
Hemangioma
Hemangioma is the most common benign tumor of the liver. It is not infrequently associated with hepatic perfusional changes [12, 13]. Again, these perfusional changes are best seen in the arterial and early portal venous phase as they become isoattenuating to the remainder of the liver parenchyma on the subsequent post-contrast phases in both CT and MRI (Fig. 9). The perilesional perfusional changes can be seen in the setting of typical as well as atypical hepatic hemangiomas, including sclerosed hemangiomas [10].

A 55-year-old patient with a hemangioma. Axial and coronal contrast-enhanced CT images show a wedge-shaped area of hyperenhancement in segment V of the liver in the arterial phase (a, b) (stars). A hypervascular flash-filling hemangioma is noted (b arrow). The geographic area of hyperenhancement becomes isoattenuating to liver parenchyma on the portal venous phase axial and coronal images (c, d). The hemangioma remains hyperattenuating as it follows the blood pool (arrows)
Malignant
Primary neoplasms
Hepatocellular carcinoma (HCC) is by far the most common primary malignant hepatic neoplasm. It is most often seen in the setting of cirrhosis as well as hepatitis B or C infection [14]. Single or multiple focal masses may be seen with perilesional perfusional changes. As well, approximately 5% of HCCs demonstrate an infiltrative rather than expansile growth pattern [14]. HCC is also often associated with portal vein thrombosis, by triggering the formation of bland thrombus or through direct tumor extension into the portal venous system (tumor thrombus). This will also lead to hepatic perfusional changes as discussed earlier. Other primary malignant hepatic neoplasms, such as cholangiocarcinoma and angiosarcoma, are not only less common, but they also rarely involve the intrahepatic vasculature [14].
Metastatic disease
Metastatic disease to the liver is more common than primary tumors. Metastatic lesions can be hypovascular from colorectal, lung, and breast primaries or can be hypervascular from melanoma, pancreatic neuroendocrine tumors, and renal cell carcinoma [15]. Perilesional hepatic perfusional changes, best seen in the arterial and early portal venous phase on CT and MRI, are primarily seen with hypervascular metastases (Fig. 10). In general, the presence of a region of hepatic parenchymal geographic or wedge-shaped enhancement in the arterial or early portal venous phase should trigger the search for an associated lesion that is resulting in this shunting phenomenon. This can be a benign lesion, primary hepatic malignancy, or metastasis (Table 1).

A 63-year-old patient with metastatic RCC to the liver. Enhancing tumor thrombus is seen within the right and left portal venous branches and portal confluence on the axial and coronal CT images in the arterial phase (a, b) (arrows). Heterogeneous geographic hypoenhancement is seen throughout the liver parenchyma secondary to this. A large heterogeneously enhancing infiltrative mass in the upper pole of the left kidney is noted in keeping with RCC (b star). A hypervascular metastatic deposit is noted in the right lobe of the liver (c arrow)
Infectious/inflammatory etiologies
Acute hepatitis
Acute hepatitis is secondary to an acute insult with secondary liver parenchymal inflammation. There are a number of etiologies associated with acute hepatitis, including viral infection, parasitic infection, autoimmune conditions, and drug-induced (chemotherapy, alcohol, and acetaminophen toxicity). Patients can be asymptomatic or can present with non-specific symptoms with elevation of liver enzymes (ALT and AST). The imaging appearance of the liver in the setting of acute hepatitis may be completely normal. Some non-specific findings include hepatosplenomegaly, ascites, and reactive gallbladder wall thickening. In addition, hepatic perfusional changes can be seen with regions of decreased liver parenchymal enhancement along with prominent periportal spaces demonstrating hypoattenuation on CT and T2 hyperintense signal on MRI due to periportal edema [16] (Fig. 11). Overall, similar imaging findings are seen on both CT and MR.

