
Abstract
The potential of online tube current modulation in subsecond multislice spiral CT (MSCT) examinations of children to reduce the dose without a loss in image quality is investigated in a controlled patient study. The dose can be reduced for oval patient sectional view without an increase in noise if the tube current is reduced where the patient diameter and, consequently, attenuation are small. We investigated a product version of an online control for tube current in a SOMATOM Sensation 4 (Siemens, Forchheim). We evaluated image quality, noise and dose reduction for examinations with online tube current modulation in 30 MSCT of thorax/abdomen and abdomen and compared mA s for tube current modulation to the mA s in standard weight-adapted children protocols. Image quality was rated as “very good,” “good,” “diagnostic” and “poor” in a consensus by three radiologists. Noise was assessed in comparison to 24 MSCT examinations without tube current modulation measured as SD in ROIs. The dose was reduced from 26 to 43% (mean 36%), depending on the patient’s geometry and weight. In general, no loss of image quality was observed. Measured noise showed a decrease up to 26% and an increase up to 36%, although there was no decrease of image quality. Online tube current modulation is now used as a standard in MSCT at our institution. Dose in MSCT examinations of children can be reduced substantially in routine examinations by online tube current modulation without a loss of image quality.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
A major disadvantage with the increased use of multislice spiral CT (MSCT) is the associated radiation exposure. Radiation exposure is particularly important for children because of the relatively increased lifetime cancer risk compared with that of adults [1] and because of the higher radiosensitivity of children compared to that of adults [2]. One technical possibility to reduce the dose was using a software-based modulation of the tube current (SmartScan, General Electric Systems, Milwaukee, WI). The local absorption was measured in the 100 central channels of two localizer radiographs (lateral and anterior-posterior) and used for sinusoidal modulation of the tube current [3–5].
Another possibility to reduce the dose in CT is an online modulation of the tube current. This approach was performed on a single slice spiral CT scanner in a phantom and cadaver study [6] and first patient studies [7, 8]. A substantial dose reduction with equal or improved image quality is possible, the noise contribution is more homogenous and there were fewer noise artifacts with tube current modulation [7].
The present study aimed to investigate the possible extent of exposure reduction for children in two scan regions on a subsecond multislice CT (MSCT) with tube current modulation in comparison to examinations without tube current modulation and in comparison to examinations of children with tube current modulation on a single-slice CT scanner [9].
Materials and methods
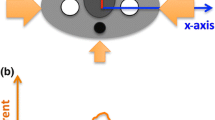
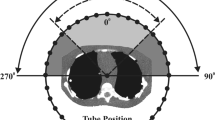
For a body with oval sectional view, attenuation is almost constant for all projections, and all measured values contribute equally. For a body with non-circular cross section, and this is normal, attenuation varies extremely, sometimes by more than three orders of magnitude [10]. Noise in the volume MSCT data measured in high attenuation projections, mostly in lateral directions, is important for the noise level in the MSCT image. This means that the tube current for projections with relatively low attenuation, mostly in the anterior-posterior direction, can be reduced substantially without a measurable increase of image noise. The deduction, and the basic consideration of the tube current modulation, is that tube current should be decreased as a function of rotation angle whenever attenuation is low. Therefore, we had to develop means for monitoring attenuation online and for variation of the tube current as a function of projection angle with a delay of 360°. Thereby, modulation can be effected after the first 360° of scanning and is updated continuously in real time. No changes were made with respect to image reconstruction. The maximal reduction of the tube current was 90% for projections with low attenuation [10, 11].
The respective technical solution (tube current modulation, CARE Dose) is the product on an MSCT SOMATOM Sensation 4 (Siemens, Forchheim, Germany). We performed 30 MSCT examinations with tube current modulation on a consecutive number of children without selection. The age ranged from 11 months up to 18 years. Two different scan regions were examined: thorax/abdomen and abdomen. The scan parameters were slice 4 times 2.5 mm, pitch 1.5, rotation time 0.5 s, 120 kVp and reconstruction increment 2.5 mm. We compared the results of mA s values read from the CT scanner with present mA s of a standard protocol adapted to the individual weight of the children. In this group we correlated the weight of the children with the measured mA s reduction. We also performed 24 MSCT examinations without tube current modulation on a consecutive number of children without selection. The age ranged from 10 months up to 13 years. We examined the two scan regions with the same parameters. The tube current in the control group was adapted to the weight of the children and for this purpose we divided the children into seven groups (see Table 1). The noise was measured by the average standard deviation (SD) of region of interest (ROI) 1 and 2 for thorax images and by the average SD of ROI 3 and 4 for abdomen scans. ROI 1 was in the trachea at the level of the clavicle, ROI 2 was in the trachea at the level of the tracheal bifurcation (ROI 1 and 2=19 observations with and 13 observations without tube current modulation). ROI 3 was in the aorta at the level of the diaphragm and ROI 4 was in the origin of the superior mesenteric artery from the aorta (ROI 3 and 4=26 observations with and 20 observations without tube current modulation). There were 54 MSCT scans of 54 children in total (30 children with and 24 children without tube current modulation with 78 ROIs in total). We investigated how the quality of the MSCT images with dose reduction compares to the standard images taken without dose reduction. An easily interpreted measure is the relative increase or decrease of noise in SD of images with tube current modulation compared to images without tube current modulation. Therefore, inference about the ratio of the median SD (with) and SD (without) is appropriate. We report non-parametric 95% confidence intervals for the ratio of medians derived from the Wilcoxon rank sum test. The exact conditional distribution was used because some of the observations were tied. All computations were performed in the R system for statistical computing (http://www.r-project.org), version 1.5.1 [12].
