
Abstract
Background
To study the frequency and outcomes of percutaneous imaging-guided drainage following pancreaticoduodenectomy and to assess if fluid collection location correlates with pancreatic duct leak.
Methods
IRB approval was obtained. Three hundred and seventy-three subjects (age 21–84 years) who underwent pancreaticoduodenectomy were included in this retrospective study. Eighty-three of these subjects underwent post-operative imaging-guided drainage (CT 77; US 6). Medical and imaging records were reviewed. Procedural details including collection location, size, catheter size, drain duration, fluid type, fluid chemistry, and fluid culture were recorded. Collection location was correlated with fluid amylase.
Results
The frequency of imaging-guided percutaneous drainage following Whipple was 22.2%. The immediate technical and overall success rates for fluid collection drainage were 97.6% and 79.6%, respectively. Rate of complication was 4.8% (4/83). 74.7% (62/83) of fluid collections were proven abscesses, and 61.4% (51/83) were complicated by pancreatic fistula. Collections near the pancreatic resection site were more likely to have elevated fluid amylase.
Conclusion
Approximately one-fifth of subjects requires percutaneous drainage following pancreaticoduodenectomy. Percutaneous imaging-guided drainage is an effective means of managing post-pancreaticoduodenectomy fluid collections. Collections near the pancreas resection site often have a pancreatic duct leak.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Pancreaticoduodenectomy (Whipple procedure) is the standard operation for carcinoma of the head of the pancreas. This operation classically involves en bloc resection of the pancreatic head; the first, second, and third portions of the duodenum; the distal common bile duct and often the distal gastric antrum. A gastrojejunostomy is performed to reconstruct the gastrointestinal tract and the common bile duct and residual pancreas are anastomosed into a segment of small bowel.
Historically, pancreaticoduodenectomy has been associated with significant mortality and morbidity. However, in high-volume referral centers, the mortality rate for this operation has consistently been <5%, with a morbidity rate of ∼30% [1].
The interventional radiologist can provide minimally invasive image-guided percutaneous drainage of abdominal abscesses, bilomas, liver abscesses, biliary obstructions, pseudocysts, and hemorrhages that may arise post-operatively. Image guidance is typically provided with CT or ultrasound. Prompt recognition and treatment of post-operative fluid collections amenable to percutaneous image-guided drainage may minimize re-operation, shorten recovery time, and decrease perioperative morbidity [2].
The primary purpose of our research was to study the frequency and outcomes of percutaneous image-guided drainage following Whipple. A secondary purpose was to study the effect of pancreatic duct leak on success of the drainage procedure and to assess whether collection location correlated with evidence of pancreatic duct leak.
Materials and methods
The study was approved by our Institutional Review Board prior to enrollment of any subjects. Due to the retrospective design, written informed consent was waived.
This was a retrospective study of all subjects who underwent Whipple procedure from February 1995 through March 2007. We identified subjects who underwent post-operative image-guided drainage. For each subject, both the medical and imaging electronic records were reviewed. Reviewed data included demographic data and procedure details including: fluid collection location, collection size, drain catheter size, aspirated fluid volume, fluid type, fluid culture and chemistries, and drain duration. Limited by the constraints of retrospective review, complete descriptive fluid culture and character results were available in 59/83 and 76/83 subjects, respectively. All subjects had both pre- and post-drainage CT imaging available. All Whipple subjects had Jackson Pratt-type drains placed at the time of surgery. Pre-, post-, and follow-up CT exams were reviewed in all subjects. Chart review of drain and surgical outcomes was performed including review of documented complications.
In order to better characterize drainage outcomes, several terms were defined. Immediate technical success was defined as successful aspiration or drain placement at the time of procedure. Single drainage success was defined as resolution of the collection on follow-up imaging and clinical improvement after a single procedure. Likewise, multiple drainage success was defined as clinical improvement without an operation following multiple drainages. We separately evaluated cases complicated by abscess or elevated fluid amylase.
