
Abstract
Objective
To compare the diagnostic accuracy of 3-T magnetic resonance imaging (MRI) with thin-slice 3D T1 VIBE sequence to 128-slice computer tomography (CT) in pars stress fractures of the lumbar spine.
Materials and methods
3-T MRI and CT of 24 patients involving 70 pars interarticularis were retrospectively reviewed by four blinded radiologists. The fracture morphology (complete, incomplete, or normal) was assessed on MRI and CT at different time points. Pars interarticularis bone marrow edema (present or absent) was also evaluated on MRI.
Results
In total, 14 complete fractures, 31 incomplete fractures and 25 normal pars were detected by CT. Bone marrow edema was seen in seven of the complete and 25 of the incomplete fractures. The overall sensitivity, specificity and accuracy of MRI in detecting fractures (complete and incomplete) were 97.7, 92.3, and 95.7 %, respectively. MRI was 100 % accurate in detecting complete fractures. For incomplete fractures, the sensitivity, specificity, and accuracy of MRI were 96.7, 92.0, and 94.6 %, respectively.
Conclusions
3-T MRI with thin-slice 3D T1 VIBE is 100 % accurate in diagnosing complete pars fractures and has excellent diagnostic ability in the detection and characterization of incomplete pars stress fractures compared to CT. MRI has the added advantages of detecting bone marrow edema and does not employ ionizing radiation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Spondylolysis is a bony defect or fracture in the pars interarticularis, which lies at the junction of the pedicle, lamina, superior, and inferior articular facets. Spondylolysis is thought to represent either a developmental lesion or a pars stress fracture, with a higher incidence of pars stress fractures in physically active adolescents [1, 2]. Within our Australian population, cricket, Australian Rules football, basketball, and tennis are associated with increased incidence of pars stress fractures. Globally, gymnasts, football linemen, weightlifters, wrestlers, dances, javelin throwers, high jumpers, and divers are the most commonly affected individuals [3, 4].
Early detection of spondylolysis is crucial to maximize the chance of bony repair with conservative management and avoid chronic nonunion and spondylolisthesis. Conventional radiography is not reliable for detection of early active or incomplete fractures [5–7]. CT has been the reference standard for assessing the extent of fractures and bony healing but is less sensitive than bone scintigraphy and MRI for distinguishing active healing fractures from inactive chronic non-union [8]. CT and bone scintigraphy also expose this predominantly young patient population to ionizing radiation and is thus not the ideal imaging modality.
MRI, in contrast, combines morphologic pars information with the presence or absence of bone marrow edema. This enables differentiation between acute stress reactions, active spondylolysis and inactive chronic non-union. MRI grading that correlates with the stages of pathophysiological progression of pars stress fractures was established by Hollenberg et al. [9]; who developed a grading system for these fractures according to severity. A stress reaction was graded 1 and a chronic non-united complete fracture was graded 4. MRI has the advantage of not using ionizing radiation and the disadvantage that osseous anatomy is not as well demonstrated as CT [8–12].
Several studies have suggested that MRI should be the first-choice investigation for pars stress fractures [8, 10]. Following the initial MRI, targeted single level CT is then used to better assess fracture morphology and bony healing [8]. More recently, thin slice 3D volumetric interpolated breath-hold examination (VIBE) MRI; a modified fast 3D T1-weighted gradient-echo sequence, has been used to provide near-isotropic resolution in three dimensions with a short acquisition time. The VIBE sequence results in T1-weighted images with increased spatial resolution, improved image contrast, increased signal-to-noise ratio, and a shorter acquisition time than conventional MRI sequences, while preserving adequate anatomic coverage [13, 14].
Review of the current literature reveals no study that has compared the ability of 3-T MRI with thin-slice 3D T-1 VIBE sequence against CT in the detection and grading of pars stress fractures. The aim of this study was to assess the ability of 3-T MRI with thin-slice 3D T-1 VIBE sequence to accurately diagnose pars interarticularis stress fractures using CT as the reference.
Materials and methods
A retrospective search of the Picture Archiving and Communication System (PACS) at our institution, a large private musculoskeletal radiology practice, was performed for the period of September 2011 and December 2013. Informed consent was obtained from all individual participants included in the study, whereby they had consented to their images being used for research purposes at the time of imaging.
