
Abstract
Background
Dose reduction by combined tube current modulation has not been evaluated in pediatric low-dose CT.
Objective
This study was performed to evaluate tube current reduction in non-ECG-gated heart CT angiography in children by combined tube current modulation, and to assess the effects of body weight, age, sex, and scan direction on tube current reduction.
Materials and methods
From September 2004 to January 2005, non-ECG-gated heart CT examinations were performed with combined tube current modulation in 50 children (median age 1 year, range 1 month to 16 years; M/F 29/21) with congenital heart disease. Sixteen-slice spiral CT studies were obtained using a weight-based low-dose protocol (80 kVp, 50–160 effective mA). CT scans were obtained in the craniocaudal direction when leg veins (n=36) were used for IV injection of contrast agent and in the caudocranial direction when arm veins (n=13) were used. In one child who underwent a Fontan operation, both arm and leg veins were used. We calculated tube current reduction by combined tube current modulation and evaluated the effects of body weight, age, sex, and scan technique on tube current reduction. The quality of CT angiography images was visually evaluated by an experienced pediatric radiologist.
Results
Overall tube current reduction by combined tube current modulation was 15.8±11.1%. The reduction was variable among five body weight groups (9.3±7.9% for <4.9 kg, 14.3±9.3% for 5.0–9.9 kg, 16.4±12.5% for 10.0–19.9 kg, 25.8±9.8% for 20.0–39.9 kg, 15.9±12.7% for 40.0–59.9 kg) and was significantly different among the five groups (P=0.017). When eight children in the 40.0–59.9-kg group were excluded, age showed a significant positive correlation with tube current reduction (γ=0.4, P=0.003). There was no significant difference in tube current reduction between boys and girls. Tube current reduction was significantly greater for the caudocranial scan (21.2±9.2%) than for the craniocaudal scan (14.2±11.3%) (P=0.049). All CT angiography images were of diagnostic quality.
Conclusions
Combined tube current modulation reduced tube current in pediatric non-ECG-gated heart CT by 15.8% without degradation of image quality. With our CT protocol, for body weights up to 39.9 kg, age showed a significant positive correlation with tube current reduction, but there was a lower dose-saving effect in children heavier than 40 kg. Tube current reduction was not affected by sex, but was affected by scan direction.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The importance of dose -reduction has been emphasized particularly in pediatric CT [1–3]. Various strategies have been described for CT dose reduction [3–9], and among them the use of a body size-adaptive CT protocol [6, 7], a low tube voltage [8], and tube current modulation [9] have been highly recommended in children. Thus, a weight-based pediatric CT protocol using a variable tube voltage and a variable tube current, which was established to achieve a diagnostic level of image noise for each body part, has been employed in our department [3]. In body CT angiography, the simultaneous use of a low tube voltage (80 or 100 kVp) and a high concentration of iodinated contrast agent (370 mg I/ml) has been found to be synergistically beneficial. In addition, tube current modulation is routinely applied to all CT studies including non-ECG-gated heart CT. Tube current modulation is a technique that allows dose reduction without significant loss of image quality enabling the efficient use of CT radiation by adjusting tube current according to the size and attenuation characteristics of the scanned body part of the patient [9]. The technique is classified into angular modulation (along the x–y plane), z-axis modulation (along the z-axis), and combined modulation (along the x–y plane and the z-axis).
Since the introduction of multislice CT in 1998, the clinical applications of heart CT have substantially increased [10]. At our institution, the three major clinical indications for CT in congenital heart disease are: (1) the morphological evaluation of the pulmonary circulation in patients with tetralogy of Fallot or pulmonary atresia with ventricular septal defect and major aortopulmonary collateral arteries, (2) the morphological evaluation of the aortic arch, and (3) evaluation of airway vascular compression. In patients with congenital heart disease, non-ECG-gated heart CT has been reported to be useful not only in the morphological evaluation of cardiovascular defects, but also in the evaluation of associated lung, airway and pleural abnormalities [11–14]. Moreover, heart CT has the advantages of a shorter examination time, less requirement for sedation or general anesthesia, and easier patient monitoring, as compared with MRI. However, the use of ionizing radiation in CT is a concern, especially in children. In addition to a body size-adaptive low-dose CT protocol, radiation dose may be further reduced by means of tube current modulation. However, dose reduction and resulting image quality by combined tube current modulation in pediatric low-dose CT have not, to our knowledge, been evaluated. Therefore, this study was performed to evaluate dose reduction in non-ECG-gated heart CT by combined tube current modulation in children, and to assess the effects of body weight, age, sex, and scan direction on dose reduction.
