
Abstract
We studied the role of duplex Doppler ultrasonography in the diagnosis of renal obstruction caused by ureteral calculi. Using duplex Doppler sonography, we evaluated the intrarenal hemodynamics of 27 patients who presented to the emergency department with renal colic. We performed Doppler ultrasonography on patients in whom US did not reveal any pathology causing renal colic and calculated and compared mean RI values of normal and obstructed kidneys and ΔRI values of each group. Threshold levels for the diagnosis of urinary tract obstruction (mean RI ≥ 0.70 and ΔRI ≥ 0.08) were used to determine the sensitivity and specificity of Doppler sonography for the diagnosis of urinary tract obstruction. Patients were investigated for revealing calculi diagnosis either by stone excretion history, intravenous pyelography or non contrast enhanced urinary computed tomography. A total of 162 intrarenal arterial Doppler recordings were made on 54 kidneys. Of the 16 patients with urinary obstruction, 11 (68%) had sonographic evidence of pelvicalyceal dilatation. The mean RI of the 16 obstructed and 11 unobstructed kidneys was 0.69 ± 0.04 and 0.61 ± 0.06 (mean ± standard deviation), respectively. The difference between the mean RI values for each group was statistically significant (P < 0.05). Mean RI values of the contralateral kidneys in the obstructed group and unobstructed group were 0.61 ± 0.03 and 0.59 ± 0.05, respectively. Also ΔRI value (0.07 ± 0.02) of obstructed kidney group was statistically higher than the ΔRI value (0.01 ± 0.03) of the unobstructed group (P < 0.05). The mean RI of the 16 obstructed kidneys (0.69 ± 0.04) was significantly greater than that of the 16 unobstructed contralateral kidneys (0.61 ± 0.03) (P < 0.05). This study supplements the existing evidence that, in acutely obstructed kidneys, renal Doppler recording can demonstrate altered renal perfusion before pelvicalyceal system dilatation and distinguish obstructed and unobstructed kidneys evaluated with suspicion of renal colic.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Flank pain due to urolithiasis is a common problem in patients presenting to the emergency department. Radiology plays a vital role in the work-up of these patients. Although helical computed tomography (CT) is considered the gold standard for the diagnosis of obstructive uropathy, it is not always available. Ultrasonography (US) is a sensitive method of detecting dilatation of the renal collecting system and therefore has been recommended for investigating renal colic [1]. However, its use in the diagnosis of acute renal obstruction is limited when dilatation has not developed. Also US lacks the ability to provide significant physiologic data on renal status and sometimes can not distinguish obstructive and nonobstructive dilatation of the kidney [2–4]. With the advent of Doppler US new insight into the physiology of the kidney has emerged, enabling the detection of subtle renal blood flow changes associated with various pathophysiological conditions. Recent work has documented significant elevation in the intrarenal resistive index (RI) in established renal obstruction [1].
This prospective study focuses on the value of duplex Doppler US for the diagnosis of renal obstruction caused by ureteral calculi.
Materials and methods
Between February 2004 and May 2004 we evaluated the intrarenal hemodynamics of 27 patients who presented to the emergency department with renal colic using duplex Doppler sonography. Patient age ranged from 17 to 68 years (mean 41). Thirteen of patients had hematuria. Among the 27 patients, 13 (48%) with varied degrees of hydronephrosis and 14 (52%) without evident obstruction were evaluated. After presenting to the emergency department, routine longitudinal and transverse images of both kidneys were obtained for assesment of pelvicalyceal dilatation, the presence of calculi or other morphological abnormality. When the central echo complex was separated minimally by distended anechoic calyceal structures, the kidneys were classified as dilated; otherwise they were categorized as nondilated. We performed Doppler US on patients in whom gray scale US did not reveal any pathology causing renal colic. Oral informed consent was obtained from each person. Doppler US was performed with a Powervision SSA-140A (Toshiba Medical Systems Co, Ltd, Tokyo, Japanese) US machine using 3.75 MHz sector probe and Toshiba SSA-390A Applio machine (Toshiba Medical Systems Co, Ltd, Tokyo, Japan) with a 3.75 MHz sector probe. The intrarenal vessels were then identified using colour flow Doppler, and Doppler signals were obtained from arcuate arteries at the corticomedullary junctions or interlobar arteries along the border of medullary pyramids, or both. The Doppler sample width was set at 2–5 mm. The individual arteries were sampled while the patient held his or her breath. Recordings were obtained from at least three separate vessels in each kidney. To maximize the size of the Doppler spectrum and decrease the percentage error in the measurements, we selected a low frequency range setting (low pulse repetition frequency) and low wall filter (50 Hz). Doppler spectrum was considered optimal when 3–5 similar appearing consecutive waveforms were obtained. All RI measurements were done after 6 h from the renal colic onset. The renal RI was calculated using the following formula: RI = (peak systolic velocity–end diastolic velocity)/peak systolic velocity. The RI difference (ΔRI) was determined as follows: ΔRI = RI of ipsilateral kidney–RI of contralateral kidney. The values of RI and ΔRI used for statistical analysis were averages of the mean measurements in the individual patients. We compared mean RI values of normal and obstructed kidneys and ΔRI values of each group. Results were calculated using the Statistical Package for the Social Sciences, version 10.0 (SPSS; Chicago) Statistical analysis of difference between RI and ΔRI values of patients with obstructed and unobstructed kidneys was made with Mann–Whitney U test and Chi-square test. Statistically, P values less than 0.05 were considered significant. Previously published discriminatory threshold levels for the diagnosis of urinary tract obstruction (mean RI ≥ 0.70 and ΔRI ≥ 0.08) were used to determine the sensitivity and specificity of Doppler sonography for the diagnosis of urinary tract obstruction [5]. Patients were investigated for revealing calculi diagnosis by either the stone excretion history, intravenous pyelography (IVP) or non contrast enhanced urinary computed tomography (CT).
