
Abstract
Baffle fenestration is associated with a significantly better outcome in standard and high-risk patients undergoing completion of Fontan. We report the effects of subsequent transcatheter closure of fenestration on exercise capacity and oxygen saturation. Sixteen patients with a mean age of 10.3 years underwent Amplatzer septal occluder (ASO) device transcatheter closure of Fontan fenestration. All had a fenestrated Fontan operation 6 month to 8 years prior to the procedure. A stress test was performed before and after device closure of fenestration in 14 patients (2 patients did not tolerate stress test before the procedure). The fenestrations in all patients were successfully occluded with the use of the Amplatzer device occluder. No complications occurred during or after the procedure. O2 saturation increased from a mean 85.1 ± 7.89% to 94.5 ± 3.63% (p < 0.01) at rest and from 66.2 ± 12.86% to 87.2 ± 8.64% (p < 0.01) following exercise. Exercise duration has also increased from 8.22 ± 2.74 min to 10.29 ± 1.91 min (p < 0.05). Transcatheter closure of Fontan fenestration increases the duration of exercise capacity and increases O2 saturation at rest and after exercise.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Three- to-six-millimeter fenestration of the Fontan is associated with better early survival and less perioperative complications after a Fontan operation [1, 2, 6]. This is attributed to the reduction of systemic venous pressure and to the augmentation of the systemic ventricular preload in the presence of high pulmonary artery pressure [1, 6, 8]. However, these short-term benefits come at the expense of systemic oxygen saturation and the potential hazards of right-to-left shunt such as endocarditis and paradoxical embolism, in the long term. Delayed postoperative transcatheter closure of Fontan fenestration is considered an option to prevent such long-term sequelae [4, 9]. The effects of such a procedure on exercise duration and oxygen saturation at rest and following exercise are reported here.
Materials and Methods
Patient Population
The study was approved by the Internal Review Board at the Prince Sultan Cardiac Centre. The mean age was 10.3 years (6–13 years) and a mean weight of 34.1 kg (15.6–61.7 kg). All participated in the study 6 months to 8 years from the date of operation. The pre-operative diagnosis is summarized in Table 1. Patients had bidirectional Glenn shunts constructed 2–8 years before the completion of Fontan. The Fontan operation consisted of using direct bicaval cannulation and aortic return, keeping the heart perfused and beating while allowing mild systemic hypothermia. All existing aortopulmonary shunts were closed and the main pulmonary artery (MPA) was transected. The pulmonary artery confluence was enlarged with a bovine pericardial patch that extended well into the undersurface of the right pulmonary artery (RPA). An 18–22-mm polytetrafluoroethylene (PTFE) (Gortex®) tube conduit of appropriate length is chosen depending on the patient’s weight. One end was anastomosed end-to-side to the undersurface of the enlarged RPA onto the bovine pericardial patch used for its enlargement. The other end of the conduit was anastomosed end-to-end to the transected end of the inferior vena cava (IVC). A 3–6-mm fenestration was created between the side of the conduit and the lateral wall of the right atrium (RA) by direct side-to-side anastomosis at the end of the procedure.
Patients underwent stress test using the modified Bruce protocol before and after the catheter procedure. The modified Bruce protocol was used while monitoring the ECG, blood pressure (BP), a pulse oximeter, and the duration of exercise.
Cardiac Catheterization
Cardiac catheterization was performed under general anesthesia, with transesopheageal echocardiography guidance, in eight patients, and under local anesthesia, utilizing intracardiac ultrasound (ICE), in the last eight patients. After complete hemodynamic assessment as previously described [9], balloon test occlusion was accomplished in 5 patients using a BALT 7 Momenah sizing balloon (Extursion Febrication de Catheters, Montmorency, France). During the procedure, saturation and cardiac output were monitored for a period of 15 min to ensure adequacy of systemic pressure and cardiac output; the balloon was then deflated. Subsequently, an angiography in the Fontan connection was performed to identify the anatomy and to measure the size of the fenestration. Transcatheter closure was performed using the Amplatzer ASO device (AGA Medical, Golden Valley, MN) as previously described [2]. In the last 11 patients, test occlusion was done with the Amplatzer device itself.
Twenty-four hours after the procedure, all patients underwent chest radiograph, ECG, and two-dimensional (2D) echocardiography study to assure the position of the device and rule out a significant residual shunt. The patients were discharged with a follow-up appointment at 6 weeks time for evaluation, including a stress test with saturation monitoring. All patients were on an adjustable dose of warfarin to maintain the international normalizing ratio (INR) between 1.8 and 2.5.
Statistical Analysis
Data are expressed as the mean value ± SD. Comparisons of results before and after closure of the fenestration were performed using the paired Student’s t-test. Statistical significance was defined as p < 0.05.
Results
All patients underwent successful occlusion of the fenestration with the use of the Amplatzer ASO device for closure of an atrial septal defect. There was no device embolization or other complications during hospital admission. Six to 12 weeks later, transthoracic 2D echocardiography and color-Doppler revealed complete occlusion of the fenestration. The pulmonary artery pressure measured before fenestration closure was a mean of 11.68 ± 3.47 and the postfenestration closure mean was 13.93 ± 2.46.
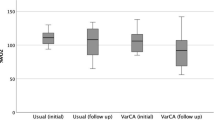
The mean oxygen saturation at rest increased from 85.12 ± 7.89% before closure of the fenestration to 94.56 ± 3.63% after the procedure (p < 0.01) (Fig. 1). The mean oxygen saturation following exercise increased from 66.21 ± 12.86% before to 87.21 ± 8.64% after the procedure (p = < 0.01) (Fig. 2). The duration of mean exercise also increased from 8.22 ± 2.74 min before to 10.29 ± 1.91 min following the procedure (p = 0.05) (Fig. 3).

