
Abstract
Narrow duplicated internal auditory canal (IAC) is a rare malformation of the temporal bone that is associated with ipsilateral congenital sensorineural hearing loss. This may be an isolated finding or a part of a syndrome. Radiological examination should demonstrate aplasia or hypoplasia of the neural components of the narrow IAC, to guide the surgical approach. We report a 7-year-old boy with Klippel-Feil syndrome with a narrow double IAC with no sensorineural hearing loss but with conductive hearing loss. In this patient, the IAC consisted of two separate narrow bony canals clearly seen on 3D temporal bone CT and one nerve that was delineated on MRI. The contralateral external auditory canal was stenotic and the ossicles were dysplastic.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Internal auditory canal (IAC) anomalies, including atresia, stenosis, aplasia and hypoplasia, are all uncommon; only 20% of the patients with congenital sensorineural hearing loss (SNHL) have inner ear abnormalities visible on CT. Anomalies are usually unilateral and are associated with other inner ear, middle or external ear anomalies [1–3]. A narrow IAC is defined as an IAC with a diameter of 1–2 mm on high-resolution CT (HRCT) [4, 5]. This anomaly is believed to be the result of aplasia or hypoplasia of the vestibulocochlear nerve [1, 2, 4]. A narrow duplicated IAC is very rare with only four cases in the literature [4]. We present a case of unilateral narrow duplicated IAC and contralateral narrow external auditory canal (EAC).
Case report
A 7-year-old boy with Klippel-Feil syndrome presented with deterioration of hearing. He had been fitted with a bone conduction hearing aid in another institution because of bilateral hearing loss at the age of 3 years. Physical examination revealed the scar of a cleft lip and palate operation that had been performed at the age of 1 year. Type I microtia with a slightly stenotic external ear canal on the right and type II microtia with a severely stenotic external ear canal impeding visualization of the tympanic membrane on the left side were confirmed. The remainder of the head and neck examination was normal except for a short neck and low posterior hairline. The patient did not have a facial palsy. Speech and language development were minimally retarded. His mother denied any symptom that would suggest vestibular impairment.
After complete audiological examination that revealed bilateral asymmetrical severe conductive hearing loss, high resolution axial, coronal, reformatted sagittal and 3D CT images of the temporal bones were obtained. For further evaluation of the seventh and eighth cranial nerves, MRI was performed using a 1.5-T MRI system. The temporal bone imaging protocol included T2-weighted spin-echo axial (TR/TE 2200/20; 4 mm slice thickness), T1-weighted spin-echo coronal (TR/TE 635/15; 3 mm slice thickness), 3D balanced fast field echo (B-FFE) axial (TR/TE 8/4; flip angle 50°; 0.6 mm slice thickness; matrix 192×256; 150 mm field of view; signal averaging 3) sequences. Sagittal, parasagittal and coronal reformatted images were obtained.
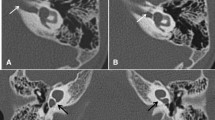
On temporal bone CT there were two narrow bony canals in the inner ear portion of the right temporal bone. Measured diameters of these bony canals were less than 1 mm. Three-dimensional reformatted CT images clearly delineated the two canals (Fig. 1). The cochlea, vestibule and semicircular canals were interpreted as normal. The facial nerve canal was intact along its course in the middle ear. The middle and external ear structures demonstrated no other abnormality. On the left side the EAC was stenotic (Fig. 2). The ossicles in the middle ear were dysplastic. The other middle and internal ear components of the temporal bone appeared normal. Axial and reformatted coronal images demonstrated normal cranial nerves in the left IAC and normal membranous labyrinth structures. On the right there was a single thin cranial nerve identified as the facial nerve on multiplanar reformatted images (Fig. 3). The right membranous labyrinth was unremarkable on MRI. The child was fitted with a new bone conduction hearing aid and he has continued to benefit from conventional hearing amplification.

Right temporal bone contiguous axial HRCT (a, b) and 3D lateral view (c) images show narrow duplicated IAC (arrows)

Left temporal bone; axial (a) and coronal (b) HRCT with 3D lateral view (c) images show normal-sized left IAC (arrow). The left EAC is narrow and obstructed with soft tissue. The space between the left ossicles and the tympanic bony wall is also very narrow

