
Abstract
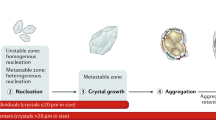
Kidney stone formation is a multifactorial disease in which the defence mechanisms and risk factors are imbalanced in favour of stone formation. We have proposed a novel infectious agent, mineral forming nanobacteria (NB), to be active nidi that attach to, invade and damage the urinary epithelium of collecting ducts and papilla forming the calcium phosphate center(s) found in most kidney stones. Stone formation may proceed in urine supersaturated with calcium phosphate, calcium oxalate and uric acid/urate under the influence of crystallization promoters and inhibitors. Our hypothesis underlines the role of active nidi: even supersaturated urine requires nidi for crystallization to appear.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The current probability of becoming affected by kidney stone disease in the western world ranges geographically from 5% to 13% [39]. The disease has numerous risk factors: genetic hereditary diseases, such as hyperoxaluria and Dent's disease [41], metabolic diseases, such as hyperparathyreosis, life style and diet (eating, drinking) [50]. However, all of these factors cannot fully explain calcium stone formation. Ideas for risk factors and treatment or prevention of the disease have changed much in the recent years. However, nobody knows how the majority of cases without any metabolic/biochemical disorder should be treated to prevent the recurrence of stone attack. There was hope that reducing calcium from diet would help, but this only increased stone recurrence [31]. The hope placed on oxalate-eating bacteria introduced into the gut [43] has diminished because the immune system and antibiotic treatments may destroy the bacteria. Current knowledge on biochemical markers for risk factors and beneficial factors in urine is controversial. A consensus exists that urinary supersaturation is bad and high concentrations of citrate and possibly magnesium [42] are good. Otherwise, the etiological factors and thus mechanisms and treatment strategies remain poorly understood.
Characteristics of nanobacteria
Nanobacteria (NB) were discovered as a contaminating agent in cell culture over 10 years ago. Despite visible biomass present on a cell culture dish, standard microbiological methods failed to detect any known microbe [24]. Culture studies indicated that the novel agent was apparently indefinitely passagable in cell culture medium (beyond 10 years) and could adapt to growing in plain DMEM or RPMI-1640. Omitting serum supplementation resulted in larger cells [10, 22] being formed inside cavities formed by thick apatite layers (Fig. 1a, c, d). In old cultures, large colonies with slimy, but only slightly mineralized walls (arrows in Fig. 1b) were observed indicating social behaviour. Figure 1b also shows the release of tiny forms of NB from the colony. Further studies with electron microscopy revealed mineralized igloos consisting mainly of carbonate apatite (Fig. 1d). Such igloos could grow in size, bud-off new ones and fuse with others to form stones visible to the naked eye (Fig. 2a). Mineral growth took place as concentric layers of elongated nanoscale crystals of apatite with intervening pore structures (Fig. 2b). What was the source of this growth?

Nanobacteria (NB) cultured without serum in DMEM, a phase contrast microscopy image, magnification 800×. The arrow shows a mineralized colony with two large organisms inside a mineralized igloo. b NB biofilm in DMEM. The micrograph shows a large community with relatively thin walls, see the two arrows. Small particles have been released outside the community. Magnification 800×. c Transmission electron microscopy (TEM) micrograph of a section of NB igloo. The micrograph shows an igloo similar to that in a. A layer of apatite crystals is evident on the surface. Bar=0.2 μm. d Scanning electron microscopy (SEM) micrograph of igloos. Bar=1 μm

SEM micrograph of cultured NB showing budding and fusion of spheroids, forming a large stone. Bar=10 μm. b Detail of the previous area showing fractured top surface. Highly organized architecture with tiny elongated apatite crystals is evident. The arrow shows an apparent pore between adjacent crystals. Bar=1 μm. c SEM micrograph of NB cultured from human kidney stone. The arrow points to a broken spheroid which has a highly organized lamellar wall. Bar=10 μm. d SEM micrograph of a fractured human kidney stone revealing spheroid particles with a similar structure to c. Bar=1 μm
Cultures established with some fetal bovine serum (FBS) batches revealed growth of the mineralizing agent as dense particles having a diameter of 80 nm to 500 nm (Fig. 3a–d). Gamma irradiation abolished culture positivity. When the gamma-irradiated serum culture was inoculated with unirradiated positive serum or cultured agent, growth was restored. In this way, the source of the agent was tracked to 'sterile' FBS used as a supplement for culture medium [24]. Over 80% of tested commercial FBS batches from many different manufacturers were positive for NB [26]. NB were found in a significant number of humans as well, in serum and/or in urine. To date, NB have been isolated from bovine serum and from human serum, urine, kidney stones, dental stones and tissue samples [12, 13, 19, 24, 38, 49]. Interestingly, NB show improved growth properties in artificial urine [6]. The general characteristics of NB are given in Table 1. The compilation of data is based on research results obtained by the present authors on a standard "strain" (SeraLab901045). Intrastrain differences due to prolonged culture have been found in cytotoxicity [8] and in the kinetics of elimination into urine after intravenous injection into rats [1].

