
Abstract
Background
Pediatric magnetic resonance imaging (MRI) can be stressful. Mock MR scanners have been proven to be effective in avoiding the use of general anesthesia.
Objectives
We prospectively evaluated the impact of a teddy bear-scale model of a mock MR scanner on the anxiety experienced by parents and their children during MRI without general anesthesia .
Materials and methods
A 1-year prospective study before and after the installation of a mock scanner in a Pediatric Radiology Department of a university hospital. Anxiety levels were self-estimated by children ages 4 to 16 years and by the parents with a visual analogue scale (from 0, completely relaxed, to 100, extremely stressed) at three moments: in the waiting room, in the preparation room after an explanation by the MRI technologists, and at the issue of the MR acquisition images. Two groups were tested: one with a mock MR scanner, the other without. Analysis of variance (ANOVA) and Fisher exact tests were performed. Motion artifacts were studied.
Results
Ninety-one children and their parents were included. The median age was 8 years (standard deviation [SD]=2). In the post mock period, the ambiance of the preparation room was considered by children as significantly more relaxing in 50% vs. 20% (P=0.004) and the anxiety level of children was significantly lower after the explanation, particularly in girls, but unchanged for their parents. The anxiety levels at the end of the examination were significantly lower for parents. The motion artifacts rate was lower (1.7% vs. 4.7%, P=0.04).
Conclusion
A mock scanner was an efficient tool to improve efficiency of the explanation and to decrease anxiety in children and motion artifacts in pediatric MRI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Magnetic resonance imaging (MRI) is considered a safe and precise imaging method in children. However, its accuracy requires the absence of any movement and good compliancy by the child during the examination. MRI can lead to mild to severe anxiety due to the confined space, difficulty lying still in the magnet, the eventuality of an intravenous injection, the loud noises from the switching gradient and the overall length of time necessary for the examination [1, 2].
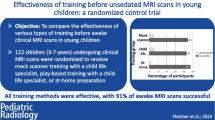
To obtain the best image quality, children must be calm and motionless [3, 4]. An efficient preparation of the child before an MRI is crucial to reduce anxiety and ensure cooperation [5]. Cahoon and Davison [6] reported that noncompliance was related to child attention problems and to poor adaptability. For neonates, a simple “feed and sleep” is enough to undergo the MRI examination. In older children, a wide range from minimal sedation (anxiolysis), moderate sedation (conscious sedation) and deep sedation (analgesia) through to general anesthesia is available. However, reducing the need for sedation for MRI would improve patient safety and reduce the cost and risk of adverse reaction to medications used for anesthesia or sedation [7, 8]. To avoid these associated dangers, alternative techniques already exist: sucrose and pacifier, gentle swaddling and practice MRI [9]. An oral explanation given by the MRI technologist helps toward a better understanding of the MRI examination. DVDs, storybooks or information sheets can also provide relevant information at appropriate ages, using cartoons to illustrate the workings of the MRI [10, 11]. However, a study evaluating educational materials before MRI in 52 school-age children and their parents did not reduce child or parental anxiety levels [12]. A randomized controlled trial comparing the use of cognitive behavioral therapy to standard care did not find any statistically significant difference in the rate of sedation for the clinical MRI [13]. Play-based therapy offers children an explanation of their procedure. Practice MRI intervention facilitated by educational play therapists is useful in helping children cope with MRI without general anesthesia [14]. Visiting a real-size mock scanner before the appointment may be useful and lead to a high rate of imaging success: The scans of 81 out of 90 children were between acceptable and excellent in quality following simulator training sessions [15]. A Carter et al. [16] study reported that mock MRI reduced the need for general anesthesia in children with the greatest effect evident in children ages 3 to 8 years. However, in previous studies, no detailed study on the anxiety level of children and their parents during the different steps of the MRI examination was performed.
The aim of our study was to prospectively evaluate the impact of an explanation helped with a teddy bear-scale model of a mock MR scanner installed in a child-friendly preparation room focused on the self-estimation of the anxiety level of parents and their children who are having an MRI. Artifact motions and image quality were studied as secondary elements.