No additional consent was required for this retrospective audit. The retrospective audit did not alter a patient’s clinical management. MRI is the primary investigation in young patients presenting with back pain at our institution where stress fractures are a consideration. Each patient followed the conventional protocol at our institution for management and investigation of pars stress fracture. All procedures and imaging performed in this study were in accordance with the ethical standards of our institution. All consecutive patients less than 30 years of age who had undergone both CT and MRI (with the thin-slice 3D T-1 VIBE sequence) of their lumbar spine for diagnosis or assessment of a lumbar pars interarticularis stress reaction or fracture were included in the study. The patients must have had both CT and MRI of their lumbar spine within a 14-day period. In most patients, the MRI and then CT were performed on the same day. There were no technical issues with any of the studies that would have caused its exclusion.
The study coordinator reviewed each of the 24 patients’ radiology and selected specific vertebral levels for pars assessment by the blinded radiologists. Most patients had one lumbar vertebral level for analysis, but some had multiple levels assessed, resulting in 35 levels and 70 pars interarticulares for review. One patient had fractures at the T12 level.
MRI protocol
All MRI studies were performed on a 3-T Siemens (Magnetom Verio I-class. Erlangen, Germany) using a dedicated spine coil. The MRI pulse sequences performed were: sagittal, fast spin-echo, T1-weighted images [repetition time (TR)/echo time (TE) of 815 ms/12 ms, 30 cm field of view (FOV), and 3.5 mm section thickness]; sagittal, fast spin-echo, T2-weighted images (TR/TE of 3030 ms/75 ms, 30 cm FOV, and 4.5 mm section thickness); sagittal short-tau inversion recovery [STIR] [TR/TE/inversion time (TI) of 5490 ms/53 ms/130 ms, 30 cm FOV, and 3.5 mm section thickness]; axial, fast spin-echo, fat-saturated T2-weighted images (TR/TE of 3000 ms/61 ms, 20 cm FOV, and 3.5 mm section thickness); axial, fast spin-echo, T2-weighted images (TR/TE of 4900 ms/87 ms, 24 cm FOV, and 4.0 mm section thickness); and a sagittal, fat-saturated, three-dimensional (3D) gradient-echo, T1, VIBE sequence (TR/TE of 7 ms/2.45 ms, 20 cm FOV, 2 mm section thickness). Whilst all standard sequences for lumbar spine imaging were performed, only the sagittal 3D T1 VIBE and STIR sequences were used for the purposes of this study. The sagittal sequences were orientated in the best plane to assess the lumbar spine as decided by the MRI technologists at the time of scanning.
CT protocol
The CT studies of the lumbar spine were performed following the MRI in all cases. Targeted CT was performed only through the pathologic vertebral level as demonstrated on MRI, following the request of the managing medical practitioner. All CT examinations were performed using a 128-slice CT system (GE Optima 660, Milwaukee, WI, USA). The imaging parameters were: 140 kVp tube voltage, dose modulation 100–150 mA tube current, 1 s rotation time, 0.625 mm slice thickness, 0.312 mm reconstruction interval. Two-dimensional axial and sagittal reformatted images were created for each vertebral level as follows: 1 mm slice thickness, 1.5–2.0 mm space between images, 12 cm field of view, bone algorithm SS40, window width 2000, window level 450.
Data analysis
All MRI and CT images were anonymized and then randomly presented by a study coordinator for independent review by four experienced musculoskeletal radiologists (A.H.R., F.A.M., J.K.R., and T.O.S.), who combined had an average of 10 years of experience. Each radiologist assessed 70 pars interarticulares on both CT and MRI. The radiologists were blinded to the levels and the patient’s symptoms.
The CT and MRI were evaluated in a random order on separate sessions at least 1 week apart. On CT, the radiologists reviewed the axial and sagittal reformatted images. The radiologists graded each pars as either normal, having an incomplete or complete fracture. An incomplete pars fracture was defined as interruption of the pars’ inferomedial cortex with an intact superior cortex (Fig. 1a). A complete pars fracture was defined as contiguous interruption of the inferomedial cortex, trabecular bone, and superior cortex (Fig. 2a).