Results
Between February and May 2004 a total of 162 intrarenal arterial Doppler recordings were made on 54 kidneys. Each examination took 20 min to perform for each kidney, depending on the co-operation of the patient, and no patient had to be excluded because it was not possible to obtain adequate Doppler waveforms. The average duration of symptoms in patients with obstruction was 17 h (range 8–35 h). Sixteen of 27 patients were proved to have urinary obstruction. Of the 16 patients with urinary obstruction, 11 (68%) had sonographic evidence of pelvicalyceal dilatation (Fig. 1). Two patients (18%) of 11 in the unobstructed kidney group had pelvicalyceal dilatation on gray scale US. The mean RI of the 16 obstructed and 11 unobstructed kidneys was 0.69 ± 0.04 and 0.61 ± 0.06 (mean plus or minus standard deviation), respectively. The difference between the mean RI values for each group was statistically significant (P < 0.05). Mean RI values of the contralateral kidneys in the obstructed group and unobstructed group were 0.61 ± 0.03 and 0.59 ± 0.05, respectively. Also the ΔRI value (0.07 ± 0.02) of the obstructed kidney group was statistically higher than the ΔRI value (0.01 ± 0.03) of the unobstructed group (P < 0.05). The mean RI of the 16 obstructed kidneys (0.69 ± 0.04) was significantly greater than that of the 16 unobstructed contralateral kidneys (0.61 ± 0.03) (P < 0.05) (Fig. 2). There was no statistically significant difference between the mean RI of the unobstructed kidneys presented with renal colic (0.61 ± 0.06) and contralateral kidneys in the same group (0.59 ± 0.05). Mean RI of obstructed kidneys (n: 11) accompanying pelvicalyceal dilatation on gray scale US was 0.68 ± 0.05 (Fig. 1). Also mean RI of obstructed kidneys (n: 5) without pelvicalyceal dilatation was 0.71 ± 0.02 (Fig. 2). Mean RI of unobstructed kidneys with pelvicalyceal dilatation (n: 2) was 0.69 ± 0.01 (Fig. 3) and mean RI of unobstructed kidneys without pelvicalyceal dilatation (n: 9) was 0.59 ± 0.08 (Table 1). The difference in the mean RI between obstructed kidneys without pelvicalyceal dilatation and unobstructed kidneys without pelvicalyceal dilatation was statistically significant (P < 0.05).

Pelvicalyceal dilatation is seen on the left kidney (a). The RI measured at the lower pole of the kidney was 0.75 (b)

There is no pelvicalyceal dilatation in the left kidney (a). RI is increased (0.71) measured in the upper pole of the kidney (b) and significantly higher than the RI value of the contralateral kidney (0.60) (c). CT revealed left ureterovesical junction calculi (arrow) caused obstruction

Minimal pelvicalyceal dilatation is seen on gray scale US in the left kidney (a). RI value of this kidney was 0.71, suggesting obstruction (b). No calculus was seen on CT
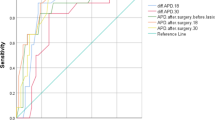
With a resistive index of 0.70 being the critical value to predict the presence of renal obstruction, the sensitivity and specificity of RI were 50 and 90%, respectively. The sensitivity and specificity of ΔRI with the acceptance of cutoff value as 0.08 were 37 and 100%, respectively. Ten patients were proved to have stone with the history of stone excretion, four patients with CT and two patients with IVP. Four patients were proved to be stone negative with repeat investigations and examinations, six patients with CT and one patient with IVP. Radiologic examinations for revealing urinary stone depended on the avaibility of the radiologic examinations and patient’s choice. Figure 4 demonstrates the RI values of obstructed and unobstructed kidneys.