TEM micrograph of a sample from NB culture in DMEM supplemented with 10% FBS. Negative staining technique omitting the stain. Bar=1 μm. b TEM micrograph of NB culture sample incubated for 20 min with colloidal gold-conjugated anti-NB 8D10 monoclonal antibody, otherwise as in a. Three approximately 20 nm-sized gold-particles are indicated by the arrow. There is highly significant binding of the gold-labelled antibody to NB. Bar=0.12 μm. c TEM micrograph of NB subjected to negative staining with 2% uranyl acetate. Bar=1 μm. d TEM image as in c at high magnification. Mucus-protein layer surrounding NB can be seen (see arrow in c). Such a sticky layer apparently helps NB to adhere on surfaces, to grow as a social colony or biofilm, and promotes apatite crystallization. Bar=0.1 μm
In addition to culture methods [9], several other diagnostic tools have been developed for the identification of NB. One of the most powerful methods is transmission electron microscopy (TEM). TEM sample preparation for negative staining takes only a few minutes and allows for the detection of NB as dark particles, due to their apatite content [33]. As shown in Fig. 3, NB culture sample dried on a carbon-coated grid can be inspected either without staining, or after staining with 2% uranyl acetate. The latter reveals slimy material around the particles (Fig. 3c,d). The most powerful tool is a novel technique in which an unstained grid is incubated for 20 min with colloidal gold-labelled anti-NB antibody, washed, dried and inspected (Fig. 3b). The antibody reveals its target (NB surface epitope) inside of the slimy material on the NB surface. These techniques allow imaging at high resolution without any fixation steps. NB have apatite mineral as a structural support, which makes them visible and so robust that fixation is unnecessary for TEM. This is a unique feature of NB, which allows fast and specific diagnosis using electron microscopy.
As shown in Table 1, many properties of NB are rare and extreme. Relatively tiny mineral-associated microbes have been found by geologists [17, 48]. Older findings link such small forms to cancer [51]. Many properties of NB support the theory that they might be primitive life forms [25]. The extremophilic characteristics of NB would be beneficial in surviving hostile conditions [4, 23]. Several groups are researching NB and have succeeded in the detection or culture of NB or NB-like forms [6, 15, 18, 19, 32, 38, 49]. However, the concept that NB are living organisms is controversial as long as their putative nucleic acid is not sequenced.
How nanobacteria are involved in stone formation?
The theory of NB-linked stone formation [28] is based on: (1) finding NB in kidney stones (Fig. 2d), (2) finding similar forms of NB in kidney stones culture (Fig. 2c), (3) in vitro calcific stone formation by NB (Fig. 1c, d, 2a, b), and (4) kidney stone formation after NB inoculation to rat kidneys. In a study by Ciftcioglu et al. [13], 70 out of 72 kidney stones contained NB. The presence of NB was independent of the stone type, although apatite stones gave the highest immunopositivity. Kidney stones were crushed, treated with 1 M HCl followed by neutralization and then analyzed using culture, immunological methods and electron microscopy. Surprisingly, kidney stones contained NB that started to replicate under culture conditions and formed calcium phosphate stones in vitro. In addition, NB were able to produce stony colonies in modified Loeffler medium, cause intra- and extracellular calcium deposits and cell damage in many cultured cell lines [8, 11]. Importantly, dose-dependent kidney stone formation was observed within 1 month in rats after injection of NB using the translumbar, percutaneous renal puncture method [18]. Despite the small number of experimental animals (n=4), the result provides evidence that kidney stone formation can be caused by introducing NB into kidney.