Sagittal CT (a) and sagittal 3-T MRI T-1 VIBE sequence (b) equally demonstrate an incomplete pars fracture at L5 in the same patient, where the fracture line involves the inferior cortex (arrow) and the superior cortex is intact

Sagittal CT (a) and sagittal 3-T MRI T-1 VIBE sequence (b) equally demonstrated a complete pars fracture at L2 in the same patient where there is contiguous interruption of the inferomedial cortex, trabecular bone and superior cortex (arrow). The sagittal 3-T MRI T-1 VIBE sequence inverted to simulate a CT style appearance (c)
On MRI, the radiologists assessed for the presence of fracture in the same manner as CT and also assessed for the presence of bone marrow edema. Only the sagittal 3D T-1 VIBE and STIR sequences were reviewed. The radiologists graded each pars’ morphology as normal, having an incomplete or complete fracture. The same definitions of incomplete and complete fractures for CT were used for the MRI grading (Figs. 1b and 2b). The VIBE sequence could be inverted to simulate a CT style appearance (Fig. 2c). Bone marrow edema was defined as increased signal intensity in the pars interarticularis, adjacent pedicle, superior and/or inferior articular process on STIR images (Fig. 3). The normal pars interarticularis above or below the abnormal level was used as an internal control. The radiologists made a binary decision as to the presence or absence of bone marrow edema on the STIR sequence only.

Sagittal 3-T MRI STIR demonstrates bone marrow edema where there is increased signal intensity in the L5 pars interarticularis (arrow)
An MRI grading system was applied to all fractures. In this study, a normal pars interarticularis was graded as 0, a stress reaction with no fracture was graded 1, an incomplete fracture with bone marrow edema was graded 2a, an incomplete fracture without bone marrow edema was graded 2b, a complete fracture with bone marrow edema was graded 3, and a complete fracture without bone marrow edema was graded 4 (Table 1).
As CT is unable to demonstrate bone marrow edema, grades 0 and 1, grades 2a and 2b and grades 3 and 4 were combined (Table 2).
After blinded assessment, the MRI and CT interpretations of each radiologist for each pars interarticularis were then evaluated by consensus and statistically reviewed. Any discrepancies between the MRI or CT interpretations between radiologists were reviewed by all radiologists, and in each case, a consensus was obtained.
Statistical analysis
Intraclass correlation coefficient (ICC) was used to measure the inter-reviewer reliability for assessment of bone marrow edema on MRI, for assessing for the presence of fractures on MRI and the presence of fractures on CT. Using CT as the standard of reference, the sensitivity, specificity and accuracy of MRI in detecting and characterizing pars fractures was then calculated.
Results
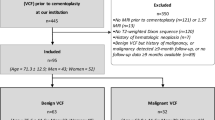
The database search revealed 24 patients who fulfilled the study inclusion and exclusion criteria. Of these 24 patients, a total of 35 vertebral levels were available for analysis. The right and left pars interarticularis at each of the 35 vertebral levels were assessed yielding 70 pars for analysis. Four of the 24 patients had recurrent disease.
Out of 70 pars interarticulares assessed, a total of 45 fractures were detected (14 complete and 31 incomplete) (Table 3). All fractures were orientated coronally. Twenty-five pars had no fracture. Thirteen of the 35 vertebral levels (37 %) had bilateral pars interarticulares fracture on CT and five of the 35 vertebral levels had bilateral complete pars fractures (14 %). The mean age of the patients was 19.7 years (range, 14–26 years; 22 males and two females). Four patients had pars stress fractures at two levels, and one patient had pars stress injuries at three levels. L5 was the most common vertebral level involved, followed by L4, L3 and L2 in decreasing order. None of our patients had pars interarticularis stress injuries at L1, and there were two incomplete fractures at T12 (Table 4).
There were 24 patients in total, of which, ten were professional athletes. Twenty patients had both MRI and CT on one occasion, three patients had both MRI and CT on two occasions and one patient had both MRI and CT on three occasions.
Intraclass correlation coefficient (ICC) demonstrated very strong agreement between the radiologists. The ICC value was 0.87 (range, 0.82–0.91) for bone marrow edema on MRI, 0.89 (range, 0.85–0.92) for detection of fractures on MRI, and 0.92 (range, 0.89–0.94) for detection of fractures on CT.