A 66-year-old patient with recent history of chemotherapy treatment. Axial post-contrast CT images in the portal venous phase shows a wedge-shaped region of patchy hypoenhancement in segment VIII of the liver (a, b) (arrows). There are no liver masses evident and the hepatic vasculature is patent. These findings were favored to represent chemotherapy-induced focal hepatic inflammation/hepatitis. A follow-up CT 6 months later shows complete resolution of the perfusion defect in hepatic segment VIII (c)
Cholangitis
The term cholangitis is a broad reference to inflammation of the biliary tree. Cholangitis can be acute in the setting of infection (ascending cholangitis) or can be subacute/chronic secondary to infectious (recurrent pyogenic cholangitis, Epstein-Barr Virus [EBV] cholangitis), inflammatory (inflammatory bowel disease [IBD]-associated sclerosing cholangitis, chemotherapy-induced cholangitis, eosinophilic cholangitis), and idiopathic (primary sclerosing cholangitis) etiologies [17]. The clinical history is essential for making the distinction between the different types. On CT, non-specific heterogeneous hepatic parenchymal enhancement may be seen in both the arterial and venous phases in the acute setting (Fig. 12). In some cases, distinct transient hyperenhancement can be seen on the arterial phase images [17]. Intra- and/or extra-hepatic biliary ductal wall thickening and hyperenhancement can also be seen [17]. MRI is a more sensitive modality as it will more clearly outline the abnormal ductal wall thickening and hyperenhancement, as well as demonstrate periductal inflammation in the form of patchy increased signal on T2-weighted images and DWI. Furthermore, Magnetic Resonance Cholangiopancreatography (MRCP) will best demonstrate the biliary anatomy and highlight dominant strictures, which are a sequela of long-standing chronic cholangitis. Intra-ductal stones and sludge can also be seen on MRI. Both CT and MR may demonstrate THEDs secondary to periductal inflammation, best seen in the arterial phase. In the chronic setting, a more homogeneous hepatic parenchymal enhancement pattern may be seen along with biliary atrophy and lobar distribution. Moreover, patients with chronic cholangitis, particularly sclerosing cholangitis, must be closely monitored as they are at risk of developing cholangiocarcinoma [17].

A 48-year-old patient with clinical signs of acute cholangitis. Large geographic regions of hypoattenuation surrounded by diffusely heterogeneous enhancement are seen on both an axial CT image in the arterial phase (a arrows) and an axial post-contrast MR image in the portal venous phase (b arrows). There was also mild biliary ductal wall thickening and hyperenhancement present (not shown). Axial T2-weighted MR shows patchy hyperintensity in the periphery of the liver (c arrows) that shows restricted diffusion on DWI (d arrows) consistent with a diagnosis of ascending cholangitis with reactive perfusional changes and inflammatory changes in the liver parenchyma
Fitz–Hugh–Curtis syndrome
Fitz–Hugh–Curtis syndrome (FHCS) is a form of perihepatitis and a complication of pelvic inflammatory disease (PID). The pathogens associated with PID can sometimes reach the liver capsule leading to capsular inflammation and occasional adhesions with the adjacent structures such as the diaphragm and parietal peritoneum [18]. The appearance of the liver in this condition closely mimics the appearance of a nutmeg liver on contrast-enhanced CT due to venous congestion as a result of hepatic capsular inflammation and perihepatitis [19] (Fig. 13a, b). The hepatic perfusional changes along with right upper quadrant pain and pelvic findings consistent with PID have to be considered in combination in order to suggest this diagnosis [19]. Otherwise, the appearance of the congested liver (nutmeg liver) is non-specific. MRI findings include hepatic capsular thickening and increased signal seen on the T2-weighted images and DWI, along with capsular thickening and hyperenhancement seen on the post-contrast images [18]. Moreover, other pelvic/gynecologic pathologies can mimic the hepatic changes/perihepatitis seen in the setting of FHCS, as in this case of a torted uterine fibroid (Fig. 13c, d).

