
Abstract
Background
Acute ureteric colic is one of the most commonly encountered acute abdominal conditions. Diagnosis of obstruction caused by ureteric calculus occasionally becomes challenging if there is inadequate dilation of the urinary tract proximal to obstruction. In such a situation, intra-renal artery Doppler parameters can be used as a diagnostic tool. Our study compared intra-renal arterial Doppler in patients with obstructed and non-obstructed kidneys presenting within 24 h of onset of symptoms of unilateral acute renal colic.
Results
The resistivity index (RI) in the segmental arteries of all 54 patients with obstructed kidneys was significantly higher than in those with non-obstructed kidney: 0.75 vs. 0.56, with a p value less than 0.001, a sensitivity of 85% and a specificity of 93%.
Conclusion
Doppler ultrasound is a useful diagnostic tool in the evaluation of acute renal obstruction, thus enabling practitioners to avoid ordering unnecessary CT and exposing patients to ionizing radiation. An RI value > 0.7 has good sensitivity and specificity in our study. The results obtained in the study were comparable to those of pioneer studies conducted worldwide.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Acute renal colic (ARC) is one of the common causes of patients presenting to the emergency room (ER). It accounts for 30–35% of urologic emergencies [1, 2]. The recurrence rate over a period of 5 years is 30–40% [2]. Ultrasonography (US) remains the most commonly used modality in the initial evaluation of patients presenting with acute abdomen, especially in children [3], and the utility of ultrasound in the diagnosis of ARC cannot be overstated in cases where ARC is one of the most common pathologies presenting as acute abdomen. Absence of significant dilatation of the pelvicalyceal system, in spite of severe obstruction being present, is a well-recognized finding in some patients. In some studies, the absence of significant dilation in ARC has been reported in up to 30% [4] of patients. The dilated collecting system seen in US need not always be due to obstruction in the downstream urinary tract. These conditions include a baggy extra-renal type of pelvis, a compound upper pole calyx, due to over-distended urinary bladder, vesico-ureteric reflux, congenital type of mega calyces, infection and residual dilatation due to previous obstruction. Very rarely, pseudo-aneurysms of intra renal arteries can mimic renal pelvi-ectasis. This kind of vascular pathology can also be easily diagnosed with CDUS [5]. Acute complete ureteric obstruction is associated with changes in renal blood flow, as well as with an increase in renal pelvic pressure. In the first few hours, renal blood flow increases, and after 3 to 5 h, renal blood flow decreases, probably because of efferent arteriolar vasoconstriction produced by prostaglandins and other vasoactive substances [6, 7]. These changes can be effectively demonstrated by the RI of intra-renal arteries, as measured by Doppler ultrasound.
Methods
A prospective study was done on 54 patients who were referred to the department of radiology with clinical features of ARC for further evaluation with ultrasound or non-contrast CT. The study period is from January 2015 to December 2017. Prior to the commencement of the study, necessary clearance was obtained from the institutional ethics committee, and informed written consent was obtained from all the participating patients.
Inclusion criteria
All patients with symptoms of acute ureteric obstruction presenting to the emergency department within 24 h of onset of unilateral ARC were included.
Exclusion criteria
(a) Patients with history of renal parenchymal disease, chronic renal obstruction, renal trauma, or bilateral renal obstruction; (b) patients with a single kidney; and (c) patients in whom ureteric obstruction could not be confirmed either with USG or with CT were excluded.
All patients underwent gray-scale ultrasonography (US) and Doppler evaluation of intra-renal arteries. Computed tomography (CT) was done for those patients in whom US could not confirm the cause of obstruction.
Evaluation by ultrasound and Doppler study
The kidney on the side of obstruction was treated as the case kidney, and the contralateral normal (non-obstructed) kidney served as control. All patients underwent B-mode US and color doppler ultrasound (CDUS) with Philips iU22 using a C 1–5 transducer and Siemens Acuson S3000 using a 6C1 HD transducer. The presence or absence of pelvicalyceal system dilatation in each kidney was assessed using the gray-scale images. At least three Doppler spectra were obtained from inter-lobar arteries along the border of the medullary pyramids, and their mean was taken (Fig. 1).