Materials and methods
Our institutional review board approved this study and informed consent was waived. From September 2004 to January 2005, non-ECG-gated heart CT examinations were performed with combined tube current modulation (CARE Dose 4D; Siemens, Forchheim, Germany) in 50 consecutive children (median age 1 year, range 1 month to 16 years; M/F 29/21) with congenital heart disease. CT scans were performed for preoperative evaluation in 27 children and for postoperative evaluation in 23 children. General indications for the examination were as follows: pulmonary artery (n=24), aorta (n=14), airway (n=7), anomalous pulmonary venous drainage (n=4), and cardiac tumor (myocardial hemangioma; n=1). The tube current modulation used in this study was based on the combined use of angular modulation and z-axis modulation. In angular modulation, tube current is adjusted along the x–y plane by online monitoring of the attenuation with a delay of 180° or 360° from the X-ray generation angle. In z-axis modulation, tube current is adjusted along the z-axis by using localizer radiograph projection data. In combined modulation, tube current is adjusted to maintain a user-selected image noise level. Three options (strong for an obese patient, average for a standard patient, or weak for a slim patient) were provided for strength of modulation in the CT system. We chose average strength, which is the default.
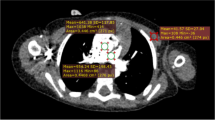
Sixteen-slice spiral CT studies (Somatom Sensation 16; Siemens) were obtained using a weight-based low-dose protocol (Table 1). Depending on arm positions of young children who were sleeping or shallowly sedated during the scan, 5–15 effective mAs was added to the reference effective mAs in order to avoid degradation of image quality because of inclusion of their arms in the scan range (Fig. 1). Spiral CT data were acquired with a 0.75-mm detector collimation, 0.75-mm slice width, 0.5-mm reconstruction interval, 12-mm table feed or with a 1.5-mm detector collimation, 2-mm slice width, 0.7-mm reconstruction interval, and 24-mm table feed, as required for z-axis coverage or breath-hold time. In terms of reconstruction algorithm or kernel, B20f was used for the first body weight group (<4.9 kg) and B30f was used for the other groups. The minimum gantry rotation time of 375 ms was chosen for maximum reduction of motion artifacts.

Three steps in calculating tube current reduction by combined tube current modulation
For optimum vascular opacification, a dual power injector [1.3 ml/kg of iodinated contrast agent (370 mg I/ml) followed by a saline chaser] and automatic bolus tracking system were used. A round region of interest was placed in the left ventricular cavity, and the threshold for CT density was set at 200 HU. The injection rate was determined by a total injection time in the range 25–30 s. CT scans were obtained in the craniocaudal direction when leg veins (n=36) were used for IV injection of contrast agent and in the caudocranial direction when arm veins (n=13) were used. The caudocranial direction was to minimize streak artifacts from undiluted contrast agent in the central thoracic veins when an arm injection was performed. A child with a Fontan operation had both arm and leg veins injected simultaneously and a caudocranial scan was obtained. In young or uncooperative children, oral or IV sedation was administered, as necessary; pulse oximetry was used according to our departmental guidelines. No patient required general anesthesia.
We calculated tube current reduction from combined tube current modulation by comparing tube currents with and without tube current modulation (Fig. 1). Because we used a fixed voltage setting (80 kVp), reduction in tube current might have been closely proportional to reduction in radiation dose. Absolute radiation dose, which is affected by compound factors including patient size, was not measured. Records of CT dose index volume or dose length product displayed on the CT console at the time of scanning were not available because of the retrospective nature of this study. First, we estimated standard tube current (mA per second) which would be given to a child when tube current modulation would not be used, and the value was calculated by dividing effective mAs by gantry rotation time (375 ms). As a next step, percentage tube current reduction was calculated slice by slice from estimated tube current without modulation and real tube current with modulation, and then percentage tube current reductions of all slices were averaged for each child. We then evaluated the effects of body weight, age, sex, and scan direction on tube current reduction. Because this study was a retrospective study and we did not keep a record of actual body weight at the time of the CT scan, correlation between body weight and tube current reduction by modulation could not be analyzed. Nevertheless, tube current reduction of each body weight group could be compared with those of other body weight groups by means of analysis of variance. Tube current reduction by combined tube current modulation was correlated with patient age by means of a Spearman’s test. A paired t-test was used to compare the reductions between boys and girls, and to compare those between the two scan directions (craniocaudal vs. caudocranial). P values less than 0.05 were considered statistically significant.