A 35-year-old patient with PID (pelvic images not shown) with findings suggestive of associated Fitz–Hugh–Curtis syndrome. Axial and coronal contrast-enhanced CT images in the portal venous phase show abnormal heterogeneous hepatic parenchymal enhancement predominantly in the periphery of the liver (a, b) (arrows). This is due to reactive perfusional changes secondary to hepatic capsular inflammation. The second case is a 48-year-old patient with a torted uterine fibroid that resulted in a similar mottled appearance of the hepatic parenchyma due to hepatic capsular inflammation/perihepatitis with associated hepatic congestion/reactive perfusional changes seen in the portal venous phase (c arrows). The torted right adnexal leiomyoma shows peripheral enhancement and central necrosis (d star); surrounding inflammatory changes and fatty stranding also noted (arrow)
Inflammatory pseudotumors
Inflammatory pseudotumor of the liver, also known as inflammatory myofibroblastic tumor or plasma cell granuloma/xanthomatous pseudotumor, is a rare entity with a non-specific clinical presentation and imaging findings [20]. It is benign and can be associated with IgG4 disease [21]. On CT, single or multiple fibrotic/inflammatory mass-like lesions may be seen. These are generally centrally hypodense with variable peripheral enhancement of the adjacent liver parenchyma. These lesions will show homogeneous delayed enhancement [21]. On MRI, these pseudotumors are usually T1 hypointense and T2 hyperintense with heterogeneous enhancement on the post-contrast images (Fig. 14). The enhancement pattern is highly variable and can sometimes be completely absent or can be absent centrally due to necrosis. Given that this is a rare entity, biopsy is often required to confirm the diagnosis as the differential considerations include hepatocellular carcinoma and cholangiocarcinoma. An elevated serum IgG4 level or other manifestations of IgG4 disease elsewhere may also help narrow down the differential diagnosis. These pseudo-masses can regress spontaneously with or without conservative management. Some complications include portal thrombophlebitis, portal hypertension, and biliary obstruction [10].

A 44-year-old patient with inflammatory pseudotumors of the liver. Axial contrast-enhanced CT images show hepatomegaly with early enhancement of the hepatic arteries in the arterial phase (a arrows) with central heterogeneous hypoenhancement in the portal venous phase (b arrows). Axial post-contrast MR images shows focal targetoid lesions centrally (c arrows) with a large wedge-shaped perfusion abnormality in the arterial phase (star). On the portal venous phase image, there is poor enhancement of the hepatic veins and no opacification of the middle and left hepatic veins (d arrows)
Confluent hepatic fibrosis
Confluent hepatic fibrosis can result from chronic hepatic injury in the setting of cirrhosis or secondary to hepatic vascular injury [22]. These prominent fibrotic scars in the periphery of the liver can mimic mass lesions. On CT, regions of confluent fibrosis will be wedge-shaped and hypoattenuating on unenhanced imaging. Post-contrast, it can be distinguished from hepatocellular carcinoma as it will shows progressive geographic/wedge-shaped enhancement without washout [22]. As well, it will generally show straight or concave borders, as opposed to the convex borders that are commonly seen with true masses. On MRI, peripheral wedge-shaped regions of mild T2 hyperintensity can be seen. Post-contrast, progressive enhancement will be seen without washout, similar to CT (Fig. 15). The challenge with confluent hepatic fibrosis can be the overlapping imaging findings with cholangiocarcinoma, which also demonstrates progressive enhancement [22]. However, intrahepatic cholangiocarcinoma is often more mass-like, is associated with more biliary ductal dilatation, and demonstrates restricted diffusion on DWI MRI. In addition, both entities can have associated hepatic parenchymal volume loss with capsular retraction.