Image quality was evaluated in consensus by visual interpretation of three experienced radiologists as very good, good, diagnostic and poor for 30 examinations with and 24 examinations without tube current modulation.
Results
mA s reduction
The average mA s reduction of all scan regions was 36% (maximal 43%, minimal 26%) compared to a standard protocol, which was weight adapted (Fig 1). In thorax/abdomen examinations the effective mA s varied from 40 up to 106. The mean dose reduction in percentage varied in this group from 31.3 up to 39. In the abdomen examinations, the effective mA s varied from 40 to 100, the according mean dose reduction was 32.3 up to 39.9% (Table 2).

Average mA s reduction for thorax/abdomen and abdomen examinations
Correlation between weight and dose reduction with tube current modulation
There is no correlation between weight and dose reduction detected in the specific categories, as can be seen in Table 2.
Assessment of image quality
With regards to the visual image quality, image noise and contrast resolution, the evaluation of image quality resulted in n=1 as diagnostic, n=14 as good and in n=15 as very good. A poor image quality was not detected in any case.
Even in areas with high attenuation, such as the shoulder or pelvis, a good image quality was found. In Fig 2, a comparison of images with and without tube current modulation is shown. Both were evaluated as very good image quality, but in the scan on the right with tube current modulation, there is a mA s reduction of 40%.

Comparison of images with (right) and without tube current modulation (left) both evaluated as very good image quality. The mA s reduction in the right images was 40%
Comparable results were found in the group without tube current modulation. Image quality was detected as diagnostic in n=2, as good in n=13 and as very good in n=9. Poor image quality was not found.
Statistical analysis for the noise
For MSCT scans of the thorax (ROI 1 and 2), the images with tube current modulation had an average SD between 74 and 136% of the images without tube current modulation. For MSCT scans of the abdomen (ROI 3 and 4), the images with tube current modulation had an average SD between 105 and 132% of the images without tube current modulation, which corresponds to an average SD increase between 5 and 32% when tube current modulation was applied.
That means, objectively, that the SD in the group with tube current modulation in the abdomen region is up to 32% higher than the SD of images without dose reduction. The SD in the group with tube current modulation in the thorax region is up to 26% lower and up to 36% higher than the SD of images without dose reduction (big variation).
Discussion
The results of this study of children show that a substantial reduction of the mA s can be achieved in both scan regions using tube current modulation. The differences in both scan regions in respect to the possibility to reduce dose was not considerable. Brix et al. considered the increase of the average dose per CT examinations for quad-slice systems with respect to single slice CT not so alarming as it might have appeared from other studies. So their results reveal that the mean effective dose to patients has been changed from 7.4 mSv at single slice CT scanners to 8.1 mSv at quad-slice systems [13]. Also, Cohnen et al. saw a comparable radiation exposure between single slice CT and MSCT. The single slice CT examinations lead to effective doses of approximately 5–20 mSv, radiation exposure in standard MSCT protocols of the neck, chest, abdomen and lumbar spine ranges from 3–15 mSv [14]. In a former study of children for single slice CT the average mA s reduction was 23% in the thorax and the abdomen scan regions and 22% in the combined scan region of thorax and abdomen [9]. Therefore, we see a comparable, respectively, higher mA s reduction for this approach in MSCT for children. The highest dose reduction was found in examinations of the thorax/abdomen and the abdomen region in the lowest weight group (9–17.9 kg), with 41.4 and 43%, respectively. This showed that a substantial dose reduction was achieved only in very young and thin children . The large spread of mA s reduction in the present study (minimal 26.3%, maximal 43%) results on the one hand from extremely thin children with a big difference in lateral and a.p. cross-section and high mA s reduction and on the other hand from obese children with almost no difference in cross-section and low mA s reduction. For an alternative approach using a sinusoidal tube current modulation based on scout views (SmartScan, General Electric Systems, Milwaukee, WI), there are no data available for dose reduction in children.
Using attenuation-based online modulation of tube current, we achieve substantially higher dose reduction in the thorax and the abdomen scan regions comparing our own results for children with the results in the same scan regions for adults with SmartScan [3, 5]. The quality deficiencies of three examinations of children (two without and one with tube current modulation) evaluated only as diagnostic were due to motion artifacts in very young children. Also other authors observed only “good” image quality by tachypneic infants [15]. But the image quality with tube current modulation was estimated subjectively in 90% as good or very good. Donnelly and co-authors advise to adapt tube current to the patient’s weight. The biggest disadvantage they have seen is the increase of noise linked with a decrease of image quality [16].