The suggested involvement of NB in kidney stone formation [28] supports the observations made by Carr and Randall [7, 40]. Carr's concretions are small shiny deposits of calcium phosphate in kidney lymphatics and collecting ducts. Calcium phosphate formed above the collecting duct might induce heterogeneous nucleation of calcium oxalate at lower levels of the renal collection system [20] and be a risk factor for Randall's plaque formation [30]. Randall described calcium-containing plaques in the kidney papilla [40]. According to his hypothesis, the formation of kidney stone starts from these plaques due to a primary lesion in the tissue. Cell culture experiments have revealed that the adherence and internalization of calcium oxalate crystals into cultured cells is an active process potentially important for kidney stone formation [29]. Recent studies on NB have produced findings suggesting that NB might be calcium phosphate nidi for kidney stone formation. NB are renotrophic, as reported from rabbit experiments using radiolabelled NB [3]. They are eliminated from the circulation through excretion into the urine [1, 3]. NB were found to adhere, invade and damage cells in collecting tubuli and the papillary area in the rat and rabbit models [3; Kajander, unpublished data]. NB colonization could lead to the accumulation of calcium deposits on the lesions and trigger stone formation as described by Randall.
Nanoscale biocrystallization by nanobacteria
Many kidney stones have a core composed of apatitic spheroids (Fig. 2d). NB cultured from human kidney stones formed apatitic spheroid particles in vitro with a similar architecture to that in kidney stone; observe the broken spheroids in Fig. 2c, d. Tiny nanoscale crystals show a highly organized structure resembling the nanosphere structures found in pearls and other calcium carbonate formations in living bodies. This suggests a protein mediated mineral growth mechanism. Pearls are known to grow in this way. Figure 3c, d indicate that the biomineralization process of NB takes place inside a mucus-protein matrix around the NB that is detectable with uranyl acetate staining. This suggests that nanoscale apatite crystals grow as a result of mucus-protein mediated crystal formation on the surface of NB. This theory was first introduced by Vali et al. [49]. Crystalluria appears to form at a lower urinary ionic concentration in stone formers [16], suggesting higher crystallization potency in these individuals, i.e., active nidi or weaker crystallization inhibitor activity. NB are transportable apatitic nidi from blood into kidney tissue and urine [3], and their active role in crystallization may explain the observation above [13, 22, 28].
Biomineralization is an effective process: apatite formation in vitro stopped only when the calcium level decreased by 50% from 1.8 to 0.9 mM and the phosphate levels fell to near zero [13]. NB can use dolomite [12] and synthetic apatite (Kajander, unpublished observation) as a calcium source. NB-induced biomineralization is dependent on the presence of oxygen [22, 24]. Gamma irradiation at doses that prevented the replication of NB, abolished the biomineralization [14, 24]. Biomineralization was abolished with several antibiotics and antimetabolites that showed a nanobactericidal effect at concentrations relevant for human therapy [14]. Further proof that biomineralization by NB are a biological phenomenon related to being a living entity came from recent experiments with light. Low intensity light treatment (without thermal effects) at certain wavelengths stimulated NB replication as detected by particle numbers, incorporation of uridine and electron microscopy. Concomitantly, light stimulated apatite formation as detected by 85-strontium incorporation [45]. Synthetic apatite did not respond. Biostimulation by light treatment is a general phenomenon observed in living entities from bacteria to mammalian cells with the used light treatment [44, 46].