Doppler US demonstrating an RI value of 0.74 in the mid pole of left kidney (obstructed kidney)
The Doppler waveforms were made using the lowest pulse repetition frequency possible without aliasing. This maximized the size of the Doppler spectrum and decreased the percentage error in the measurements. In addition, the lowest possible wall filter for each ultrasound scanner was used. The Doppler sample width was set at 2–3 mm. The renal RI was calculated using the standard formula. The mean RI value was calculated for each kidney.
Evaluation by computed tomography
Siemens SOMATOM Definition Edge 128 slice Computerized Tomography (CT) equipment was used for the study. Non-enhanced CT of the abdomen, extending from the dome of the diaphragm to the pubic symphysis, was performed in all patients in whom the site and cause of obstruction could not be confirmed with US. Raw data was acquired with 0.6 mm thickness and pitch of 0.8. Reconstruction from the raw data was done in 5 mm thickness for viewing purposes and in 1 mm thickness for coronal and sagittal multi-planar reconstruction (MPR) (Fig. 2). The sites of ureteric obstructions were identified. Those patients not confirmed to have obstructions by CT were excluded from the study.

Sagittal reconstruction of non-enhanced CT showing a calculus in the left distal ureter who presented with acute left renal colic
Statistical methods
All data were systematically collected, tabulated and analyzed using Microsoft Excel and Strata 6 for Windows. The Student t test was used in univariate analysis for the continuous variables, and Chi square test was used for analysis of noncontiguous variables. A p value of less than 0.05 was considered to be statistically significant.
Results
This study evaluated 54 patients who had presented to the EMD with unilateral ARC within 24 h of the onset of symptoms. All the patients underwent B-mode US, CDUS and CT if the obstruction could not be confirmed in US. The presence or absence of PCS dilatation in each kidney was assessed using the grey-scale images. In this study population, 34 patients were males and 20 were females, as shown (Fig. 3). The mean age of the male patients was 46.8 years and that of the female patients was 38.5 years. The age range of the male patients was 19–79 years, and that of the female ones was 18–61 years.

Sex distribution in the study population
The modalities used in the diagnosis and the site of obstruction are shown in Tables 1, 2.
Out of 54 patients, 26 cases proximal obstructions, while 28 had distal obstructions. The mean RI of the obstructed kidneys was higher in cases of distal obstruction (0.79 ± 0.004) than in those of proximal obstruction (0.76 ± 0.006).
Of the 54 patients, 45 patients had mild hydronephrosis, FIVE patients had moderate hydronephrosis and four patients did not have any dilatation of the collecting system despite the presence of ureteric obstruction (Fig. 4).

Degree of hydronephrosis in the study population
Of the 54 patients who were included in this study, 27 patients had elevated renal parameters, but did not have history of chronic renal impairment (Table 3).
In our study, we found that the RI in obstructed kidneys was significantly higher than in unobstructed kidneys (0.75 vs. 0.56; p < 0.001). The RI was higher in obstructed kidneys in all cases. The difference in RI between the obstructed and unobstructed kidneys (delta RI) ranged from 0.09 to 0.38, with a mean delta RI of 0.24 (Table 4).
The RI values in obstructed kidneys ranged from 0.68 to 0.84 (Fig. 5). The mean RI value in obstructed kidneys was 0.75, compared to 0.56 in unobstructed kidneys.

Mean RI values in obstructed kidneys
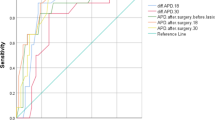
The group statistics of RI are shown in Tables 5, 6. The receiver operating characteristic curve (ROC) curve depicting the sensitivity of RI in ureteric obstruction is shown in Fig. 6.

ROC curve showing the sensitivity and specificity of resistive index
By using a cut off RI value of > 0.70 in acute unilateral renal obstruction, the sensitivity obtained in the study was 85% and the specificity was 93% (Table 7).