The quality of CT angiography images was visually evaluated and graded using a three-point scale (1 non-diagnostic images degraded by high image noise, 2 noisy but still diagnostic images, 3 diagnostic images without noticeable image noise) by an experienced pediatric radiologist with 5 years experience of non-ECG-gated heart CT. The major extracardiac vessels, including the aorta, pulmonary arteries and pulmonary veins were evaluated on both axial and reformatted images. CT images showing grade 2 or 3 quality were regarded as diagnostic.
Results
Overall tube current reduction by combined tube current modulation was 15.8±11.1%. The reductions in five body weight groups varied from 9.3±7.9% for the <4.9-kg group (Fig. 2) to 25.8±9.8% for the 20.0–39.9-kg group (Fig. 3), and the reduction tended to increase gradually with increasing group weight apart from the 40.0–59.9-kg group (Table 2). The percentage reductions among the five groups were significantly different (P=0.017). The age ranges of the children in the body weight groups were as follows: 1–2 months, <4.9 kg; 4 months to 1 year, 5.0–9.9 kg; 5 months to 2 years, 10.0–19.9 kg; 2–9 years, 20.0–39.9 kg; 7–16 years, 40.0–59.9 kg. The male:female ratios in the groups were as follows: 8:3, <4.9 kg; 9:6, 5.0–9.9 kg; 3:4, 10.0–19.9 kg; 6:3, 20.0–39.9 kg; 3:5, 40.0–59.9 kg. When all 50 children in the five groups were included, the correlation between age and tube current reduction was not statistically significant. However, age showed a significant positive correlation with tube current reduction (γ=0.4, P=0.003) when eight children in the 40.0–59.9-kg group were excluded (Fig. 4). Tube current reduction was significantly greater for caudocranial scan (21.2±9.2%; Fig. 5) than for the craniocaudal scan (14.2±11.3%; P=0.049). There was no significant difference in the reduction between boys and girls. There was no significant difference in age between the two scan direction groups (31±46 months among 36 children with craniocaudal scan: 48±47 months among 13 children with caudocranial scan; P>0.05). All CT angiography images, including both axial and reformatted images, showed diagnostic image quality (visual grade 2 in 26 studies, visual grade 3 in 24 studies), which meant that image noise was acceptable for the delineation of major extracardiac vessels including the aorta, pulmonary arteries and pulmonary veins in all studies.



