
Abstract
Objective
The quality of medication use by the elderly is a major safety concern because of an increasing number of people in this segment of the population and the fact that they are major drug consumers. The objective of this study was to test whether administrative computerized pharmacy prescription data could be used to assess the prevalence of potentially inappropriate medication use by the elderly in Rijeka, Croatia, using two sets of explicit criteria data.
Methods
In 2002, the prevalence of potentially inappropriate medication use in the elderly aged 70 years or over was evaluated using Beers’ criteria. Inappropriate co-prescribing was evaluated using a list of eight potentially harmful drug combinations. Information on the use of drugs was collected from a computerized pharmacy record of all prescriptions dispensed in the “Jadran Pharmacies” in Rijeka.
Results
Five computerized pharmacies dispensed 306,000 (65% of all prescriptions in Rijeka); 78,000 were for those aged 70 years and over. Among these elderly, the prevalence of inappropriate choice of drugs was 2.2% and inadequate co-prescribing 1.9%. The most common inappropriate drug was a long-acting benzodiazepine, diazepam. Mostly used potentially harmful combinations were a non-steroidal anti-inflammatory drug (NSAID) co-prescribed with a diuretic, and two benzodiazepines co-prescribed.
Conclusion
We found that computerized pharmacy data can be used as a screening tool in efforts to improve the quality of drug prescribing in Rijeka. Explicit criteria for assessing inappropriate prescribing for the elderly can easily be applied to population based surveys. This study suggests a low rate of potentially inappropriate prescribing for the elderly in Rijeka.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Drug Utilization and Quality of Care was the title of a WHO Drug Utilization Research Group meeting in Oxford in 1993. With the recent sociopolitical changes in Europe, a number of newly formed European countries took part, some of which needed to draft new drug policies, drug control and drug surveillance programs. The meeting illustrated important methodological issues of measuring and evaluating the outcome of prescribing [1]. Croatia (4.5 million inhabitants) is one such country that has adopted various methods to make the use of drugs more rational. We report on how existing pharmacy data and modern technology can be used as a screening tool in detecting and improving drug use for individual patients.
Inappropriate medication use is a major safety concern especially for the elderly because of an increasing number of people in this segment of the population and the fact that they are the major drug consumers. The aging process increases the risk of drug-related problems, mainly because of impaired renal and liver function, increased body fat and changes in the receptor sensitivity. Furthermore, drug-related illnesses are seldom recognized as such and are often mistaken by a new illness or, even worse, interpreted as aging itself [2]. Because medication use plays a central role in geriatric practice, a systematic surveillance of the quality of drug use in the elderly is essential.
The objective of this study was to examine whether administrative computerized pharmacy prescription data could be used to assess the prevalence of potentially inappropriate medication use in the elderly in Rijeka (170,000 inhabitants), Croatia, based on two sets of explicit criteria.
Methods
Information on the use of drugs was collected from a computerized pharmacy record of all prescriptions dispensed in the “Jadran Pharmacies”, which consists of five major pharmacies in the city of Rijeka. This population-based database is up to date and provides information about prescribed drugs (substance, brand and formulation; using the ATC classification [3]), amount, dose, date of prescription, physician code and patient identification number. In Croatia, only primary-care physicians can prescribe drugs that will be reimbursed.
The prevalence of potentially inappropriate medication in the elderly aged 70 years or over was evaluated using Beers’ citeria in the year 2002 [4]. These criteria define medications that should generally be avoided in the ambulatory elderly. Only drugs available for outpatient use in Croatia were included (Table 1). Potentially inappropriate co-prescribing to the elderly, during January 2002, was evaluated using a list of eight potentially harmful drug combinations (Table 2). The authors have agreed upon these eight inappropriate drug combinations as mostly cited in the literature, taking into account only the drugs available in Croatia.
Results
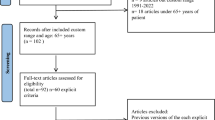
In 2002, the five computerized pharmacies dispensed 305,874 prescriptions. These corresponded with 65% of all prescriptions dispensed in Rijeka. Of these prescriptions analyzed, 78,091 (25.5%) were prescribed to patients aged 70 years and over. On average, there were 7.5 prescriptions per patient in this age group in the year 2002. The most commonly prescribed drugs were cardiovascular drugs (ATC group C) with 41%, followed by drugs affecting the nervous system (group N) with 15%.
According to Beers’ criteria, 1677 prescriptions (2.2%) were for drugs that were inappropriate for use by the elderly. The most commonly prescribed drug was diazepam (Table 1).
In January, 4848 prescriptions were dispensed to the elderly in the “Jadran Pharmacies”. Potentially harmful drug combinations were issued to 40 of 2114 patients (1.9%) (Table 2). Among the eight drug combinations examined, the most common was a combination of an NSAID with a diuretic.