The overall sensitivity, specificity and accuracy of MRI for the detection of fracture (complete and incomplete) was 97.7, 92.3, and 95.7 %, respectively. The accuracy of MRI for the detection of complete fracture was 100 %. The sensitivity, specificity and accuracy of MRI for detection of incomplete fractures was 96.7, 92.0, and 94.6 %, respectively.
Compared to CT, MRI detected all 14 complete fractures and 30 of 31 incomplete fractures (24 with marrow edema and six without marrow edema). One incomplete fracture on CT was incorrectly graded ‘no fracture’ on MRI. This pars interarticularis, however, demonstrated bone marrow edema so was graded as a stress reaction on MRI. MRI detected stress reactions in a further six pars interarticularis that were occult on CT (Table 5).
MRI also accurately diagnosed in 23 of the 25 (92 %) no fracture cases on CT. MRI incorrectly diagnosed incomplete fractures with no bone marrow edema in two pars, which demonstrated no fracture on CT, leading to two false positives.
Other pathology such as disc disease, scoliosis, facet joint disease, Schmorl’s nodes and the incidence of paraesthesia was not recorded, as it was not within the scope of this study.
Discussion
It is well established that early diagnosis of spondylolysis is crucial to prevent spondylolisthesis [15–18]. There is currently no consensus on the optimal imaging pathway for assessing pars stress injuries.
Campbell et al. [8] suggested using MRI as the first-line investigation, followed by targeted CT in patients with acute defects, stress reactions, or in equivocal cases. This has been the conventional protocol used at our institution. MRI combines morphologic pars information with the presence or absence of bone marrow edema. This enables differentiation between acute stress reactions, active spondylolysis, and inactive chronic non-union. An added advantage of MRI is that patients receive no ionizing radiation. However, a disadvantage of MRI until recently is that osseous anatomy is not as well demonstrated as compared to CT. More recently, thin-slice 3D VIBE MRI has been used to provide near-isotropic resolution in three dimensions with a short acquisition time.
In this study, we have shown that 3D T1 VIBE sequence can be used for accurate assessment of pars bone morphology with comparable findings to CT. Our study demonstrates that 3-T MRI with thin-slice 3D T-1 VIBE sequence is 100 % accurate in diagnosing complete fractures. This is concordant with Ganiyusufoglu et al.’s [10] findings that MRI has a similar diagnostic accuracy to CT in detecting complete fractures with or without marrow edema in young patients (mean age 15).
Incomplete pars fractures are clinically important due to their potential to heal with conservative management [15–17]. In previous studies, incomplete fractures have been diagnostically challenging for MRI as osseous anatomy has until recently not been as well demonstrated as on CT. Our study has demonstrated a high accuracy (94.6 %) for detecting incomplete fractures, better than those previously published by Ganiyusufoglu et al. [10], Dunn et al. [19], and Campbell et al. [8]. Our improved results are attributed to the higher-strength 3-T MRI machine and the improved spatial resolution of the gradient-echo fine-slice 3D T-1 VIBE sequence over spin-echo T1-weighted imaging. Ganiyusufoglu et al. [10] only used the 3D T-1 VIBE sequence on a 1.5-T MRI scanner in their final nine of 105 cases. They found 3D T-1 VIBE correlated well with CT in showing the extent of fracture lines in both complete and incomplete fractures. These were, however, only performed in the lower lumbar spine and therefore they were not able to comment on the value of 3D T-1 VIBE for the upper lumbar levels. The majority of pars interarticular stress fractures are at L5, and L4, with these levels constituting 75 % of all fractures in our study. However, we have also shown that the 3D T-1 VIBE sequence has excellent diagnostic ability in the upper lumbar levels.
In our study, we had two false-positive cases diagnosed as incomplete fractures at L4 and L5 on MRI that were normal on CT. These normal pars were incorrectly graded as 2b stress injuries on MRI (chronic incomplete stress fractures). Theoretically, without the use of CT, this may have altered management. Interestingly, both false-positive gradings were in the same patient, a professional fast-bowling cricketer. CT demonstrated marked sclerosis of the two pars interarticulares, suggesting chronic stress lesions. On sagittal MRI, partial voluming and slight obliquity of the inferior pedicle and pars junction was mistakenly diagnosed as subtle incomplete fractures (Fig. 4a and b). In the future, more care has to be taken in interpreting pars that have cortical hypertrophy and sclerosis. It is possible that we were seeing remnants on an old incomplete fracture on MRI that is now healed on CT. In view that both false-positive results were at different levels in the same patient, it is thought that the patient’s anatomy played a role in the misdiagnosis. Of note, of the 70 pars assessed, there were only two false-positives and these both occurred in the same patient.