A 1-month-old boy (body weight <4.9 kg) who underwent truncus separation and a valveless right ventricle-pulmonary artery conduit for truncus arteriosus type 1. Contrast agent was administered through a leg vein and CT was performed in the craniocaudal direction. a Axial CT image at the level of the major bronchi (the 12th of 37 slices) is of diagnostic quality (grade 2). The round thoracic geometry may partly reduce the effect of combine tube current modulation. b Graph illustrates tube current reduction by combined tube current modulation in relation to slice position. An increase in tube current noted between the 6th and 18th slices is due to inclusion of the arms; these slice positions correspond with the position of the arms on the scout image (c). The inclusion of the arms in the scan range is thought to be the main cause of the lower dose-saving effect of combined tube current modulation in this examination


A 7-year-old boy (body weight 20.0–39.9 kg) with supravalvar aortic and pulmonary stenoses associated with Williams syndrome. Contrast agent was injected through the leg vein and CT was performed in the craniocaudal direction. a Axial CT image at the level of the major bronchi (the 20th of 55 slices) is of diagnostic quality (grade 3). Compared with the case illustrated in Fig. 2, exclusion of the arms from the scan range and a large proportion of the lung in an ovoid thorax may contribute to greater tube current reduction by combined tube current modulation. b Graph illustrates tube current reduction by combined tube current modulation related to slice position. In contrast to the case illustrated in Fig. 1, a marked reduction in tube current is identified in the region of the lung

Graph illustrating the correlation between age and tube current reduction by combined tube current modulation. Age shows a significant positive correlation with tube current reduction (γ=0.4, P=0.003) when eight children in the 40.0–59.9-kg group are excluded. A relatively wide range of tube current reductions in children with similar ages on the graph may be due to wide variations in thoracic geometry and attenuation


A 7-year-old boy (body weight 20.0–39.9 kg) with pulmonary atresia, ventricular septal defect and major aortopulmonary collateral arteries who underwent a right ventricle-pulmonary artery conduit. Contrast agent was administered through the arm vein and CT was performed in the caudocranial direction. a Axial CT image at the level of the major bronchi is of diagnostic quality (grade 2). The cross section of the thorax looks ovoid and the lung occupies a large proportion of the thoracic cross section. b Graph illustrates tube current reduction by combined tube current modulation related to slice position. A 32.9% reduction was achieved by combined tube current modulation. The pattern of the curve is very similar to the case illustrated in Fig. 3 which was the result of scanning in the opposite craniocaudal direction. The caudocranial scan was found to provide greater tube current reduction by combined modulation than did a craniocaudal scan
Discussion
Tube current modulation has been reported to be useful in achieving a significant reduction in CT radiation dose with preservation of diagnostic image quality [15–23]. As far as we are aware, there has been only one previous study dealing with combined tube current modulation; it demonstrated that combined modulation using both angular and z-axis modulation provided greater dose reduction and better correlation between the mean effective tube current level and body mass index of patients than did angular modulation [15]. In a few studies tube current modulation has been used in children [16, 17]. Low tube voltage, less than 100 kVp, has not, to our knowledge, been evaluated with tube current modulation and combined tube current modulation has also not been evaluated in children. We found that combined tube current modulation was able to reduce tube current of non-ECG-gated heart CT when performed with a weight-based low-dose protocol using 80 kVp in children, by an average of 15.8%.
Although combined modulation provides a good anatomy-adapted automatic exposure control, a body size-adaptive reference mAs table is still required to maintain desired image noise regardless of body geometry, particularly in children. These individually adapted protocols using a combination of weight-adapted effective mAs and tube current modulation have been shown to provide a well-balanced 16-slice spiral chest CT examination [17]. We also used a combination of our own weight-based protocol and combined tube current modulation. In order to be free from a body size-adaptive reference mAs table, further technical developments are needed. Recently, a new body size parameter, the so-called topogram-based estimate, has been found to be more suitable for individual dose adaptation than other body size parameters [24], but the parameter has not been used in combination with tube current modulation.
In our study, a tendency for greater tube current reduction by combined tube current modulation was found in older children except for the 40.0–59.9-kg group. This tendency may be explained by differences in thoracic geometry and attenuation profile among the groups. In other words, younger children have a more rounded thoracic geometry, smaller proportions of the lung, and greater likelihood of inclusion of the arms, all of which contribute to the lower dose-saving effect of tube current modulation observed in younger children. A round thoracic geometry unequivocally lessens dose reduction by angular modulation. A smaller proportion of the lung having very low attenuation might diminish tube current reduction by z-axis modulation. Slice positions showing increased tube current in young children actually matched well with the position of the arms included in the CT scan (Fig. 1). This inclusion of the arms might change the local attenuation profile and, subsequently, might limit the reduction by tube current modulation. Based on this finding, every effort to exclude the arms from the CT scan range should be made in young children. High attenuation structures, such as metallic endoprostheses, were found to increase tube current associated with tube current modulation [25]. Though a technique avoiding the increase in CT radiation dose associated with metallic prosthesis was implemented in the combined tube current modulation (CARE Dose 4D) used in our study [26], high attenuation regions not reaching a threshold, such as the arms, may still increase tube current.