Macromolecule-calcium phosphate mineral complexes have also been recently observed in human and animal circulation by other researchers [34, 35, 36, 37]. Price hypothesized that these particles cause soft tissue calcification, such as atherosclerosis and kidney calcification. The source of Price's particles was an enigma. These high molecular weight complexes of calcium phosphate together with proteinaceous calcification inhibitors were circulating in rats (subjected to atherogenic treatments) after a single subcutaneous dose of etidronate [36]. The maximum concentration of complexes was observed at 6 h after the drug dose and complexes were cleared from circulation within 24 h after injection. The route of elimination was not studied. The presence of the protein-mineral complex increased total serum calcium and phosphate 1.8- and 1.6-fold, respectively, after a dose of 8 mg/100 g body weight etidronate, and even more with higher doses [36]. It was suggested that the complex originates due to the inhibition of bone mineralization by etidronate [36]. These findings confirm our detection of high molecular weight mineral-protein complexes containing calcium phosphate in serum (NB). We have shown that the treatment of such complexes inside calcific biofilms or stones with bisphosphonates, chelating agents and some antibiotics, resulted in the release of destroyed particles into the medium [14]. We propose an explanation for the appearance of complexes as described by Price et al.: bisphosphonate administration causes the destruction of NB into "popcorn-like" floating particulate debris in a few hours [14], and these detached particles could appear in the blood until removed by the reticuloendothelial system. Bisphosphonates and chelating agents, either alone or together with antibiotics, might thus be useful agents in the treatment of pathological calcification, whether in the form of atherosclerosis or stone formation. In fact, a recent summary advocates bisphosphonate treatment for stopping or preventing atherosclerosis [52], and one earlier report has shown bisphosphonate therapy to decrease the recurrence of kidney stones [5]. Larger studies are warranted, because this approach might have deep implications in the treatment of recurrent kidney stones, nephrocalcinosis and atherosclerosis.
Cisar et al. [15] were able to culture NB-like apatitic particles from human saliva and dental plaques. They reported unsuccessful DNA extraction, failed PCR detection due to bacterial contamination and a negative result from protein isolation although some protein bands were obtained. Their conclusion was that the particles were self-replicating inorganic apatite. The use of positive and negative controls and methods to identify NB could have been used in their study to confirm or exclude the presence of NB, but were not performed. Interpretation should not be based only on failed nucleic acid results. Nucleic acid research on NB has many problems, e.g., nucleic acid extraction is difficult due to apatite and extracted DNA-like material has inhibited the amplification of exogenous bacterial DNA in PCR methods. More effort should be made for the characterization of NB.
Ongoing research on nanobacteria
Ongoing research aims at solving the mystery behind nanoscale biomineralization: What are NB? What are their survival and growth strategies? How do they mineralize and what is their role in kidney stone disease and other calcifications? Does their eradication prevent stone formation? Research is now being carried out by an increasing number of researchers, among others, in the Mayo Clinic and NASA. Effective eradication therapies may arise as a consequence of such international research efforts. New approaches in the treatment and prevention of kidney stones could significantly reduce health care costs and increase the quality of life. Emerging knowledge on the drug sensitivity of nanobacteria/kidney stone forming units [14] suggests that novel treatment strategies could be based on a combination therapy using "old" drugs. A major hindrance in adopting such new therapies can be the reluctance of drug companies to carry out the necessary but expensive clinical studies with generic drugs.
Epidemiological studies are important for determining the prevalence of NB in various populations and diseases. Serum prevalence of the antigen in adult Finnish volunteers is about 5% [26]. Our recent collaboration with Holmberg et al. from Uppsala revealed that about 14% of healthy Swedish blood donors have antibodies to the agent [21]. Furthermore, gamma globulin preparations pooled from thousands of healthy volunteers revealed NB antibodies [2]. In some disease states, e.g. atherosclerosis and hemodialysis, NB markers, antibodies and antigen, can be found in the serum/urine in the majority of cases (Kajander, unpublished data).