Discussion
This study was the first attempt to assess the quality of drug prescribing in the elderly in Croatia, using explicit criteria by analyzing pharmacy record on prescription data. We found that computerized pharmacy data could also be used in Rijeka as a screening tool in efforts to improve the quality of drug prescribing [5]. General practice offices’ data on drug prescribing as well as individual patient records were not available for the survey. Therefore, our estimates may represent only a fraction of inappropriate prescribing for the elderly in Rijeka. Other limitations of the study are the lack of assessment of indicators for which the drugs were prescribed, the data on dosages and duration of treatments, the data on prevalence of adverse drug reactions as well as other drug-related problems.
It should be emphasized that explicit criteria for assessment of inappropriate drug prescribing to the elderly were used as a screening tool for defining potential problem areas.
The five computerized pharmacies enabling this study covered 65% of all prescriptions dispensed in Rijeka. This means that our findings are based on the bulk of the person-linked prescriptions. There are no reasons why patients with the remaining 35% of the prescriptions should present a different pattern of potential inappropriate prescribing.
It has been shown that inappropriate drug therapy is an important risk factor for drug-related illnesses among the elderly [6]. Various criteria have been developed to determine the appropriateness of drug use by the elderly. Some of them identify medications, doses, or drug combinations that should not be used by the elderly and can be assessed examining only drug usage data, while others take into account the indication in conjunction with other clinical factors and thus require access to medical records. The most widely used set of explicit criteria for inappropriate prescribing to elderly people was developed by Beers and collaborators [4].
The most common inappropriate drug prescribed was a long-acting benzodiazepine, diazepam (56% of all inappropriate drugs, with an overall prevalence of 1.2%), followed by diphenhydramine and amitriptyline. This finding is in accordance with a review of published studies that have been using Beers’ criteria for inappropriate medication use by the elderly in various settings [6, 7]. In these studies, the most common inappropriate medications were long-acting benzodiazepines, dipyridamole, propoxyphene and amitriptyline. At the time of the study, dipyridamole and propoxyphene were not available as prescription drugs in Croatia. Diphenhydramine is appropriate for treatment of allergic reactions and urticaria, but not sedation [8]. However, without access to a patients’ medical record it is difficult to assess what the indication was for diphenhydramine in our study population. Long-acting benzodiazepines such as diazepam should be avoided for the elderly because of the associations with daytime sedation and the risk of falls and fractures [9].
It has been suggested that a program to decrease inappropriate prescribing should focus on the most commonly prescribed inappropriate medications. Programs may include professional education and formulary management [6]. The Beers’ criteria have helped create a consistent and explicit measure of inappropriate medication use in the elderly in different health-care settings.
Among the potential harmful drug combinations (Table 2) all drug interactions were classified as being clinically important [10]. The most common combinations were NSAIDs co-prescribed with a diuretic, and two benzodiazepines co-prescribed, one as a tranquilizer and the other as a hypnotic. NSAIDs should be used with caution in patients with a history of cardiovascular disease. The risk of NSAID-related congestive heart failure might even exceed the risk of NSAID-related gastrointestinal bleeding [11]. The combination of two benzodiazepines may result in over-sedation, impaired cognition, confusion, dependence and increased risk of falls and fractures [12]. Published studies that assess appropriateness of drug prescribing for the elderly vary considerably in setting, scope, sample size, study design, data source and data collection period, so our results could not be fully compared with other similar surveys.
Focusing on drug use in the elderly, our study concerns a significant and increasing part of the population in many countries. In Croatia, we found that those of 70 years and over consumed more than one quarter of all prescription drugs. In the USA those of 65 years and over made up 14% of the population but consumed over 30% of all prescription drugs [2]. In Sweden, this was even more pronounced as those of 70 years and over correspondingly consumed 30% [13]. These figures may reflect different reimbursement systems, but also different ranges of drugs available on the market. In Croatia, there were about 2300 brands (formulations) while in Sweden there were 7000.
Taking into account all the limitations, our data suggests a low rate of inappropriate prescribing to the elderly in Rijeka. This may be explained by a comparatively limited number of prescriptions. We found 7.5 prescriptions per patient to those 70 years and older in Croatia. In Sweden, those 70 years and older received on average 21 prescriptions per inhabitant (and even more per patient; data not available, however, due to confidentiality legislation). In addition, in Croatia, a prescription generally corresponds to a maximum of two packages of 30 tablets, while in Sweden a prescription may correspond to 90 days treatment (on average 68 DDDs, defined daily doses to those 70 years and older [3]). Thus, the potential for inappropriate prescribing seems to be much lower in Croatia than in Sweden.