Discussion
Grayscale ultrasound is the investigation method of choice in the initial evaluation of ARC, as it is easily available, portable and involves no ionizing radiation [8, 9]. However, urinary system dilatation seen on conventional gray-scale USG has been shown to be sensitive (90%), but not specific (65–84%), in the diagnosis of renal obstruction.
The most sensitive, gold standard test for diagnosing obstructive uropathy is renal scintigraphy. However the availability of scintigraphy and radiation associated with it continue to be problematic [10]. Traditionally, the evidence of renal obstruction provided by US has been indirect and dependent on the anatomical criterion of dilatation of the pelvicalyceal system and ureter proximal to the level of obstruction. However, US fails to reveal hydronephrosis in acute obstruction of the kidney in up to 35% of cases [11]. More direct functional evidence of obstruction usually requires scintigraphy, but recently Doppler US techniques have been used to obtain functional information in suspected renal obstruction [11]. US imaging may miss (false negative) the diagnosis of obstruction in a variety of situations. Mild dilatation may be overlooked or considered clinically insignificant. Some patients with obstructive renal failure may show no pelvicalyceal system (PCS) dilatation. The reasons for this are unclear; in some patients, it may be related to dehydration or due to decompression of the pelvicalyceal system by rupture of a calyceal fornix [12]. It is commonly explained by urologists to be caused by the use of non-steroidal anti-inflammatory drugs (NSAIDs), by dehydration or by the renin angiotensin effect [13]. If that is true, such impairment will be detected through measurement of glomerular filtration rate (GFR). Measurement of GFR is commonly done using Technetium c-99 m diethylene-triamine-penta-acetate (DTPA), and does not require blood or urine sampling [14]. There is a growing evidence that renal impairment in acute unilateral ureteric obstruction is due to absorption of obstructed urine, with its high amount of creatinine, back into systemic circulation. This is considered false renal impairment with normal GFR [15]. In a study, El-Shazly et al. [16] measured renal function through measurement of estimated GFR (eGFR) usingTc-99 m DTPA. The authors showed that differences between eGFR on admission and after passage of stone or relieve of obstruction were non-significant. Their results support the hypothesis of false impairment in this clinical scenario. This tends to change the practice, as there is no need to embark on urgent intervention to relieve the ureteric obstruction, and conservative medical management is justifiable.
Routine B-mode US can be falsely positive or negative in acute ureteric obstruction [10]. PCS dilatation may be missed if the system is filled with blood clots, calculus, tumors or pus, in which case the usual anechoic appearance of the PCS is lost. Intermittent ureteric obstruction, particularly that caused by ureteric calculi, may also lead to a failure to visualize dilatation of collecting system with US. On the other hand, in an attempt not to miss the diagnosis of obstruction in patients with only mild PCS dilatation, the false positive rate was found to be as high as 26% Causes of a false positive diagnosis include: (i) dilatation of non-obstructed PCS, when there are anatomical variants such as extra-renal pelvis; (ii) over-distended urinary bladder, with or without diuresis; (iii) vesico-ureteric reflux (VUR), (iv) residual dilatation of PCS due to previous obstruction or infection; (v) advanced pregnancy; and (vi) central renal fluid collections other than in the PCS, including in normal vessels, renal artery aneurysms and para-pelvic cysts.
Acute unilateral ureteric obstruction results in a complex sequence of changes in renal blood flow and ureteric pressure [17]. In the first two hours, the renal blood flow increases, because of afferent arteriole vasodilatation and the ureteric pressure increases. From two to six hours after obstruction, the renal blood flow decreases, secondary to vasoconstriction of the efferent arterioles, and the ureteric pressure remains elevated. Subsequently, at 6 to 18 hours, the renal blood flow remains reduced because of vasoconstriction of the afferent arterioles, and the ureteric pressure decreases.