Materials and methods
Study population
This prospective controlled trial was performed from March 2018 to March 2019. All children ages 4 to 16 years who presented to our ambulatory tertiary center for an MRI scan were included, provided that they had a normal level of understanding expected for their age and had parents who agreed to participate in the research. The study period was divided according to the period following the installation and establishment of the mock MRI (from March 2018 to September 2018) and a comparable time thereafter (from October 2018 to March 2019). These two time periods are referred to as pre-mock periods and post-mock periods.
Children were excluded because of severe cerebral palsy, severe attention deficit hyperactivity disorder or a lack of communication skills. All participants provided written informed consent after the study aims and procedures were fully explained. The study was approved by the Local Ethics Committee (RNI – 2019-019). The study complied with the Declaration of Helsinki.
MRI data
There were no significant changes in scan techniques during the study period. The length of examination, number of sequences, artifact motions and image quality were tabulated. The time of preparation and explanation by the MRI technologist was determined as 5 min for every child and their parents. The examination time was determined as time on the MR table between the beginning of the first sequence and the end of the last sequence.
Mock MRI scanner
Our mock MRI scanner has been specially designed to look like a toy, specially designed for use with young children, adapted to easy handling both by its teddy bear size and materials: wood, plexiglass and cotton fabric. The mock MR was as realistic as possible, with a removable head antenna, gentle contention and a stereo system diffusing MRI sequence sounds to accustom children to the loud noises (Fig. 1).

Photograph of our teddy bear-scale model of a mock MRI scanner in the preparation room
Procedures
In the pre-mock and post-mock periods, a written form with adapted language was given to the child and their parents to complete. The ambiance of the preparation room was evaluated with a four-point Likert scale (relaxing, neutral, frightening, scary). The anxiety level was self-estimated with a visual analogue scale (from 0, completely relaxed, to 100, extremely stressed) at three different moments: in the waiting room, in the preparation room after an explanation by the MRI technologists and at the issue of the MR acquisition images. Overall appreciation of the MRI examination was collected at the end of the procedure. Free comments were welcome.
The only difference between the two periods was the use of a teddy bear-scale model of the mock MR scanner for the explanation given by the MRI technologists. The intervention pre/post mock was delivered by the same staff members composed of experienced MRI technologists. The preparation script was identical in both conditions. We invited children to take a teddy bear (MR compatible) into the MRI as they themselves would be able to do the same day in the real MRI scanner. They also were encouraged to keep the teddy bear in their arms during the MRI examination.
Statistical analysis
An MRI test was defined as successful when it yielded interpretable results by a pediatric radiologist and did not require general anesthesia. Median ages were compared between patient groups by the Mann-Whitney-Wilcoxon test. P-values less than 0.05 were considered statistically significant. Statistical analysis was performed using R software [17] and Statistica®. The statistical analysis of the anxiety score included a General Linear Model analysis of variance (ANOVA) with repeated measures (Time factor=3 anxiety scores: in the waiting room, after an explanation by the MRI technologists and after the MR exam). The analysis included two factors (gender [M or F] and mock [mock or no-mock]) and a covariate (age). Two analyses were performed: one for anxiety scores evaluated by parents, one for anxiety evaluated by their children. Greenhouse-Geisser (G-G) corrections were performed and the homogeneity of variances was verified by a Levene analysis.
Results
Study population
Ninety-one children (46 girls and 45 boys) and their parents were included (44 in the pre-mock and 47 in the post-mock period). Questionnaires were given randomly in 20% of the cases. Participation rate was 95%. The two groups were comparable with no significant difference in age or gender. The median age was 8 years (standard deviation [SD]=2).
MRI data
All MRI examinations were interpretable. Minimal sedation (hydroxyzin) was prescribed by clinicians depending on the attended compliance of children in 12 cases and 17 cases in pre- and post-mock periods. The mean time of examination was 28 min (SD: 7 min) in the pre-mock period and 24 min (SD: 5 min) in the post-mock period. Three hundred thirty-eight sequences were acquired in the pre-mock period and 343 in the post-mock period. Intravenous injection was required in 12/44 cases in the pre-mock period and in 7/47 in the post-mock period. Motion artifacts were observed in 16 cases (4.7%) and 6 cases (1.7%) in the pre- and post-mock periods, respectively (Fisher exact test, P=0.04).
Questionnaires
The ambiance of the preparation room was considered by children as significantly more “relaxing” in 50% in the post-mock period vs. 20% (Fisher exact test P=0.004).