In a recent publication concerning MSCT dose exposure in children, Vock recommends not to achieve the perfect but rather the image quality needed to get all the necessary information with the least possible dose. He proposes to get used to more noisy, but still diagnostic images in the future [17]. But in the end, everyone has to decide the level of acceptable noise on his own. With tube current modulation, we see a decrease in measured noise up to 26% and an increase up to 36%, but we see no effect on the subjectively evaluated image quality. This means that a dose reduction of approximately 36% is possible, and we still get CT images rated good or very good , although there is a measured increase in noise. We conclude that the use of tube current modulation allows a substantial mA s reduction in both investigated scan regions without a decrease in image quality. This technique is efficient and practical for minimizing dose exposure in MSCT of children.
References
Rogers LF (2001) Taking care of children. Check out the parameters used for helical CT. Am J Roentgenol 176:287
Ware D, Huda W, Mergo P, Litwiller A (1999) Radiation effective doses to patients undergoing abdominal CT examinations. Radiology 210:645–650
Giacomuzzi SM, Erckert B, Freund MC, Schöpf T, Dessl A, Jaschke W (1996) Dosisreduktion in der Computertomographie mit einem neuen Scan Verfahren. Akt Radiol 6:110–113
Kopka L, Funke M, Breitner N, Hermann K-P, Vosshenrich R, Grabbe E (1995) Anatomisch adaptierte Variation des Röhrenstroms bei der CT. Untersuchungen zur Strahlendosisreduktion und Bildqualität. Fortschr Röntgenstr 163:383–387
Lehmann KJ, Wild J, Georgi M (1997) Klinischer Einsatz der Software gesteuerten Röhrenstrommodulation „SmartScan“ in der Spiral-CT. Akt Radiol 7:156–158
Kalender WA, Wolf H, Suess C, Gies M, Greess H, Bautz WA (1999) Dose reduction in CT by on-line tube current control: principles and validation on phantom and cadavers. Eur Radiol 9:323–328
Greess H, Wolf H, Kalender WA, Bautz W (1998) Dose reduction in CT anatomically adapted tube current modulation: first patient studies. In: Glazer G, Krestin G (eds) Advances in CT IV. Springer, Berlin Heidelberg New York, pp 35–40
Greess H, Wolf H, Baum U, Lell M, Pirkl M, Kalender WA, Bautz W (2000) Dose reduction in computed tomography by attenuation based on on-line modulation of the tube current: evaluation of six anatomical regions. Eur Radiol 10:391–394
Greess H, Nömayr A, Wolf H, Baum U, Lell M, Böwing B, Kalender WA, Bautz WA (2002) Dose reduction in CT examination of children by attenuation-based on-line modulation of tube current (CARE Dose). Eur Radiol 12:1571–1576
Kalender WA, Wolf H, Suess C, Gies M, Greess H, Bautz W (1998) Dose reduction in CT by anatomically adapted tube current modulation: principles and first results. In: Glazer G, Krestin G (eds) Advances in CT IV. Springer, Berlin Heidelberg New York, pp 27–34
Kalender WA, Wolf H, Suess Ch (1999) Dose reduction in CT by anatomically adapted tube current modulation. II. Phantom measurements. Med Phys 26:2248–2253
Ihaka R, Gentlemen R (1996) R: a language for data analysis and graphics. J Comput and Graph Stat 5:299–314
Brix G, Nagel HD, Stamm G, Veit R, Lechel U, Griebel J, Galanski M (2003) Radiation exposure in multi-slice versus single-slice spiral CT: results of a nationwide survey. Eur Radiol 13:1979–1991
Cohnen M, Poll LW, Puettmann C, Ewen K, Saleh A, Mödder U (2003) Effective doses in standard protocols for multi-slice CT scanning. Eur Radiol 13:1148–1153
Ambrosino MM, Genieser NB, Roche KJ, Kaul A, Lawrence RM (1994) Feasibility of high-resolution, low-dose chest CT in evaluating the paediatric chest. Pediatr Radiol 24:6–10
Donnelly LF, Emery KH, Brody AS, Laor T, Gylys-Morin VM, Anton CG, Thomas SR, Frush DP (2001) Minimizing radiation dose for paediatric body: applications of single-detector helical CT. Strategies at a large children’s hospital. Am J Roentgenol 176:303–306
Vock P (2002) CT Exposition beim Kind: Geht das Erwachen der Amerikaner uns Europäer an? Radiologe 42:679–702
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Greess, H., Lutze, J., Nömayr, A. et al. Dose reduction in subsecond multislice spiral CT examination of children by online tube current modulation. Eur Radiol 14, 995–999 (2004). https://doi.org/10.1007/s00330-004-2301-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-004-2301-9