A total of 373 Whipple subjects were identified with 146 (39.1%) females and 227 (60.9%) males with an age range of 21–84 years and mean age of 60.7 years. The most common pathology was pancreatic adenocarcinoma with 185 cases. There were 48 cases of ampullary carcinoma, 36 cases of chronic pancreatitis, and 25 cases of cholangiocarcinoma. Seventy-nine remaining cases with other pathology included: functioning and non-functioning neuroendocrine tumors, duodenal adenocarcinoma, benign biliary stricture, choledochol cyst, mucinous cystic neoplasm, serous microcystic adeoma, variant ampullary adenocarcinoma vs. cholangiocarcinoma, intraductal papillary mucinous tumor, combined ductal and ampullary carinoma, duodenal adenoma with and without villous components, gastrointestinal stromal tumor, lymphoma, and metastatic disease (renal cell carcinoma, colon carcinoma, and malignant fibrous hystiocytoma), fibrous disease with and without the presence granuloma, solid and pseudopapillary tumor, and villous adenoma of the ampulla of Vater.
Results
Of the 373 Whipple subjects, we observed that 83 (22.2%) required post-surgical drainage. Drainages occurred on average 14.8 days post-Whipple with a range of 1 to 71 days. Of the 83, 77 (92.8%) subjects were drained under CT guidance; 6 (7.2%) subjects were drained under ultrasound guidance. Nearly all of these drainages had immediate procedural success with 81/83 (97.6%) success recorded.
Overall outcomes of our 83 subjects included 34 successful single drainage cases and 32 successful multi-drainage cases for an overall drainage success rate of 66/83 (79.6%) (Fig. 1). Of the 43, 32 (74.4%) multiple drainage cases were successful with the average number of drainage procedures equal to 3.4 (range 2–11).

Overall outcomes of 83 patient drainage group. 39.6% single drainage and 41.0% multi-drainage success were observed combining for an overall drainage success in our 83 patients' of 79.6%.
Of the 83, 26 (31.3%) collections were located in the region of the pancreatic surgical bed. Mean diameter of largest collection was 7.4 cm (range 1.4–19.5 cm). At the time of initial drainage 67% of cases had between 5 and 100 mL aspirated (absolute range 0–1200 mL).
All cases with drainage catheter placement were performed utilizing Seldinger technique or aspiration via an 18-gauge trocar needle. 80.5% of catheters utilized ranged from 10–14 French. The character of fluid reported was variably reported as “purulent” in 24/76 (31.6%) cases, “bloody” or “serosanguinous” 19/76 (25.0%) cases, and “clear yellow” 6/76 (7.9%) cases. More valuable were the results of fluid culture with 42/59 (71.2%) collections polymicrobial. Of the 59, 19 (32.2%) cases contained either methicillin resistant Staphylococcus aureus or Candida albicans. Of the 83, 62 (74.7%) fluid collections were proven abscesses (Fig. 2).

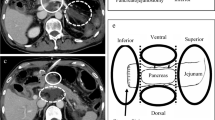
A 65-year-old male with post-surgical fluid collection. (A) Collection is seen in the pancreatic surgical bed adjacent to several surgical clips (arrow). (B) Needle aspiration (arrow) revealed turbid fluid with an elevated amylase; cultures were positive for bacteria. (C) The collection was successfully drained with a single drainage catheter (arrow).
Of the 83, 4 (4.8%) immediate post-procedural complications were reported with single cases of catheters trangressing colon, small bowel, and pleura, respectively. A fourth subject developed fever and chills during the procedure representing transient sepsis.
Of the 83, 51 (61.4%) collections had elevated fluid amylase values over 150 units/L. All elevated amylase values were more than three times greater than serum amylase and thus met criteria for suspected pancreatic duct leak. Of the 33, 27 (81.8%) collections with elevated amylase were located within or adjacent to the pancreatic resection site, while 10/22 (45.5%) collections with elevated amylase were located about the liver. There were three biliary fistulas as determined by imaging and/or drain output and five entero-cutaneous fistulas as proven by imaging or surgery.
In the subset of subjects in whom there was an abscess, there were 25 single drain success cases, and 28 multi-drain success cases for a 53/62 (85.5%) overall drainage success rate. In the subset of subjects in whom fluid had elevated amylase, there were 23 single drain success cases and 22 multi-drain success cases for a 45/51 (88.2%) overall drainage success rate (Fig. 3).

Subgroup analysis showed similar success in cases complicated by abscess or elevated fluid amylase. These subgroups had overall drainage success of 85.5% and 88.2%, respectively.