RI values of obstructed and nonobstructed kidneys
Discussion
Traditionally, the evidence of renal obstruction provided by US has been indirect, and dependent on the “anatomical” criterion of dilatation of the pelvicalyceal system and ureter proximal to the level of obstruction. One study showed that US had a sensitivity of only 37% for ureteral calculi (direct visualization); when hydronephrosis was included as a positive sign for ureteral calculi the sensitivity increased to 74% [6]. But early in the course of ureteral obstruction, hydronephrosis may be absent or only of minimal severity in as many as 11–35% of cases [7–10]. So in the absence of pelvicalyceal dilatation functional evaluation of urinary tract gains importance in the diagnosis of evidence of distal urinary tract obstruction. Also US imaging may miss the diagnosis of obstruction in a variety of situations [11]. Mild dilatation may be overlooked or considered clinically insignificant. A minority of patients with obstructive renal failure (up to 5%) may show no pelvicalyceal dilatation [12]. The reasons for this are unclear; in some patients it may relate to dehydration, or to decompression of the pelvicalyceal system by rupture of a calyceal fornix. Intermittent ureteric obstruction, particularly caused by ureteric calculi, may also lead to a failure to visualize the collecting system with US [13]. More direct “functional” evidence of obstruction has usually required scintigraphy, but recently Doppler US techniques have been used to obtain functional information in suspected renal obstruction [13].
The hemodynamic responses of the kidney to ureteral obstruction have been investigated extensively in animal models [14]. Animal studies have demonstrated that a complex series of events follows acute ureteric obstruction. In the first 2 h the renal blood flow increases, because of afferent arteriole vasodilatation, and the ureteric pressure increases. From 2 to 6 h after obstruction, renal blood flow decreases, secondary to vasoconstriction of the efferent arterioles, and ureteric pressure remains elevated. Subsequently, at 6–18 h, renal blood flow remains reduced, because of vasoconstriction of the afferent arterioles, and ureteric pressure decreases [13].
Doppler waveform studies are noninvasive, painless, readily available, and relatively easy to perform and learn. In addition, Doppler US obviates the need for ionizing radiation and intravenous contrast material administration in situations in which they may be undesirable, such as pregnancy, allergy and renal insufficiency [5]. Renal blood flow can be assessed indirectly by Doppler US using the RI. The resistive index is a physiological parameter reflecting the degree of renal vascular resistance. Therefore, it is potentially applicable for detecting kidney disease associated with increased or decreased resistance of the intrarenal vasculature [5]. Normal renal arterial flow has a low resistance pattern with flow maintained throughout diastole. Increased values of RI indicate increased vascular resistance, which is a result of urinary tract obstruction. Experimental studies of ureteric obstruction in dogs have shown that the increase in RI after ureteric obstruction can be detected [3, 15, 16]. Opdenakker et al. [17] found that the RI increase was maximal at 6–48 h after the onset of obstruction. Early Doppler US studies in patients with obstructed kidneys and in normal subjects indicated that the normal RI is <0.7 and that the increase in RI in obstructed kidneys can be used to distinguish dilated obstructed from dilated unobstructed kidneys [2].
Early results using RI for obstruction suggested an excellent sensitivity of 87–100% when an RI of >0.7 was used in patients with suspected ureteric colic [7, 18]. There has been much debate on the role of Doppler US in the diagnosis of acute obstructive uropathy, and the sensitivity and specificity of this method have varied substantially among series. The causes for the discrepancy in the results in the literature concerning the sensitivity of duplex Doppler US in the diagnosis of urinary obstruction are related to these factors: variable discriminatory thresholds used for both RI and ΔRI, nonmeasurement of ΔRI, degree of obstruction, quality of Doppler examination [19]. In our study we used 0.7 as a cutoff value for RI, which refers to obstructed kidneys according to the literature [5, 13, 20]. In the evaluation of renal obstruction, ΔRI may be more important than the RI of the obstructed kidney. In our study we evaluated the ΔRI values of obstructed and unobstructed kidneys and accepted 0.08 as a threshold value refers to obstruction.