A 57-year-old patient with confluent hepatic fibrosis. Patchy geographic regions of hyperintensity are seen on the axial T2-weighted image (a arrows) with similar patchy geographic primarily peripheral high signal noted on the DWI image (b arrows). There are patchy geographic regions of hyperenhancement within the liver parenchyma on the post-contrast MR images in the arterial phase, most prominent within the wedge-shaped region within the right lobe (c star). This persists on the PV phase image (d star). Capsular retraction is also noted (arrow)
Imaging techniques
In characterizing hepatic perfusional changes and any additional associated liver abnormalities, both multiphasic contrast-enhanced CT and MRI can be effectively utilized. In the case of CT, at minimum late arterial (35–45 s post contrast injection) and venous phase (60–75 s post contrast injection) images are needed [23]. Depending on the clinical context, delayed phase images (2–5 min post contrast injection) may also be of added value [23]. MRI imaging should include the standard T1, T2, and DWI sequences, in addition to pre- and post-contrast imaging utilizing a Gadolinium-based contrast agent [23]. This can be performed with either a 1.5T or 3T magnet with a phased array multichannel torso coil. The post-contrast images should be performed in the arterial (late arterial phase should be used with either bolus tracking or a multi-arterial acquisition), venous (60–80 s post contrast injection), and delayed phases (2–5 min post contrast injection) [23]. As well, depending on the clinical context, hepatobiliary contrast agents can be utilized, which should include arterial and portal venous post-contrast imaging, in addition to delayed hepatobiliary phase images (up to 20 min post contrast injection) [23]. MRI offers the additional advantage of allowing for subtraction images generated from post-processing of the pre-contrast and post-contrast images. This allows for optimal assessment of true enhancement [23]. Liver ultrasound and contrast-enhanced ultrasound are additional cost-effective and beneficial techniques for liver imaging; however, they are less valuable in the detection and characterization of hepatic perfusional changes.
Conclusion
This review aimed to present an overview of a number of relevant pathologies that exhibit the sometimes over-looked hepatic perfusional changes. There are a multitude of causes for hepatic perfusional changes. Most of these are related to vascular pathologies affecting branches of the hepatic arteries, portal veins, or hepatic veins or are inflammatory in nature. Perfusional abnormalities can also occur adjacent to benign and malignant neoplasms and in tumor-like conditions. This review serves to highlight some important causes, as well as some strategies for differentiating the various conditions on imaging. It is imperative that the radiologist understand the various presentations of hepatic perfusional changes and perfusion defects and be aware of factors that help narrow down the differential diagnosis. In addition to recognizing the imaging features of the different pathologies, it is crucial to also be aware of the relevant clinical and biochemical findings that can help clinch the diagnosis.
References
Lupescu IG, Grasu M, Capşa R, Pitrop A, Georgescu SA. Hepatic perfusion disorders: Computer-tomographic and magnetic resonance imaging. J Gastrointest Liver Dis 2006;15:273–9.
Torabi M, Hosseinzadeh K, Federle MP. CT of nonneoplastic epatic vascular and perfusion disorders. Radiographics 2008;28:1967–82. https://doi.org/10.1148/rg.287085067.
Li YL, Lee KH, Cheng AKC, Yu ML. Nutmeg liver. Abdom Radiol 2018;43:1275–6. https://doi.org/10.1007/s00261-017-1283-4.
Wells ML, Fenstad ER, Poterucha JT, Hough DM, Young PM, Araoz PA, et al. Imaging findings of congestive hepatopathy. Radiographics 2016;36:1024–37. https://doi.org/10.1148/rg.2016150207.
Das CJ, Soneja M, Tayal S, Chahal A, Srivastava S, Kumar A, et al. Role of radiological imaging and interventions in management of Budd–Chiari syndrome. Clin Radiol 2018;73:610–24. https://doi.org/10.1016/j.crad.2018.02.003.
Yang S, Wu J, Lei S. CT Features of Hepatic Veno-occlusive Disease: A Meta-analysis. Acad Radiol 2018;25:328–37. https://doi.org/10.1016/j.acra.2017.10.012.
Qi X, Han G, He C, Yin Z, Guo W, Niu J, et al. CT features of non-malignant portal vein thrombosis: A pictorial review. Clin Res Hepatol Gastroenterol 2012;36:561–8. https://doi.org/10.1016/j.clinre.2012.05.021.
Adler DD, Glazer GM, Silver TM. Computed tomography of liver infarction. Am J Roentgenol 1984;142:315–8. https://doi.org/10.2214/ajr.142.2.315.
Dickson AM. The focal hepatic hot spot sign. Radiology 2005;237:647–8. https://doi.org/10.1148/radiol.2372031690.
Costa AF, Clarke SE, Stueck AE, McInnes MDF, Thipphavong S. Benign Neoplasms, Mass-Like Infections, and Pseudotumors That Mimic Hepatic Malignancy at MRI. J Magn Reson Imaging 2020. https://doi.org/10.1002/jmri.27251.