Drain durations were recorded for each of the groups (Fig. 4). In the 83 subjects, there was a median drain duration of 28.0 days with a range of 3 to 152 days. In the abscess group, there was a median drain duration of 29.0 days with a range of 4 to 152 days. In contrast, in subjects without abscess, median drain duration was 11.0 days with a range of 3 to 60 days. In the pancreatic leak group, there was a median drain duration of 29.8 days with a range of 4 to 152 days. In the subjects without elevated amylase in the fluid, there was a median drain duration of 24.5 days with a range of 3 to 117 days.

Median drain duration in subgroups. Although cases with abscess and elevated fluid amylase had similar drainage success when compared to the overall group of 83 subjects, both the abscess and pancreatic leak groups required longer drainage duration over the cases without abscess and with normal fluid amylase values.
Discussion
Pancreaticoduodenectomy is a procedure associated with a relatively high morbidity and mortality even at high volume centers [1]. While refinements in surgical technique and perioperative management have led to a marked reduction in operative mortality, mobidity remains on the order of 30% [1]. Our own institutional experience with patients undergoing surgery alone and in those undergoing neoadjuvant chemoradiation prior to surgery has identified that peripancreatic fluid collections remain a frequent source of post-operative morbidity [3]. The observation that 22.2% of patients undergoing a pancreaticoduodenectomy over a 12-year period required percutaneous interventions highlights the importance of an aggressive interventional abdominal imaging team in the post-operative management of these patients.
Post-operative fluid collections at our institution were rarely drained prior to postoperative day 5. In general, most postoperative Whipple fluid collections can be approached percutaneously as long as the subject is hemodynamically stable, has an acceptable coagulation panel, and there is a safe access route for a needle. In special cases, an unconventional approach (e.g., transpleural) might be taken to access difficult to reach collections. Moreover, although an abscess is often associated with fever, leukocytosis, pain, or sepsis, small but significant numbers of clinically silent abscesses have been reported [4].
Three-quarters of our drainage subjects proved to have abscess, reflecting the known high level of morbidity seen in complicated post-Whipple cases. Nearly one-third of subjects grew resistant organisms, either methicillin-resistant Staphylococcus aureus or Candida albicans. These results point to the validity of attempting to obtain fluid for culture and sensitivities in cases where there are no overt sign or symptoms of infection. In the case of a small collection, one might simply perform an aspiration for culture and sensitivity rather than place a drainage catheter.
The rates at which image-guided intervention is performed are likely highly institutional dependent, and maybe influenced by factors such as availability of service, interdisciplinary follow-up, procedural experience, and logistics of an abdominal intervention service. Beecher et al. [5] recommended that once post-pancreaticoduodenectomy fluid collection is identified input from interventional radiology, gastroenterology, and surgery should be available to choose optimal treatment that might include a single intervention or an orchestrated approach of all specialties. Studies report rates of image-guided intervention post-Whipple between 8% and13% [6, 7].
Our results show that percutaneous drainage is safe and successful following pancreaticoduodenectomy and raise the question as to whether surgical drains should be placed at all. Conlon et al. [8] prospectively randomized patients undergoing Whipple to either have no drains placed or to have standard surgical drains placed. This clinical trial failed to show a reduction in the number of deaths, need for interventional radiologic drainage, or surgical exploration with the addition of surgical drain placement; the study concluded that surgical drainage should not be considered mandatory or standard after pancreatic resection [8].
There are two studies that specifically describe experience with percutaneous drainage following pancreaticoduodenectomy. AAssar et al. [9] performed a retrospective review of 19 subjects with fluid collections status post-pancreaticoduodenectomy who underwent image-guided drainage with success rate of 17 of 19 subjects (89%). In 2003, Sohn et al. [7] retrospectively reviewed 1061 subjects who underwent pancreaticoduodenectomy. One hundred and twenty-nine (12%) required postoperative interventional radiologic procedures. Eighty-four subjects underwent percutaneous aspiration or catheter drainage for intra-abdominal abscess, biloma, or lymphocele, with two or more abscess drains required in 24 subjects. Of the 129, 19 subjects (15%) who required postoperative radiologic intervention also required reoperation.
AAssar et al. [9] reported 88% rate of percutaneous drainage success even though three subjects had concurrent biliary fistulas and all subjects demonstrated a fistulous connection at the pancreatico-jejunal anastomosis. Likewise, our results demonstrate a similar high rate of success (88%) even in patients with pancreatic leak. Gervais et al. [2] reported that advances in cross-sectional imaging and improvements in image-guided intervention have contributed to the decreasing perioperative mortality rate following Whipple procedure.