Contiguous coronal 3D B-FFE MR images demonstrate normal left seventh/eighth cranial nerve complex (black arrows on left). The IAC is seen on the right side (white arrow). There is only one nerve seen through the right IAC (small black arrows)
Discussion
A narrow IAC is a rare malformation of the temporal bone which is frequently associated with various systemic developmental anomalies including cardiac, renal, skeletal and intestinal malformations [4]. IAC anomalies can also be components of some syndromes—Michel, Mondini, Bing-Sieberman, Scheibe and Klippel-Feil. Congenital IAC stenosis should be considered after certain predisposing conditions (exostosis, Paget disease and trauma) have been excluded. The association of IAC stenosis or atresia and congenital SNHL is unclear. Some patients with unilateral IAC stenosis may have normal hearing bilaterally while others may suffer hearing loss in the ear without stenosis [5]. In addition, the diameter of the IAC varies greatly among healthy individuals.
Development of the inner ear begins at 22 days of gestation as a thickening of the otic placode that later forms the otocyst from which the audiovestibular structures originate. The fibres of the eighth nerve grow and come in contact with the otocyst on day 37. During the eighth week of gestation, the seventh and eighth nerves become involved in the mesoderm which forms the bony canal by chondrification and ossification [5].
One hypothesis suggests that the primary defect is bony stenosis and this causes aplasia or hypoplasia of the eighth nerve, but the usually normal appearance of the facial nerve is in contradiction to this hypothesis. Interestingly, in most cases with stenotic IAC, facial nerve function is preserved. According to the other widely accepted hypothesis, the embryonic cochlea and vestibule induces the growth of the eighth nerve and the bony canal develops around the nerve together with the seventh nerve by chondrification and ossification of mesoderm in the eighth week of gestation. When the eighth nerve is aplastic or hypoplastic the IAC fails to develop [1].
CT has a high sensitivity when evaluating the bony structures of the IAC and temporal bone. The vertical diameter of the IAC varies between 4 and 8 mm; less than 2 mm is considered stenotic [6]. A stenotic IAC does not contain a nerve but a hypoplastic IAC may contain a vestibulocochlear nerve with abnormal nerve function [2]. A normal sized IAC does not imply normal vestibulocochlear nerve development. CT has a limited role in assessing the neural elements in the bony canal. As imaging capabilities improve it is now possible to confirm the presence or absence of neural structures by MRI, which provides more detailed information about the IAC and its soft tissue contents [7].
Table 1 summarizes previously reported narrow duplicated IAC anomalies. The first was reported in 1997 by Casselman et al. [7] who described a unilateral duplicated narrow IAC with a superior portion containing normal facial nerve and an empty inferior portion. There was no labyrinthine abnormality. The second was reported by Vilain et al. [8] in 1999. They described an empty unilateral narrow IAC and an anterior superior second canal where the facial and vestibulocochlear nerves were present. The third was reported by Cho et al. [2] in 2000, and was similar to the first case. In 2003 Ferreira et al. [4] reported a narrow duplicated IAC containing only the facial nerve. This patient also had a bilateral abnormally enlarged vestibule and a lateral semicircular canal and a dysplastic cochlea.
In our patient there were two highly stenotic bony canals in the right temporal bone and no vestibular or cochlear abnormality, similar to the patients reported by Casselman et al. [7] and Cho et al. [2]. Three-dimensional verification of the bony canals was made using 3D CT images. On B-FFE MRI only one nerve was identified through the narrow canals in the subarachnoid space. Assessment of the normal cochlear nerve is necessary when making a decision for implantation surgery [9]. Patients who do not have cochlear nerves cannot respond to the electric stimulation of cochlear implantation [3, 10]. Although audiological examination of our patient did not reveal SNHL, but conductive type of hearing loss, the right cochlear nerve was not seen on MRI. This may have been related to the smaller size of the cochlear nerve on the right side. Although the vestibulocochlear nerve and IAC were seen to be normal on the left side, the left EAC was stenotic and the ossicles were dysplastic. As a result of these bilateral temporal bone abnormalities the patient continued to benefit from conventional hearing amplification.
In conclusion, congenital deafness has many different aetiologies. A narrow duplicated IAC is an unusual finding, which has to be examined radiologically to demonstrate the neural components of the IAC in case of congenital hearing loss. Only after detailed radiological examination, including high resolution axial, reformatted coronal, sagittal 3D reconstructed CT and MRI imaging for the vestibulocochlear nerves, can the appropriate treatment be planned.
References
Yates JA, Patel PC, Millman B, et al (1997) Isolated congenital internal auditory canal atresia with normal facial nerve function. Int J Pediatr Otorhinolaryngol 41:1–8
Cho YS, Na DG, Jung JY, et al (2000) Narrow internal auditory canal syndrome: parasagittal reconstruction. J Laryngol Otol 114:392–394
Camacho RR, Berrocal JR, Arellano B (2001) Bilateral malformation of the internal auditory canal: Atresia and contralateral transverse megacrest. Otolaryngol Head Neck Surg 125:115–116
Ferreira T, Shayestehfar B, Lufkin R (2003) Narrow, duplicated internal auditory canal. Neuroradiology 45:308–310
Rothschild MA, Wackym PA, Silvers AR, et al (1999) Isolated primary unilateral stenosis of the internal auditory canal. Int J Pediatr Otorhinolaryngol 50:219–224
Valvassori GE, Pierce RH (1964) The normal internal auditory canal. AJR 92:1232–1241
Casselman JW, Offeciers FE, Govaerts PJ, et al (1997) Aplasia and hypoplasia of the vestibulocochlear nerve: diagnosis with MR imaging. Radiology 202:773–781
Vilain J, Pigeolet Y, Casselman LW (1999) Narrow and vacant internal auditory canal. Acta Otorhinolaryngol Belg 53:67–71
Maxwell AP, Mason SM, O’Donoghue GM (1999) Cochlear nerve aplasia: its importance in cochlear implantation. Am J Otol 20:335–337
Shelton C, Luxford WM, Tonokawa LL, et al (1989) The narrow internal auditory canal in children: a contraindication to cochlear implants. Otolaryngol Head Neck Surg 100:227–231
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Demir, Ö.İ., Cakmakci, H., Erdag, T.K. et al. Narrow duplicated internal auditory canal: radiological findings and review of the literature. Pediatr Radiol 35, 1220–1223 (2005). https://doi.org/10.1007/s00247-005-1547-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-005-1547-y