Whether NB are bacteria, mineral autocatalytic aggregates or self-replicating biological particles, they should be regarded as an infectious agent which can be involved in the pathogenesis of pathological calcifications. Exposure to NB can cause an immune response and may result in chronic bacteremia. One accidental exposure to NB during laboratory work has been monitored. The exposure was followed by the development of antibodies against NB, antibody levels remaining high for several years after the accident (Kajander, unpublished data). This finding suggests that NB may cause chronic infection without immediate clinical symptoms. It has been estimated that the growth of a 3 mm thick layer of calcium oxalate takes approximately 2.7 years, based on crystal growth rate [47]. For this and other reasons, exposure to NB infection might have serious consequences several years after exposure. It is suspected that biopharmaceuticals might be contaminated via FBS [26] and some viral vaccines were found to contain NB [27]. This possibility should be kept in mind and efforts should be made to determine the role of NB in the etiology of kidney stones and pathological calcification, diseases with an apparently increasing prevalence.
Conclusions
NB remain controversial agents that mediate apatite nucleation and crystal growth. They are renotropic, cause apoptotic cell death, are present in human kidney stones and occasionally in urine. They may trigger renal pathology involving damage to tubular epithelium, biomineralization, and perhaps tubule obstruction and chronic infection resulting in defective tissue repair and stone formation.
References
Aho K (2002) In vivo biodistribution and toxicity of nanobacteria in rodents. In: International Nanobacteria Minisymposium, March 8 2001, Kuopio. Book of abstracts, Kuopio University Press, Kuopio, (in press). Abstract at http://www.nanobac.com/nbminisymp080301/page9.html
Aho K, Kajander EO, Ciftcioglu N, Hjelle JT, Miller-Hjelle MA (2002) Screening of human gamma globulin products for nanobacteria markers. American Society for Microbiology, 102nd General Meeting; May 19–23 2002, Salt Lake City. Abstract Y-10, p. 507.
Akerman KK, Kuikka JT, Ciftcioglu N, Parkkinen J, Bergstrom KA, Kuronen I, Kajander EO (1997) Radiolabeling and in vivo distribution of nanobacteria in rabbit. Proc SPIE Int Soc Opt Eng 3111:436
Bjorklund M, Ciftcioglu N, Kajander EO (1998) Extraordinary survival of nanobacteria under extreme conditions. Proc SPIE Int Soc Opt Eng 3441:123
Bone HG3rd, Zerwekh JE, Britton F, Pak CY (1979) Treatment of calcium urolithiasis with diphosphonate: efficacy and hazards. J Urol 121:568
Burton SK (2001) Nanobacteria growth characteristics and biofilm formation. Proceedings American Society of Microbiology 101st General Meeting, May 20–24, 2001, Orlando. Abstract I-98, p 437
Carr RJ (1954) A new theory of the formation of renal calculi. Brit J Urol 26:105
Ciftcioglu N, Kajander EO (1998) Interaction of nanobacteria with cultured mammalian cells. Pathophysiology 4:259
Ciftcioglu N, Kajander EO (2000) Growth factors for nanobacteria. Proc SPIE Int Soc Opt Eng 3755:113
Ciftcioglu N, Pelttari A, Kajander EO (1997) Extraordinary growth phases of nanobacteria isolated from mammalian blood. Proc SPIE Int Soc Opt Eng 3111:429