Sagittal 3-T MRI T-1 VIBE sequence (a) and inverted sagittal 3-T MRI T1 VIBE sequence (b) of the false-positive patient where the L5 pars demonstrated increased sclerosis at the inferior aspect of the pars, incorrectly diagnosed as chronic incomplete stress fracture on MRI
An L2 incomplete fracture (grade 2) on CT was incorrectly graded as a stress reaction, with bone marrow edema but an intact pars interarticularis cortex (grade 1) on MRI. Review of the case revealed that the patient was also a professional fast-bowling cricketer with marked hypertrophic sclerosis of the left L2 pars on both CT and MRI. The MRI occult and CT diagnosed subtle incomplete fracture involved the inferior lamina and pars junction. The fracture was best shown on the axial CT images, for which there were no MRI equivalent images in our study (Fig. 5). The slightly unusual anatomical location and the very subtle nature of the fracture may have been the reason that the fracture was detected on CT but missed on MRI. The left L2 pars interarticularis did however demonstrate bone marrow edema on MRI, resulting in the diagnosis of a stress reaction (grade 1). Theoretically, without the use of CT, this incorrect diagnosis of stress reaction (grade 1 instead of grade 2a) would still have afforded appropriate management.

Axial CT of the lumbar spine at L2 in a professional fast-bowling cricketer with marked hypertrophic sclerosis of the left L2 pars where a subtle incomplete fracture involving the inferior lamina and pars junction was seen only on CT, and was MRI occult
MRI diagnosed stress reactions without fractures in six pars, which is a diagnostic advantage of MRI over CT. These patients with early acute stress responses are in the best position to respond to conservative management. At our institution, the sports medicine clinicians believe that patients with either a pars stress reaction or acute incomplete fracture should be managed with a period of prolonged rest and no sport activities for an extended period of 3–6 months. This is to ensure that adequate time is given for the stress reaction to resolve or the incomplete fracture to unite, and to avoid a chronic defect and spondylolisthesis. In the setting of a chronic compete fracture, a prolonged period of rest is believed to be unnecessary as the fracture has a low probability of union. These patients are managed with a shorter period of rest (4 weeks) and symptomatic treatment with an earlier return to sporting activities.
We have performed serial MRIs in patients with stress fractures and have observed evolutional changes of these over time. With time, edema reduces in both fractures that heal and those that remain un-united. Non-united chronic fractures develop smooth corticated margins whilst healing chronic fractures have blurred and less well defined margins. Therefore, chronicity could be determined in the absence of information on the duration of symptoms.
For some institutions, MRI may be substantially more costly than CT, but we believe the added benefits of 3-T MRI with 3D T-1 VIBE sequence negate these costs by providing more rapid diagnosis of treatable pathology, i.e., in the diagnosis of pre-fracture stress edema and incomplete fractures whilst preventing the cost of an added, subsequent CT, given its similar diagnostic accuracy for fracture. Whilst 3D T-1 VIBE is an additional sequence to the conventional MRI lumbar spine sequence array, this only adds 4 min to the total scan time. This is performed at no extra cost to the patient.
Our study focused on the diagnostic accuracy of MRI in detecting pars stress fractures. We did not, within the scope of this project, follow up the fractures with MRI to assess for healing. Given the excellent accuracy of the 3D T-1 VIBE sequence, assessing pars stress fracture healing with only serial MRI could be assessed in a future study.
In conclusion, the diagnostic accuracy and characterization of lumbar spondylolysis by 3-T MRI using the thin-slice 3D T-1 VIBE sequence is very similar to CT. 3-T MRI with thin-slice 3D T-1 VIBE allows spondylolysis, a condition that occurs predominantly in young patients, to be diagnosed without ionizing radiation. The T-1 VIBE sequence has 100 % diagnostic accuracy in the detection of complete fractures and importantly, very high accuracy in the detection of incomplete pars stress fractures.