Analysis of our results shows similarities to those previously published [1, 2, 7, 17]. The mean RI for unobstructed kidneys (0.61 ± 0.06) was equivalent to that reported from other studies; the difference between the mean RI of obstructed and nonobstructed kidneys was statistically significant. In addition, there was a statistically significant difference between the ΔRI in patients with and without urinary obstruction. The sensitivity and specificity of mean RI was 50 and 90%, respectively. In the literature the sensitivity of RI differs in the range between 30 and 87% with a cutoff value of 0.70. In addition ΔRI had sensitivity and specificity values of 37 and 100%, respectively. The sensitivity and specificity values depend on the cutoff values. So we could have high sensitivity and specificity values by choosing low thresholds as used in some studies. We think that emphasizing the statistical difference with obstructed and unobstructed kidneys is more realistic than sensitivity and specificity values in order to search for the value of RI in urinary obstruction.
We think it was important to show the difference between obstructed kidneys without pelvicalyceal dilatation and unobstructed kidneys without pelvicalyceal dilatation. The mean RIs of the first and second group were 0.71 ± 0.02 and 0.59 ± 0.08, respectively, and the difference of these values was statistically significant. In the absence of pelvicalyceal and ureteral dilatation, it is difficult to see ureteral calculi by US. So patients without pelvicalyceal dilatation have a disadvantage with US with the risk of false negative results. Doppler RI values in this patient group are so helpful as shown in our study.
In this study normal contralateral kidneys in unilateral urinary obstruction had no elevated resistive index. This suggested that the hemodynamic changes in obstructed kidneys were local intrarenal rather than systemic events as suggested by Ichikawa and Brenner in an animal study [21].
In our study 50% of patients in the obstructed group had a RI lower than 0.70. This phenomenon can be explained by intermittent or partial obstruction. These subgroups have been shown to have relatively normal resistive index values [1, 22]. Another issue of probable relevance is pyelosinus extravasation, which is evident in 10–20% of acutely obstructed kidneys on conventional US and urography [7–9]. Platt et al. [7] have argued that pyelosinus rupture leads to decompression of the collecting system, so that true obstruction is no longer present and, thus, it may be responsible for some false negative results. In addition, they have advocated that the value of a normal RI in a suspected obstructed kidney should be questioned when the slightest amount of perirenal or periureteral fluid is detected [7].
The literature indicates that up to 35% of acutely obstructed kidneys have no sign of dilatation [9], of which about 60% may have positive Doppler US findings indicating obstruction [7]. In our study 31% (5 of 16) of acutely obstructed kidneys had no sign of dilatation with gray scale US. In this group 60% (3 of 5 kidneys) had mean RI > 0.70 indicating obstruction.
The application of an adequate Doppler US technique is essential for obtaining accurate results. The most common reason for obtaining a normal RI in the presence of significant obstruction is a technical error that is simple to correct. As described previously, the use of the correct scale (pulse-repetition frequency) to expand the waveform size to fill as much of the available display as possible, without aliasing, is crucial [23]. With this strategy, errors in measurements of RI can be reduced and flow at the end of the diastole generally can be differentiated from background machine noise and the wall filter. Failure to make this simple technical correction results in minute waveforms barely deviating from the baseline; when measured, these waveforms invariably result in an RI that is calculated to lie within the normal range, even when a true state of elevated renal arterial resistance is present [24]. In our study we used an optimal Doppler US technique to have objective values.
Although it is uncommon in clinical practice ureteral calculus may occur in the unhealthy kidney such as atrophic kidney. We could not find any study in the literature regarding Doppler changes in the obstructed atrophic kidney by ureteral calculus. Resistive index increase is caused by several competing hormonal factors, the most important of which seems to be mediated by prostaglandin [24]. So we think that the type of anomaly (atrophy or congenital anomaly) will affect the releasing of this mediator and pathophysiology of resistive index increase. So resistive index increase may not be a reliable indicator on unhealthy kidneys. Another potential limitation of Doppler US is that the resistive index could be elevated in conditions other than renal obstruction, e.g. chronic hypertension and renal medical diseases. Therefore, in the setting of known renal medical diseases and renal colic, an elevated RI could be caused by the renal disease or obstruction, thus limiting the value of the abnormal RI in this particular situation. The importance of ΔRI in such a condition is also unknown. However, a normal RI in this setting would still be helpful in arguing against the presence of obstruction [25].
Finally, this study supplements the existing evidence that, in acutely obstructed kidneys, renal Doppler recording can demonstrate altered renal perfusion before pelvicalyceal system dilatation and distinguish obstructed and unobstructed kidneys evaluated with suspicion of renal colic.