Singh et al. [10] reported success rates of catheter drainage for abdominal collections with biliary and pancreatic ductal communications of 93% (39/42) and 67% (10/15), respectively. However, this study was not confined to the post-pancreaticoduodenectomy subject, but included a retrospective review of subjects with abdominal collections with proven pancreaticobiliary fistulous communication of variable etiologies.
Although many of our subjects improved with image-guided drainage, both abscesses and collections with pancreatic leak required longer median drainage durations, 29.0 and 29.8 days, respectively. Moreover, in no group was the average drain duration trivial. Across all 83 subjects median drain duration was 28 days and even in the no abscess group, the median duration was 11 days. In light of these findings, when providing informed consent, the physician should state that although the drainage catheters have a high success rate, several weeks of drainage may be required. These drain durations are compatible with those reported by AAssar et al. [9], where the average drain duration was 31 days.
A secondary purpose of our research was to study the effect of pancreatic duct leak on success of the drainage procedure and to determine if collection location correlated with evidence of pancreatic duct leak. We observed that fluid collections about the pancreas had abnormally elevated amylase values compatible with leak in 81.8% (27/33) of cases, in contrast to collections situated about the liver which had elevated fluid amylase values in only 45.5% (10/22) of the collections. Our findings are supported by previous work by Hashimoto et al. [11] who observed that fluid collections around the pancreaticojejunostomy site were significantly associated with a pancreatic fistula.
The major limitation of this study was that it was performed retrospectively such that research questions were limited by the confines of preexisting data. Future work might include prospective comparison of drainage verses observation in post-surgical collections without clear clinical signs of sepsis.
In conclusion, approximately one-fifth of post-Whipple subjects require post-surgical image-guided drainage. Although subjects with abscess and/or pancreatic leak did require longer courses of drainage, 80%–88% of these subjects were successfully drained. Those collections about the pancreatic resection site were likely to be associated with a pancreatic duct leak. Aggressive use of interventional percutaneous drainage in the perioperative period of patients undergoing pancreaticoduodenectomy is a safe and effective way to manage fluid collections that arise as a result of this surgical procedure.
References
Erickson, RA (2005) Pancreatic cancer. Emedicine.com. http://www.emedicine.com/med/topic1712.htm. Accessed December 15, 2005
Gervais DA, Fernandez-del Castillo C, O’Neill MJ, et al. (2001) Complications after pancreatoduodenectomy: imaging and imaging-guided interventional procedures. Radiographics 21:673–690
Cheng T, Sheth K, White RR, et al. (2006) Effect of neoadjuvant chemoradiation on operative mortality and morbidity for pancreaticoduodenectomy. Ann Surg Oncol 13(1):66–74
Goldman R, Hunter TB, Haber K (2006) The silent abdominal abscess: role of the radiologist. AJR 187:1591–1596
Beecher EE, Shires GT, Shires GT (2004) Treatment of post-pancreaticoduodenectomy complications. Curr Treat Options Gastroenterol 7(5):365–370
Suzuki Y, Fujino Y, Ajiki T, et al. (2005) No mortality among 100 consecutive pancreaticoduodenectomies in a middle-volume center. World J Surg 29(11):1409–1414
Sohn TA, Yeo CJ, Cameron JL, et al. (2003) Pancreaticoduodenectomy: role of interventional radiologists in managing patients and complications. J Gastrointest Surg 7(2):209–219
Conlon KC, Labow D, Leung D, et al. (2001) Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Ann Surg 234(4):487–493
AAssar OS, LaBerge JM, Gordon RL, et al. (1999) Percutaneous management of abscess and fistula following pancreaticoduodenectomy. Cardiovasc Intervent Radiol 22(1):25–28
Singh AK, Gervais DA, Alhilali LM, et al. (2006) Imaging-guided catheter drainage of abdominal collections with fistulous pancreaticobiliary communication. AJR 187:1591–1596
Hashimoto M, Koga M, Ishiyama K, et al. (2007) CT features of pancreatic fistula after pancreaticoduodenectomy. AJR 188:W323–W327
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zink, S.I., Soloff, E.V., White, R.R. et al. Pancreaticoduodenectomy: frequency and outcome of post-operative imaging-guided percutaneous drainage. Abdom Imaging 34, 767–771 (2009). https://doi.org/10.1007/s00261-008-9455-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-008-9455-x