The role of renal CDUS in the evaluation of ARC has been vigorously debated. Rodgers et al. [18] found an elevated RI in acutely obstructed kidneys, especially when compared with the RI in normal contralateral kidneys and with a control group of healthy subjects. Similar results were obtained by Platt et al. [19] in a study of 23 patients with acute unilateral ureteric obstruction. However, others have reported that Doppler ultrasound is highly insensitive for detecting ARC. Tublin et al. [20] correlated the results of Doppler USG with those of urography in 32 patients presenting with symptoms of renal colic. The RI value of normal kidneys is usually less than 0.7 [21, 22]. When the published discriminatory thresholds for obstruction (mean RI ≥ 0.70 and ΔRI ≥ 0.10) were applied, the sensitivity and specificity of Doppler USG were only 44% and 82%, respectively.
In our study of 54 patients, we found that the RI in obstructed kidneys was significantly higher than in the unobstructed kidneys (0.75 vs. 0.56; p < 0.001). The RI was higher in obstructed kidneys in all cases. The difference between the obstructed and unobstructed kidneys (delta RI) ranged from 0.09 to 0.38, with a mean delta RI of 0.24.
Saboo et al. [6] stated in their study that delta RI ≥ 0.006 was highly sensitive and specific, and with a higher delta RI specificity remained the same whereas the sensitivity fell rapidly. Our results correlate well with those reported in earlier studies by Badr et al. [23] and Miletic et al. [24].
We also studied the effect of the level of obstruction on RI values. When we compared levels of ureteric obstruction (proximal vs distal), distal obstructions had a higher mean RI value (0.79) than proximal obstructions (0.76), and the values were not statistically significant. However, the study done by de Toledo et al. [25] showed that patients with proximal ureteric obstructions have RIs higher than those with distal obstructions.
We also analyzed the utility of CDUS in patients who did not show dilatation of the PCS on ultrasound. Patients who did not have PCS dilatation on US were later confirmed to have obstruction on CT. RI values were higher in all these patients (0.71), with a delta RI of 0.24. Discriminatory RI ≥ 0.70, which is higher than the delta RI found in the study done by Platt JF et al. [26], was found to be highly sensitive (85%) and specific (93%) in this study.
Conclusion
Using the discriminatory threshold RI of ≥ 0.70, the overall sensitivity of CDUS in diagnosing acute ureteric obstruction is 85% and the specificity is 93%. CDUS is a useful tool for demonstrating altered renal perfusion in acute ureteric obstructions before pelvicalyceal system dilatation occurs, thus increasing the sensitivity and specificity. Gray-scale US should therefore, be complemented by CDUS as an adjunctive test in patients presenting with acute renal colic, as it is a very simple, noninvasive and easy-to-calculate parameter. The utility of this tool cannot be overemphasized in special cases like pregnant women and children, in whom a dilated pelvicalyceal system without acute obstruction is encountered more frequently. It is mandatory to differentiate obstructive and non-obstructive causes with US alone in this subset of patients, as further evaluation with CT is not desirable due to the hazard of ionizing radiation. Given the high propensity of any group of patients with urinary tract calculi to undergo frequent imaging studies due to recurrent ureteric colic and the presence of significant residual hydronephrosis, we should strive hard to minimize radiation dosage by avoiding frequent CT studies. At the same time, maintaining acceptable diagnostic accuracy is of paramount importance.
Limitations of the study: US is an operator-dependent examination and the results are affected by patients’ body habitus and availability of good window. An increase in the RI of intra-renal vessels is also found in case of vascular or parenchymal diseases (renal vein thrombosis, acute renal insufficiency, etc.). The CDUS changes can return to normal after 48 h [27], after which its utility is doubtful with reduced sensitivity and specificity.
Abbreviations
- ARC:
-
Acute renal failure
- ER:
-
Emergency room
- USG:
-
Ultrasonography
- US:
-
Ultrasound
- RI:
-
Resistive index
- CT:
-
Computed tomography.
- NSAID:
-
Non-steroidal anti-inflammatory drugs
- GFR:
-
Glomerular filtration rate
- eGFR:
-
Estimated glomerular filtration rate.