The ANOVA did not revealed any main effect on the anxiety level estimated by children but showed an interaction of time x gender (dll=2, F=3.441, P=0.034, G-G adjusted P=0.043) and an interaction time x mock (dll=2, F=3.441, P=0.029, G-G adjusted P=0.037).
Post hoc tests (Scheffé) showed that the anxiety level estimated by children was significantly lower after the explanations in the post-mock period (P<0.0001) as compared to the level estimated in the waiting room (no difference for waiting room versus after explanation in the pre-mock condition). In pre- and post-mock periods, a significant difference between anxiety score in the waiting room and after the exam was also observed (pre-mock period: P<0.001, post-mock period: P<0.0000001).
Post hoc also revealed that the anxiety score after the exam was significantly lower for boys (P<0.05) and girls (P<0.0000001). Furthermore, a difference was also observed between anxiety score in the waiting room and the score after explanation only in girls (P<0.05).
Concerning the score estimated by the parents, the analysis only revealed a main effect of time (dll=2, F=5.166, P=0.007, G-G adjusted P=0.08).
The anxiety levels of children and their parents are provided in Figs. 2 and 3, respectively. The anxiety level depending on gender is provided in Fig. 4.

Mean child anxiety level evaluation in the waiting room, the preparation room and at the end of the MRI

Mean parent anxiety level evaluation in the waiting room, the preparation room and at the end of the MRI

Mean anxiety level evaluation of girls and boys in the waiting room, the preparation room and at the end of the MRI
Children and parents gave free comments: Five people thanked the department for this initiative. They also reported that they understood the MRI device much better. One child explained that he was still afraid of the possibility of having an intravenous injection during the examination.
Discussion
The results of our prospective clinical trial suggested that a teddy bear-scale model of a mock MR scanner helped MRI technologists significantly reduce the anxiety level of the children before undergoing an MRI examination and induce a secondary benefit with a significant lower rate of motion artifacts, with a similar time of explanation during the preparation. Reduction in examination time was due to the fewer repeated sequence due to motion artifacts. The efficiency of the explanation was significantly greater with the mock MRI. Our motion artifacts rate was also slightly lower than the 2% previously reported in the Carter et al. [16] study. It could be explained by a more relaxed child when being installed in the MRI. As they were encouraged to take the teddy bear in their arms, the toy kept them concentrated on a specific task and so the children were distracted from the imaging process. It led to greater confidence in the MR procedure. Reducing anxiety during a medical examination has probably reduced its short-term negative effects (crying, movements, lack of cooperation). It also should reduce its potential long-term impact: post-traumatic stress syndrome, fear, avoidance of imaging examinations. The residual anxiety level in our study could possibly be explained by the suspected pathology corresponding to the medical indication of the MRI and the fear about the MR results. Contrary to previous studies [12], we did not observe inadvertent increased anxiety levels after providing an explanation. One child reported anxiety due to the possibility of having an intravenous injection.
Although we did not observe a modification of the parent’s anxiety levels after the explanation, we noticed that, contrary to the Hartman et al. [12] study, their anxiety levels at the end of the MRI examination were significantly lower. We could suggest that parental anxiety was not caused by the technical part of the images acquisition, but mainly by their child’s behavior during the examination and also by the pathology of their child.
Advantages of our preparation procedure were its simplicity and its rapidity. We do not need several training sessions to decrease the anxiety level of the children. The use of a MR-compatible teddy bear allowed children to use it with the mock MR scanner, and then, keep it in their arms during the real MRI examination. The teddy bear distracted the child from the imaging process.
The strength of the present study was its prospective study design, which compared outcomes of an MRI technologist’s explanation with or without a mock MR scanner for children and their parents. The high rate of participation has limited the impact of the possibility that children or parents who chose not to participate in the study were likely to be less anxious. The absence of any statistically significant differences between both study groups supports a lack of selection bias in our sample. Our child population was representative of a general pediatric hospital’s recruitment and our results could be useful for any radiologic center performing pediatric MR examinations.
The age range of children participating in this trial was 4 to 16 years. We acknowledge that only a few healthy children ages 12 to 16 years old would require any sedation for an MR scan [6], but they appreciated the clarity of the MRI technologist. Even children who had already undergone an MRI examination were more curious about the technical aspects and asked questions they had not asked before the mock MRI.