Older children heavier than 40 kg demonstrated a paradoxical drop in tube current reduction using combined tube current modulation. The exact reason for this remains unclear, but the use of 80 kVp may relate to the lower dose-saving effect of tube current modulation in older children. An explanation could be that the penetrating strength of 80 kVp might be insufficient to generate tube current modulation function data in the heaviest group. This assumption was proven by our phantom study in which 80 kVp demonstrated a smaller dose-saving effect obtained by tube current modulation than higher voltage settings in two large phantoms (an adult-size torso anthropomorphic phantom and a cone-shaped acrylic phantom, 36 to 85 cm in diameter and bottles of dilute barium on both sides) having some high-attenuation regions (unpublished data). As far as we know, this finding has not been described in the literature and should be taken into account in planning a CT protocol with tube current modulation. Therefore, a higher tube voltage (such as 100 kVp) may result in tube current modulation having a larger dose-saving effect in older children. Accordingly, we modified our CT angiography protocol and now use 100 kVp instead of 80 kVp in children heavier than 40 kg. In contrast to tube voltage preset, the dose reduction obtained with tube current modulation is independent of the effective tube current preset [15].
As described above, three options (weak, average, or strong) were available for strength of combined tube current modulation in our study. This option was originally described for adult patients and further optimization of tube current modulation may be achieved by choosing an appropriate strength of modulation according to body size, ‘strong’, ‘average’, or ‘weak’. The same principle can be applied to children who have wider variations in body size. In this study, we used ‘average’ strength modulation in all children. We believe that application of ‘weak’ mode to young children may achieve a greater reduction of tube current by tube current modulation possible with the same imaging parameters. A further study is necessary to assess this.
In our study, tube current reduction by tube current modulation was significantly greater in the caudocranial direction than in the craniocaudal direction. The differences in reduction according to scan direction may be caused by differences in attenuation of the introducing body part where tube current modulation starts, which is the upper abdomen for the caudocranial scan and the shoulder in the craniocaudal scan. The upper abdomen is a less-attenuating body part than the shoulder. Therefore, when the scan begins with the less-attenuating body part (the upper abdomen in the caudocranial scan), tube current will be kept constantly lower than that obtained with the opposite scan direction through tube current modulation. Significantly greater reduction of tube current by combined modulation in the caudocranial scan, which has not been described in the literature, was confirmed by our phantom study (unpublished data). Based on this finding, we recommend caudocranial scanning whenever a CT examination includes the thorax and is performed with combined tube current modulation.
There are several limitations of this study. Accurate body weight of the child at the time of CT examination was not available because of the retrospective nature of the study. Nonetheless, we were able to determine that tube current reductions by tube current modulation were significantly different among five body-weight groups although the numbers in each body-weight group were relatively small. Instead of body weight, the age of a child was significantly correlated with tube current reduction by tube current modulation. A major limitation of this study was that our results cannot be applied to different CT systems, different types of tube current modulation, different CT protocols, and different patient profiles. However, other pediatric radiologists can test our results with their own equipment and protocols, and this may eventually lead to improvement in strategies for CT dose reduction based on our results. Our observations come from clinical studies and, therefore, multiple confounding factors potentially affecting our results might have been present. However, a phantom study (unpublished data) subsequently performed after this study did validate our results. Finally, quantitative evaluation of the quality of CT images would be better than the qualitative approach we used.
In conclusion, combined tube current modulation reduced tube current in pediatric non-ECG-gated heart CT by 15.8%, without degradation of image quality. This is less than the percentage reduction previously reported by other investigators, partly due to our low-dose CT protocol using 80 kVp and partly due to inclusion of the arms in young children. To obtain greater tube current reduction by combined tube current modulation, we recommend exclusion of the arms from the scan range in younger children, the use of a higher tube voltage in older children, and the use of caudocranial scanning in all children. We hope that our results contribute to further technical optimization of combined tube current modulation in pediatric CT.