Effect of fenestration closure on oxygen saturation at rest

Effect of fenestration closure on oxygen saturation at peak of exercise

Effect of fenestration closure on exercise tolerance
Discussion
The introduction of a fenestration to the Fontan circuit allows a right-to-left shunt as a vent maintaining cardiac output [1, 6, 8]. This effect is achieved at the cost of decreasing systemic oxygen saturation [4, 9]. This procedure can be useful, especially in the early postoperative phase when there is a relative increase in pulmonary vascular resistance [1, 8]. Beyond the acute postoperative stage, the presence of fenestration might not be desirable [3, 5, 7]. Others have reported successful percutaneous closure of a Fontan fenestration in a number of cases without detailed analysis of the effects of closure of the fenestration on exercise tolerance and oxygen saturation before and after exercise [4, 9]. In this study, we found that closure of a fenestration in a patient with a fenestrated Fontan beyond 6 months does not only improve oxygen saturation but also enhances exercise performance. The timing of intervention is not well defined; we have elected to wait for 6 months postoperatively, as for the majority of these patients the fenestrations can close spontaneously within the first 1 year after surgery [10]. Studies of acute hemodynamic changes, oxygen-carrying capacity, and VO2 max could not be done in this study.
In summary, closure of a fenestration using the Amplatzer ASO device can be done with minimal risk. It increases oxygen saturation and improves the ability to exercise by preventing a right-to-left shunt. Long-term follow-up is recommended to evaluate the benefits versus the risks of fenestration closure.
References
Bridges ND, Mayer JE Jr, Lock JE, et al. (1992) Effect of baffle fenestration on outcome of the modified Fontan operation. Circulation 86(6):1762–1769
Fontan F, Baudet E (1971) Surgical repair of tricuspid atresia. Thorax 26:240–248
Giannico S, Hammad F, Amodeo A, et al. (2006) Clinical outcome of 193 extracardiac Fontan patients: the first 15 years. J Am Coll Cardiol 47(10):2065–2073
Hijazi Z MD, Fahey J MD, Kleinman C MD, et al. (1992) Hemodynamic evaluation before and after closure of fenestrated Fontan. An acute study of changes in oxygen delivery. Circulation 86:196–202
Jacobs ML, Pelletier G (2006) Late complications associated with the Fontan circulation. Cardiol Young Suppl 1:80–84
Lemler M, Scott W, Leonard R, et al. (2002) Fenestration improves clinical outcome of the Fontan procedure. A prospective randomized study. Circulation 105:207–212
Ono M, Boethig D, Goerler H, Lange M, et al. (2006) Clinical outcome of patients 20 years after Fontan operation: effect of fenestration on late morbidity. Eur J Cardiothorac Surg 30(6):923–929
Petrossian E, Reddy VM, Collins KK, et al. (2006) The extracardiac conduit Fontan operation using minimal approach extracorporeal circulation: early and midterm outcomes. J Thorac Cardiovasc Surg 132(5):1054–1063
Sommer RJ, Recto M, Golinko RJ, Griepp RB (1996) Transcatheter coil occlusion of surgical fenestration after Fontan operation. Circulation 94(3):249–252
Toefig M, Walsh K P, Chan C, Ladusans E, Gladman G, Arnold R (1998) Occlusion of Fontan fenestration using the Amplatzer septal occluder. Heart 79:368–370
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Momenah, T.S., Eltayb, H., Oakley, R.E. et al. Effects of Transcatheter Closure of Fontan Fenestration on Exercise Tolerance. Pediatr Cardiol 29, 585–588 (2008). https://doi.org/10.1007/s00246-007-9154-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-007-9154-3