Ciftcioglu N, Bjorklund M, Kajander EO (1998) Stone formation and calcification by nanobacteria in human body. Proc SPIE Int Soc Opt Eng 3441:105
Ciftcioglu N, Ciftcioglu V, Vali H, Turcott E, Kajander EO (1998) Sedimentary rocks in our mouth: dental pulp stones made by nanobacteria. Proc SPIE Int Soc Opt Eng 3441:130
Ciftcioglu N, Bjorklund M, Kuorikoski K, Bergstrom K, Kajander EO (1999) Nanobacteria: an infectious cause for kidney stone formation. Kidney Int 56:1893
Ciftcioglu N, Miller-Hjelle MA, Hjelle JT, Kajander EO (2002) Inhibition of nanobacteria by antimicrobial drugs as measured by a modified microdilution method. Antimicrob Agents Chemother 46:2077
Cisar JO, Xu D-Q, Thompson J, Swaim W, Hu L, Kopecko DJ (2000) An alternative interpretation of nanobacteria-induced biomineralization. Proc Natl Acad Sci U S A 97:11511
Fan J, Chandhoke PS (1999) Examination of crystalluria in freshly voided urines of recurrent calcium stone formers and normal individuals using a new filter technique. J Urol 161:1685
Folk RL (1993) SEM imaging of bacteria and nannobacteria in carbonate sediments and rocks. J Sediment Petrol 63:990
Garcia Cuerpo E, Kajander EO, Ciftcioglu N, Lovaco Castellano F, Correa C, Gonzalez J, Mampaso F, Liano F, Garcia de Gabiola E, Escudero Barrileiro A (2000): Nanobacteria. Un modelo de neo-litogenesis experimental. Arch Esp Urol 53:291
Hjelle JT, Miller-Hjelle MA, Poxton IR, Kajander EO, Ciftcioglu N, Jones ML, Caughey RC, Brown R, Millikin PD, Darras FS (2000) Endotoxin and nanobacteria in polycystic kidney disease. Kidney Int 57:2360
Hojgaard I, Fornander AM, Nilsson MA, Tiselius HG (1999) Crystallization during volume reduction of solutions with a composition corresponding to that in the collecting duct: the influence of hydroxyapatite seed crystals and urinary macromolecules. Urol Res 27:417
Holmberg M (2002) Serological evidence for nanobacteria prevalence suggests a possible zoonosis. In: International Nanobacteria Minisymposium, March 8 2001, Kuopio. Book of abstracts, Kuopio University Press, Kuopio, (in press). Abstract at http://www.nanobac.com/nbminisymp080301/page10.html
Kajander EO, Ciftcioglu N (1998) Nanobacteria: an alternative mechanism for pathogenic intra- and extracellular calcification and stone formation. Proc Natl Acad Sci U S A 95:8274
Kajander EO, Ciftcioglu N (2000) Nanobacteria as extremophiles. Proc SPIE Int Soc Opt Eng 3755:106
Kajander EO, Kuronen I, Akerman K, Pelttari A, Ciftcioglu N (1997) Nanobacteria from blood, the smallest culturable autonomously replicating agent on Earth. Proc SPIE Int Soc Opt Eng 3111:420
Kajander EO, Bjorklund M, Ciftcioglu N (1998) Mineralization by nanobacteria. Proc SPIE Int Soc Opt Eng 3441:86
Kajander EO, Heinonen T, Kuronen I, Luoto K, Ciftcioglu N (1999) Nanobacteria, mycoplasma and bacterial L-forms; problems for sterile filtration. In: Wirtanen G, Salo S, Mikkola A (eds) 30th R3-Nordic Contamination Control Symposium, Helsinki, Finland, May 30–June 2, 1999. VTT Technical Research Centre of Finland, Espoo, p 279
Kajander EO, Ciftcioglu N, Aho K (2001) Detection of nanobacteria in viral vaccines. Proceedings of the American Society of Microbiology, 101stGeneral Meeting, 20–24 May 2001, Orlando. Abstract Y-3, p 736.