References
Linton OW, Mettler FA Jr (2003) National conference on dose reduction in CT with an emphasis on pediatric patients. AJR 181:321–329
Brenner DJ, Elliston C, Hall E, et al (2001) Estimated risks of radiation-induced fatal cancer from pediatric CT. AJR 176:289–296
Goo HW (2005) Pediatric CT: understanding of radiation dose and optimization of imaging techniques. J Korean Radiol Soc 52:1–5
Kalra MK, Maher MM, Toth TL, et al (2004) Strategies for CT radiation dose optimization. Radiology 230:619–628
Boone JM, Geraghty EM, Seibert JA, et al (2003) Dose reduction in pediatric CT: a rational approach. Radiology 228:352–360
Frush DP, Soden B, Frush KS, et al (2002) Improved pediatric multi-detector body CT using a size-based color-coded format. AJR 178:721–726
Starck G, Lonn L, Cederblad A, et al (2002) A method to obtain the same level of CT image noise for patients of various sizes, to minimize radiation dose. Br J Radiol 75:140–150
Sigal-Cinqualbre AB, Hennequin R, Abada HT, et al (2004) Low-kilovoltage multi-detector row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology 231:169–174
Kalra MK, Maher MM, Toth TL, et al (2004) Techniques and applications of automatic tube current modulation for CT. Radiology 233:649–657
Flohr TG, Schaller S, Stierstorfer K, et al (2005) Multi-detector row CT systems and image-reconstruction techniques. Radiology 235:756–773
Goo HW, Park IS, Ko JK, et al (2003) CT of congenital heart disease: normal anatomy and typical pathologic conditions. Radiographics 23:S147–S165
Goo HW (2004) Evaluation of the airways in patients with congenital heart disease using multislice CT. J Korean Pediatr Cardiol Soc 8:37–43
Goo HW, Park IS, Ko JK, et al (2005) Computed tomography for the diagnosis of congenital heart disease in pediatric and adult patients. Int J Cardiovasc Imaging 21:347–365
Goo HW, Park IS, Ko JK, et al (2005) Visibility of the origin and proximal course of coronary arteries on non-ECG-gated heart CT in patients with congenital heart disease. Pediatr Radiol 35:792–798
Mulkens TH, Bellinck P, Baeyaert M, et al (2005) Use of an automatic exposure control mechanism for dose optimization in multi-detector CT examinations: clinical evaluation. Radiology 237:213–223
Greess H, Lutze J, Nomayr A, et al (2004) Dose reduction in subsecond multislice spiral CT examination of children by online tube current modulation. Eur Radiol 14:995–999
Greess H, Wolf H, Baum U, et al (2000) Dose reduction in computed tomography by attenuation-based on-line modulation of tube current: evaluation of six anatomical regions. Eur Radiol 10:391–394
Das M, Mahnken AH, Mühlenbruch G, et al (2005) Individually adapted examination protocols for reduction of radiation exposure for 16-MDCT chest examinations. AJR 184:1437–1443
Kalra MK, Rizzo S, Maher MM, et al (2005) Chest CT performed with z-axis modulation: scanning protocol and radiation dose. Radiology 237:303–308
Tack D, De Maertelaer V, Gevenois PA (2003) Dose reduction in multidetector CT using attenuation-based online tube current modulation. AJR 181:331–334
Mastora I, Remy-Jardin M, Delannoy V, et al (2004) Multi-detector row spiral CT angiography of the thoracic outlet: dose reduction with anatomically adapted online tube current modulation and preset dose savings. Radiology 230:116–124
Greess H, Nomayr A, Wolf H, et al (2002) Dose reduction in CT examination of children by an attenuation-based on-line modulation of tube current (CARE Dose). Eur Radiol 12:1571–1576
Rizzo SM, Kalra MK, Schmidt B (2005) Automatic exposure control techniques for individual dose adaptation (letter). Radiology 235:335–336
Menke J (2005) Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology 236:565–571
Rizzo SM, Kalra MK, Maher MM, et al (2005) Do metallic endoprostheses increase radiation dose associated with automatic tube-current modulation in abdominal-pelvic MDCT? A phantom and patient study. AJR 184:491–496
Dalal T, Kalra MK, Rizzo SM, et al (2005) Metallic prosthesis: technique to avoid increase in CT radiation dose with automatic tube current modulation in a phantom and patients. Radiology 236:671–675
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00247-006-0186-2
Rights and permissions
About this article
Cite this article
Goo, H.W., Suh, D.S. Tube current reduction in pediatric non-ECG-gated heart CT by combined tube current modulation. Pediatr Radiol 36, 344–351 (2006). https://doi.org/10.1007/s00247-005-0105-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-005-0105-y