Results of this study have indicated areas that should probably be targeted in future audits of drug prescribing for the elderly: a significant part of inappropriate use was linked to benzodiazepines and NSAIDs.
Future studies are needed to assess other types of inappropriate medication use, such as extended drug–drug and drug–disease interaction, and should move beyond simple descriptions of prescribing patterns and measure the adverse clinical and financial consequences of poor pharmacotherapeutic decision making for the elderly [8].
It may be concluded that explicit criteria for assessing the prescription of inappropriate drugs or drug combinations for the elderly can easily be applied to population-based surveys to identify areas for quality improvement. Such quality indicators may help identify potential problems that may require further investigation and should enable targeted interventions to influence future prescribing practices. They could also be used to quantify the impact of interventions.
The most successful strategies for improvement of prescribing quality seem to be multifaceted approaches, e.g., educational outreach visits combined with feedback on prescribing patterns [14, 15]. One of the challenges for clinical pharmacology is to provide feedback to practicing physicians with clear and evidence-based alternatives or guidelines. We have recently found that physicians in Rijeka generally have a positive attitude to receiving such feedback on their prescription practices [16].
Future audits should include data on indications for prescribed drugs that are available from the same database. Similar international comparisons are most welcome in order to put our results in perspective.
References
Bergman U, Herxheimer U (1993) Drug utilisation research in Europe. Lancet 342:167
Knight EL, Avorn J (2001) Quality indicators for appropriate medication use in vulnerble elders. Ann Intern Med 135:703–710
WHO (2002) Guidelines for ATC classification and DDD assignment. WHO Collaborating Centre for Drug Statistics Methodology, Oslo
Beers M (1997) Explicit criteria for determining potentially inappropriate medication use by the elderly: an update. Arch Intern Med 157:1531–1536
Strom BL (ed) (2000) Pharmacoepidemiology 3rd edn. John Wiley & Sons, Ltd, Chichester, New York
Aparasu RR, Mort JR (2000) Inappropriate prescribing for the elderly: Beers criteria based review. Ann Pharmcother 34:338–345
Laurier C, Moride Y, Kennedy WA (2002) Health survey data on potentially inappropriate geriatric drug use. Ann Pharmacother 36:404–409
Zhan C, Sangl J, Bierman AS, Miller MR, Friedman, Wickizer SW, Meyer GS (2001) Potentially inappropriate medication use in the community-dwelling elderly. Findings from the 1996 Medical Expenditure Panel Survey. JAMA 286:2823–2829
Straand J, Rokstad KS (1999) Elderly patients in general practice: diagnoses, drugs and inappropriate prescriptions. A report from the Møre & Romsdal Prescription Study. Fam Pract 16:380–388
Sjöqvist F (1997) A new classification system for drug interactions. Eur J Clin Pharmacol 52[Suppl]:A126
Page J, Henry D (2000) Consumption of NSAIDs and the development of congestive heart failure in elderly patients: an unrecognized public health problem. Arch Int Med 160:777–784
McLeod PJ, Huang AR, Tamblyn RM, Gayton DC (1997) Defining inappropriate practices in prescribing for elderly people: a national consensus panel. Can Med Assoc J 156:385–391
Svensk Läkemedelsstatistik 2000 (2000) Apoteket AB, Stockholm (Swedish Drug Statistics 2000, National Corporation of Swedish Pharmacies)
Thomson O’Brian MA, Oxman AD, Davis DA, Haynes RB, Freemantle N, Harvey EL (2001) Audit and feedback: effects on professional practice and health care outcomes (Cochrane Review). In: The Cochrane Library, Issue 4, Update Software, Oxford
Figueiras A, Sastre I, Gestal-Otero J (2001) Effectiveness of educational interventions on the improvement of drug prescription in primary care: a critical literature review. J Eval Clin Pract 7:223–241
Vlahović-Palčevski V, Wettermark B, Prpić I, Bergman U (2004) Attitudes to feedback with drug utilisation 90% (DU90%) profiles among prescribers in Rijeka, Croatia. Pharmacoepidemiol Drug Safety (in press)
Acknowledgements
We thank Silvana Jager, MSc Pharm, for providing anonymous prescription data. We acknowledge the Swedish Institute for a scholarship and Pharmacia Corp. for an unrestricted grant to Vera Vlahović-Palčevski.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vlahović-Palčevski, V., Bergman, U. Quality of prescribing for the elderly in Croatia—computerized pharmacy data can be used to screen for potentially inappropriate prescribing. Eur J Clin Pharmacol 60, 217–220 (2004). https://doi.org/10.1007/s00228-004-0747-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-004-0747-y