A limitation would be the difficulty to obtain a fully randomized control design study since the children received the same information during a similar MR preparation script albeit delivered by potentially different MR technologists.
In the post-mock period, MR technologists and patients were more aware of the effort to reduce anxiety in the preparation room. This phenomenon has clearly influenced the results, but we do not know by what magnitude.
Conclusion
Anxiety levels before the MRI examination were lower in children after the installation of our teddy bear-scale model of a mock MR scanner with a similar time of explanation during the preparation without several training sessions. Secondary benefits were a significant lower rate of motion artifacts in MRI and reduced anxiety of the parents at the end of the MR examination.
References
Tyc VL, Fairclough D, Fletcher B et al (1995) Children’s distress during magnetic resonance imaging procedures. Child Health Care 24:5–19
Marshall SP, Smith MS, Weinberger E (1995) Perceived anxiety of pediatric patients to magnetic resonance. Clin Pediatr (Phila) 34:59–60
American Society of Anesthesiologists Task Force on sedation and analgesia by non-anesthesiologists (2002) practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology 96:1004–1017
Sury M, Bullock I, Rabar S et al (2010) Sedation for diagnostic and therapeutic procedures in children and young people: summary of NICE guidance. BMJ 341:c6819
Cejda KR, Smeltzer MP, Hansbury EN et al (2012) The impact of preparation and support procedures for children with sickle cell disease undergoing MRI. Pediatr Radiol 42:1223–1228
Cahoon GD, Davison TE (2014) Prediction of compliance with MRI procedures among children of ages 3 years to 12 years. Pediatr Radiol 44:1302–1309
Cravero JP, Beach ML, Blike GT et al (2009) The incidence and nature of adverse events during pediatric sedation/anesthesia with propofol for procedures outside the operating room: a report from the pediatric sedation research consortium. Anesth Analg 108:795–804
Sanborn PA, Michna E, Zurakowski D et al (2005) Adverse cardiovascular and respiratory events during sedation of pediatric patients for imaging examinations. Radiology 237:288–294
Edwards AD, Arthurs OJ (2011) Paediatric MRI under sedation: is it necessary? What is the evidence for the alternatives? Pediatr Radiol 41:1353–1364
Bratton SC, Ray D, Rhine T, Jones L (2005) The efficacy of play therapy with children: a meta-analytic review of treatment outcomes. Prof Psychol Res Pract 36:376–390
Russell C, Smart S (2007) Guided imagery and distraction therapy in paediatric hospice care. Paediatr Nurs 19:24–26
Hartman JH, Bena J, McIntyre S, Albert NM (2009) Does a photo diary decrease stress and anxiety in children undergoing magnetic resonance imaging? A randomized, controlled study. J Radiol Nurs 28:122–128
Tyc VL, Leigh L, Mulhern RK et al (1997) Evaluation of a cognitive-behavioral intervention for reducing distress in pediatric cancer patients undergoing magnetic resonance imaging procedures. Int J Rehabil Health 3:267–279
Hallowell LM, Stewart SE, de Amorim E et al (2008) Reviewing the process of preparing children for MRI. Pediatr Radiol 38:271–279
de Bie HMA, Boersma M, Wattjes MP et al (2010) Preparing children with a mock scanner training protocol results in high quality structural and functional MRI scans. Eur J Pediatr 169:1079–1085
Carter AJ, Greer ML, Gray SE, Ware RS (2010) Mock MRI: reducing the need for anaesthesia in children. Pediatr Radiol 40:1368–1374
R Foundation (2015) R: A language and environment for statistical computing. Vienna, Austria; 2014. http://www.r-project.org (Accessed 7 August 2019)
Acknowledgments
We thank the participating children and their families, all the MRI technologists at Tours University Hospital Center and Elodie Gaspard. We are especially grateful to Elodie Semelier and Marie Claude Santini from the Pharmavie Association and Laura Elharrar.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Morel, B., Andersson, F., Samalbide, M. et al. Impact on child and parent anxiety level of a teddy bear-scale mock magnetic resonance scanner. Pediatr Radiol 50, 116–120 (2020). https://doi.org/10.1007/s00247-019-04514-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-019-04514-1