- Tc99m DTPA:
-
Technetium−99 m- Diethylene-triamine- penta-acetate
- CDUS:
-
Color Doppler Ultrasound
- MPR:
-
Multiplanar reconstruction
- ROC:
-
Receiver operating characteristic curve
- PCS:
-
Pelvicalyceal system
References
Piazzese EMS, Mazzeo GI, Galipo S, Fiumara Canfora F, Angio LG (2012) The renal resistive index as a predictor of acute hydronephrosis in patients with renal colic. J Ultrasound 15:239246
Sterrett S, Stephen N (2009) Emergency room follow-up trends in urolithiasis: single-center report. Urology 73:1195–1198. https://doi.org/10.1016/j.urology.2008.07.057
di Giacomo V, Trinci M, van der Byl G, Catania VD, Calisti A, Miele V (2014) Ultrasound in newborns and children suffering from non-traumatic acute abdominal pain: imaging with clinical and surgical correlation. J Ultrasound. https://doi.org/10.1007/s40477-014-0087-4
Ravindernath ML, Mahender Reddy G (2017) Mean resistive index as a prognostic tool for hydronephrosis in patients with acute renal colic: a study in a tertiary care. Int J Adv Med 4(2):329–333. https://doi.org/10.18203/2349-3933.ijam20170996
Tufano A, Minelli R, Rossi E, Brillantino C, Di Serafino M, Zeccolini M, Cantisani V, Vallone G (2017) Inferior epigastric artery pseudoaneurysm secondary to port placement during a robot-assisted laparoscopic radical cystectomy. J Ultrasound. https://doi.org/10.1007/s40477-020-00442-1
Saboo SS, Soni SS, Saboo SH, Chinapuvvula NR, Kaza S (2007) Doppler sonography in acute renal obstruction. Indian J Radiol Imaging 17:188–192
Azmi H (2003) Duplex doppler sonography in patients with acute renal colic: prospective study and literature review. Int Urol Nephrol 35(2):135–140
Jindal G, Ramchandani P (2007) AFP secondary to urolithiasis: radiologic evaluation and alternate diagnoses. Radiol Clin N Am 45(2007):395–410. https://doi.org/10.1016/j.rcl.2007.04.001
Apoku N, Ayoola O et al (2015) Ultrasound evaluation of obstructive uropathy and its hemodynamic responses in southwest Nigeria. Int Braz J Urol. 41:556–561. https://doi.org/10.1590/S1677-5538.IBJU.2014.0197
Ruiz-Martíneza A, Sierra-Díazb E et al (2019) Renal Doppler ultrasound resistive index vs renal scintigraphy with 99mTc-DTPA as diagnostic test for ureteropelvic junction obstruction in children. Actas Urol Esp 43(8):419–424. https://doi.org/10.1016/j.acuro.2019.02.005
Granata A, Zanoli L, Clementi S, Fatuzzo P, Fiorini F (2014) Resistive intrarenal index: myth or reality? Br J Radiol 87:20140004. https://doi.org/10.1259/bjr.20140004
Arumuham V, Brodie A, Bycroft J (2019) The management of urolithiasis. Surgery 37:7. https://doi.org/10.1016/j.mpsur.2019.04.003
Al-Ani A, Al-Jalham K, Ibrahim T, Majzoub A, Al-Rayashi M, Hayati A, Mubarak W et al (2015) Factors determining renal impairment in unilateral ureteral colic secondary to calcular disease: a prospective study. Int Urol Nephrol 47(7):1085–1090
Prigent A, Cosgriff P, Gates GF, Granerus G, Fine EJ, Itoh K, Peters M et al (1999) Consensus report on quality control of quantitative measurements of renal function obtained from the renogram: international consensus committee from the scientific committee of radionuclides in nephrourology. Semin Nucl Med 29(2):146–159. https://doi.org/10.1016/s0001-2998(99)80005-1
Rosenzweig B, Pinthus JH, Kleinmann N, Joffe E, Erlich T, Fridman E, Winkler H et al (2015) The relative contribution of urine extravasation to elevate plasma creatinine levels in acute unilateral ureteral obstruction. Can Urol Assoc J 9(7–8):428–433. https://doi.org/10.5489/cuaj.2804
El-Shazlya M, Aziza M et al (2016) Acute unilateral ureteric obstruction in young men with high serum creatinine: is it true or false renal impairment? World J Nephrol Urol 5(3):51–53