Given the strong performance of 3-T MRI with 3D T-1 VIBE, clinical practice could be changed so that only MRI is performed. Since the result of this audit, our local clinicians no longer request a CT scan due to their confidence in MRI being able to accurately detect and grade pars stress lesions. The omission of CT from the imaging pathway for assessing spondylolysis may result in significant economic and radiation dose savings for the community. In the future, 3-T MRI with 3D T-1 VIBE may be used as the initial and only imaging modality for young patients with pars interarticularis stress injury.
References
Jackson D, Wiltse L, Cirincione R. Spondylolysis in the female gymnast. Clin Orthop. 1976;117:658–73.
Soler T, Calderon C. The prevalence of spondylolysis in the Spanish elite athlete. Am J Sports Med. 2000;28:57–62.
Kim H, Green D. Spondylolysis in the adolescent athlete. Curr Opin Pediatr. 2011;23:68–72.
Kruse D, Lemmen B. Spine Injuries in the sport of gymnastics. Curr Sports Med Rep. 2009;8:20–8.
Elliot S, Hutson M, Wastie M. Bone scintigraphy in the assessment of spondylolysis in patients attending a sports injury clinic. Clin Radiol. 1988;39:269–72.
Lowe J, Schachner E, Hirschberg E, et al. Significance of bone scintigraphy in symptomatic spondylolysis. Spine. 1984;9:653–5.
Bellah R, Summerville D, Treves S, et al. Low back pain in adolescent athletes: detection of stress injury to the pars interarticularis with SPECT. Radiology. 1991;180:509–12.
Campbell R, Grainger A, Hide I, et al. Juvenile spondylolysis: a comparative analysis of CT, SPECT and MRI. Skeletal Radiol. 2005;34:63–73.
Hollenberg G, Beattie P, Meyers S, et al. Stress reactions of the lumbar pars interarticularis: the development of a new MRI classification system. Spine. 2002;27:181–6.
Ganiyusufoglu A, Onat L, Karatoprak O, et al. Diagnostic accuracy of magnetic resonance imaging versus computed tomography in stress fractures of the lumbar spine. Clin Radiol. 2010;65:902–7.
Leone A, Cianfoni A, Cerase A, et al. Lumbar spondylolysis: a review. Skelet Radiol. 2011;40:683–700.
Kobayashi A, Kobayashi T, Kato K, et al. Diagnosis of radiographically occult lumbar spondylolysis in young athletes by magnetic resonance imaging. Am J Sports Med. 2013;41:169–76.
Zheng Z, Shan H, Li X. Fat-Suppressed 3D T1-weighted gradient-echo imaging of the cartilage with a volumetric interpolated breath-hold examination. AJR. 2010;194:W414–9.
Thomson V, Pialat J, Gay F, et al. Whole-body MRI for metastases screening: a preliminary study using 3D VIBE sequences with automatic subtraction between non contrast and contrast enhanced images. Am J Clin Oncol. 2008;31:285–92.
Blanda J, Bethem D, Moats W, et al. Defects of pars interarticularis in athletes: a protocol for nonoperative treatment. J Spinal Disord. 1993;6:406–11.
Steiner M, Micheli L. Treatment of symptomatic spondylolysis and spondylolisthesis with the modified Boston brace. Spine. 1985;10:937–43.
Morita T, Ikata T, Katoh S, Miyake R. Lumbar spondylolysis in children and adolescents. J Bone Joint Surg (Br). 1995;77:620–5.
McCleary M, Congeni J. Current concepts in the diagnosis and treatment of spondylolysis in young athletes. Curr Sports Med Rep. 2007;6:62–6.
Dunn A, Campbell R, Mayor P, et al. Radiological findings and healing patterns of incomplete stress fractures of the pars interarticularis. Skelet Radiol. 2008;37:443–50.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Ang, E.C., Robertson, A.F., Malara, F.A. et al. Diagnostic accuracy of 3-T magnetic resonance imaging with 3D T1 VIBE versus computer tomography in pars stress fracture of the lumbar spine. Skeletal Radiol 45, 1533–1540 (2016). https://doi.org/10.1007/s00256-016-2475-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-016-2475-7