References
Rodgers PM, Bates JA, Irving HC (1992) Intrarenal Doppler ultrasound studies in normal and acutely obstructed kidneys. Br J Radiol 65:207–212
Platt JF, Rubin JM, Ellis HM et al (1989) Duplex Doppler US of the kidney:differentiation of obstructive from non-obstructive dilatation. Radiology 17:515–517
Shokeir AA, Provoost AP, El-Azab M et al (1997) Renal Doppler ultrasound in children with obstructive uropathy: effect of intravenous normal saline fluid load and furosemide. Br J Urol 80:313–318
Shokeir AA, Nijman RJ, El-Azab M et al (1997) Partial ureteral obstruction: effect of intravenous normal saline and furosemide upon the renal resistive index. J Urol 157(3):1074–1077
Rawashdeh YF, Djurhuus JC, Mortensen J et al (2001) The intrarenal resistive index as a pathophysiological marker of obstructive uropathy. J Urol 165:1397–1404
Aslaksen A, Gothlin JH (1990) Ultrasonic diagnosis of ureteral calculi in patients with acute flank pain. Eur J Radiol 11:87–90
Platt JF, Rubin JM, Ellis JH (1993) Acute renal obstruction: evaluation with intrarenal duplex Doppler and conventional US. Radiology 186:685–688
Erwin BC, Carroll BA, Sommer FG (1984) Renal colic: the role of ultrasound in initial evaluation. Radiology 152:147–150
Laing FC, Jeffrey RB Jr, Wing VW (1985) Ultrasound versus excretory urography in evaluating acute flank pain. Radiology 154:613–616
Hill MC, Rich JI, Mardiat JG, Finder CA (1985) Sonography vs. excretory urography in acute flank pain. AJR Am J Roentgenol 144:1235–1238
Amis ES, Cronan JJ, Pfister RC, Yoder IC (1982) Ultrasonic inaccuracies in diagnosing renal obstruction. Urology 19:101–105
Rascoff JH, Golden RA, Spinowitz BS, Charytan C (1983) Non-dilated obstructive nephropathy. Arch Intern Med 143:696–698
Webb JAW (2000) Ultrasonography and Doppler studies in the diagnosis of renal obstruction. BJU Int 86(Suppl 1):25–32
Chen JH, Pu YS, Liu SP, Chiu TY (1993) Renal hemodynamics in patients with obstructive uropathy evaluated by duplex Doppler soography. J Urol 150:18–21
Dodd GD, Kaufman PN, Bracken RB (1991) Renal arterial duplex Doppler ultrasound in dogs with urinary obstruction. J Urol 145:644–646
Ulrich JC, York JP, Koff SA (1995) The renal vascular response to acutely elevated intrapelvic pressure: resistive index measurements in experimental obstruction. J Urol 154:1202–1204
Opdenakker L, Oyen R, Vervloessen I et al (1998) Acute obstruction of the renal collecting system: the intrarenal resistive index is a useful yet time-dependent parameter for diagnosis. Eur Radiol 8:1429–1432
Sauvain JL, Pierrat V, Chambers R et al (1989) Ultrasound and pulsed Doppler in the study of the arteries of the renal parenchyma during obstructive syndromes and dilatation of the excretory cavities of the kidney. J Radiol 70:389–398
Haroun A (2003) Duplex Doppler sonography in patients with acute renal colic: prospective study and literature review. Int Urol Nephrol 35:135–140
Akçar N, Özkan IR, Adapınar B, Kaya T (2004) Doppler sonography in the diagnosis of urinary tract obstruction by stone. J Clin Ultrasound 32:286–293
Ichikawa I, Brenner BM (1979) Local intrarenal vasoconstrictor–vasodilator interactions in mild partial ureteral obstruction. Am J Physiol 236:F131
Miletic D, Fuckar Z, Sustic A et al (1998) Resistance and pulsatility indices in acute renal obstruction. J Clin Ultrasound 26:79
Platt JF, Ellis JH, Rubin JM (1995) Role of renal Doppler imaging in the evaluation of acute renal obstruction. Am J Roentgen 164:379–380
Shokeir AA, Abdulmaaboud M (1999) Resistive index in renal colic: a prospective study. BJU Int 83:378–382
Shokeir AA, Provoost AP, Nijman RJM (1997) Resistive index in obstructive uropathy. Br J Urol 80:195–200
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Onur, M.R., Cubuk, M., Andic, C. et al. Role of resistive index in renal colic. Urol Res 35, 307–312 (2007). https://doi.org/10.1007/s00240-007-0116-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-007-0116-2