Welle CL, Welch BT, Brinjikji W, Ehman EC, Venkatesh SK, Johnson MP, et al. Abdominal manifestations of hereditary hemorrhagic telangiectasia: a series of 333 patients over 15 years. Abdom Radiol 2019. https://doi.org/10.1007/s00261-019-01976-7.
Byun JH, Kim TK, Lee CW, Lee JK, Kim AY, Kim PN, et al. Arterioportal shunt: Prevalence in small hemangiomas versus that in hepatocellular carcinomas 3 cm or smaller at two-phase helical CT. Radiology 2004;232:354–60. https://doi.org/10.1148/radiol.2322030966.
Mathew RP, Sam M, Raubenheimer M, Patel V, Low G. Hepatic hemangiomas: the various imaging avatars and its mimickers. Radiol Medica 2020. https://doi.org/10.1007/s11547-020-01185-z.
Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 2014;272:635–54. https://doi.org/10.1148/radiol.14132361.
Sica GT, Ji H, Ros PR. CT and MR Imaging of Hepatic Metastases. Am J Roentgenol 2000;174:691–8. https://doi.org/10.2214/ajr.174.3.1740691.
Sharma A, Houshyar R, Bhosale P, Choi J Il, Gulati R, Lall C. Chemotherapy induced liver abnormalities: an imaging perspective. Clin Mol Hepatol 2014;20:317–26. https://doi.org/10.3350/cmh.2014.20.3.317.
Kim SW, Shin HC, Kim IY. Transient arterial enhancement of the hepatic parenchyma in patients with acute cholangitis. J Comput Assist Tomogr 2009;33:398–404. https://doi.org/10.1097/rct.0b013e318186faa1.
Matsumoto K, Inoue F, Amano S, Tamura Y, Ashiarai M. Fitz-Hugh-Curtis Syndrome Preceded by Constipation in a 14-Year-Old Girl. Gynecol Obs Case Rep 2018;4:57. https://doi.org/10.21767/2471-8165.1000057.
de Boer JP, Verpalen IM, Gabriëls RY, de Haan H, Meijssen M, Bloembergen P, et al. Fitz-Hugh-Curtis syndrome resulting in nutmeg liver on computed tomography. Radiol Case Reports 2019;14:930–3. https://doi.org/10.1016/j.radcr.2019.04.008.
Zhang Y, Lu H, Ji H, Li Y. Inflammatory pseudotumor of the liver: A case report and literature review. Intractable Rare Dis Res 2015;4:155–8. https://doi.org/10.5582/irdr.2015.01021.
Kurowecki D, Patlas MN, Haider EA, Alabousi A. Cross-sectional pictorial review of IgG4-related disease. Br J Radiol 2019;92. https://doi.org/10.1259/bjr.20190448.
Faria SC, Ganesan K, Mwangi I, Shiehmorteza M, Viamonte B, Mazhar S, et al. MR imaging of liver fibrosis: Current state of the art. Radiographics 2009;29:1615–35. https://doi.org/10.1148/rg.296095512.
Chandarana H, Fowler UC San Diego Alice Fung KJ, Ganeshan Sir Reliance Foundation Rajan Gupta KH, Harris Vancouver Imaging Thomas Hope San Francisco Jeanne Horowitz AU, Hussain H, Sahani Massachusetts General Hospital Claude Sirlin UC San Diego Vahid Yaghmai DB. LI-RADS ® v2018 CT/MRI Core LI-RADS ® Technique. n.d.
Funding
This paper received no funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
CME activity This article has been selected as the CME activity for the current month. Please visit https://ce.mayo.edu/node/103495 and follow the instructions to complete this CME activity.
Rights and permissions
About this article

Cite this article
Gunter, D., Riaz, S., Haider, E.A. et al. Hepatic perfusional changes on CT and MRI: a radiology primer. Abdom Radiol 46, 179–196 (2021). https://doi.org/10.1007/s00261-020-02787-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-020-02787-x