Sayani R, Ali M et al (2012) Functional evaluation of the urinary tract by duplex Doppler ultrasonography in patients with acute renal colic. Internat J Nephrol Renov Dis 5:15–21. https://doi.org/10.2147/IJNRD.S27628
Rodgers PM, Bates JA, Irving HC (1992) Intrarenal Doppler ultrasound studies in normal and acutely obstructed kidneys. Br J Radiol 65(771):207–212. https://doi.org/10.1259/0007-1285-65-771-207
Platt J, Ellis J, Rubin J (1991) Examination of native kidneys with duplex Doppler ultrasound. Semin Ultrasound CT MR 12:308–318
Tublin ME, Bude RO, Platt JF (2003) The resistive index in renal Doppler sonography: where do we stand? AJR Am J Roentgenol 180(4):885–892. https://doi.org/10.2214/ajr.180.4.1800885
Drudi FM, Liberatore M, Cantisani V et al (2014) Role of color Doppler ultrasound in the evaluation of renal transplantation from living donors. J Ultrasound. https://doi.org/10.1007/s40477-014-0077-6
Spatola L, Andrulli S (2015) Doppler ultrasound in kidney diseases: a key parameter in clinical long-term follow-up. J Ultrasound. https://doi.org/10.1007/s40477-016-0201-x
Badr K, Brenner B (1988) Renal circulatory and nephron function in experimental obstruction of the urinary tract. In: Brenner BM, Lazarus J (eds) Acute renal failure. Churchill Livingstone, New York, pp 91–118
Miletic D, Fuckar Z, Sustic A, Mozetic V, Smokvina A, Stancic M (1998) Resistance and pulsatility indices in acute renal obstruction. J Clin Ultrasound 26(2):79–84
Toledo De et al (2017) Doppler-duplex ultrasound in renal colic. Eu J Radiol 23(2):143–1481996
Platt JF, Rubin JM, Ellis J (1989) Distinction between obstructive and nonobstructive pyelocaliectasis with duplex Doppler sonography. AJR Am J Roentgenol 153(5):997–1000. https://doi.org/10.2214/ajr.153.5.997
Gul H, Habib I et al (2014) Diagnostic accuracy of renal arterial resistive index in acute renal colic. KJMS 7:1
Acknowledgements
Nill.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
VM: Conception, Design, Acquisition, Analysis and Interpretation of data, Review. KMS: Design, Acquisition, analysis, Interpretation. NE: Concept, Design, Review. BD: Concept, Design. All the authors have read the manuscript and approve the manuscript fully for publication.
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethics approval
Obtained from the Institutional Human Ethics committee (IHEC) of PSG institute of Medical sciences and Research, Coimbatore, Tamilnadu, India. Reference Number: 15/417.
Consent to participate
It was obtained from each patient at the time of Ultrasound Scan and CT (wherever applicable) along with general consent prescribed by the institution. This consent is a verbal consent since no additional procedure was done or drugs were administered for the purpose of the study. The ultrasound and CT Scan (wherever applicable) were done at the request of the referring physician and only those studies performed at the request of the referring clinician were utilized for the study. It is approved by the institutional ethics committee.
Consent for publication
Obtained from all the authors all the authors have read and approved the manuscript.
Availability of data and material
Available.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Viyannan, M., Kappumughath Mohamed, S., Nagappan, E. et al. Doppler sonographic evaluation of resistive index of intra-renal arteries in acute ureteric obstruction. J Ultrasound 24, 481–488 (2021). https://doi.org/10.1007/s40477-020-00539-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40477-020-00539-7