Kajander EO, Ciftcioglu N, Miller-Hjelle MA, Hjelle JT (2001) Nanobacteria: controversial pathogens in nephrolithiasis and polycystic kidney disease. Curr Opin Neprol Hypertens 10:445
Lieske JC, Toback FG (2000) Renal cell-urinary crystal interactions. Curr Opin Neprol Hypertens 9:349
Low RK, Stoller ML, Schreiber CK (2000) Metabolic and urinary risk factors associated with Randall's papillary plaques. J Endourol 14:507
Martini LA, Wood RJ (2000) Should dietary calcium and protein be restricted in patients with nephrolithiasis? Nutr Rev 58:111
McKay DS, Gibson EKJr, Thomas-Keprta KL, Vali H, Romanek CS, Clemett SJ, Chillier XD, Maechling CR, Zare RN (1996) Search for past life on Mars: Possible relic biogenic activity in Martian meteorite ALH840001. Science 273:924
Miller-Hjelle MA, Hjelle JT, Ciftcioglu N, Kajander EO (2003). Nanobacteria: methods for growth and identification of this recently discovered calciferous microbe. In: Olson W (ed) Rapid analytical microbiology: the chemistry and physics of microbial identification. Sue Horwood, Storrington (in press)
Price PA, Buckley JR, Williamson MK (2001) The amino bisphosphonate ibandronate prevents vitamin D toxicity and inhibits vitamin D-induced calcification of arteries, cartilage, lungs and kidneys in rats. J Nutr 131:2910
Price PA, Faus SA, Williamson MK (2001) Bisphosphonates alendronate and ibandronate inhibit artery calcification at doses comparable to those that inhibit bone resorption. Arterioscler Thromb Vasc Biol 21:817
Price PA, Thomas GR, Pardini AW, Figueira WF, Caputo JM, Williamson MK (2002) Discovery of a high molecular weight complex of calcium, phosphate, fetuin, and matrix γ-carboxyglutamic acid protein in the serum of etidronate-treated rats. J Biol Chem 277:3926
Price PA, Omid N, Than TN, Williamson MK (2002) The amino bisphosphonate ibandronate prevents calciphylaxis in the rat at doses that inhibit bone resorption. Calcif Tissue Int 71:356
Puskás L (2002) Detection of nanobacteria in human atherosclerotic plaques. In: International Nanobacteria Minisymposium, March 8 2001, Kuopio. Book of abstracts, Kuopio University Press, Kuopio, (in press). Abstract at http://www.nanobac.com/nbminisymp080301/page13.html
Ramello A, Vitale C, Marangella M (2000) Epidemiology of nephrolithiasis. J Nephrol 13:S45
Randall A (1937) The origin and growth of renal calculi. Ann Surg 105:1009
Scheinmann SJ (1999) Nephrolithiasis. Semin Nephrol 19:381
Schwartz BF, Bruce J, Leslie S, Stoller ML (2001) Rethinking the role of urinary magnesium in calcium urolithiasis. J Endourol 15:233
Sidhu H, Schmidt ME, Cornelius JG, Thamilselvan S, Khan SR, Hesse A, Peck AB (1999) Direct correlation between hyperoxaluria/oxalate stone disease and the absence of the gastrointestinal tract-dwelling bacterium Oxalobacter formigenes: possible prevention by gut recolonization or enzyme replacement therapy. J Am Soc Nephrol 10 (Suppl 14):S334
Sommer AP, Pinheiro AL, Mester AR, Franke RP, Whelan HT (2001) Biostimulatory windows in low-intensity laser activation: lasers, scanners and NASA's light-emitting diode array system. J Clin Laser Med Surg 19:29
Sommer AP, Hassinen HI, Kajander EO (2002) Light induced replication of nanobacteria-a preliminary report. J Clin Laser Med Surg 20:241
Sommer AP, Oron U, Kajander EO, Mester AR (2002) Stressed cells survive better with light. J Proteome Res 1:475
Söhnel O, Grases F (1993) Fine structure of calcium oxalate monohydrate renal calculi. Nephron 63:176
Uwins PJR, Webb RI, Taylor AP (1998) Novel nano-organisms from Australian sandstones. Am Minerol 83:1541
Vali H, McKee MD, Ciftcioglu N, Sears SK, Plows FL, Chevet E, Ghiasi P, Plavsic M, Kajander EO, Zare RN (2001) Nanoforms: a new type of protein-associated mineralization. Geochim Cosmochim Acta 65:63
Wahl C, Hess B (2000) Kidney calculi – is nutrition a trigger or treatment? Ther Umsch 57:138
Wainwright M (1999) Nanobacteria and associated 'elementary bodies' in human disease and cancer. Microbiology 145:2623
Ylitalo R (2002) Bisphosphonates and atherosclerosis. Gen Pharmacol 35:287
Acknowledgments
This study was supported by grants from the Sigrid Juselius Foundation, TEKES and the Research Council for Biosciences and Environment, Finnish Academy.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kajander, E.O., Ciftcioglu, N., Aho, K. et al. Characteristics of nanobacteria and their possible role in stone formation. Urol Res 31, 47–54 (2003). https://doi.org/10.1007/s00240-003-0304-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-003-0304-7