
Abstract
The isoprenoids farnesyl pyrophosphate (FPP) and geranylgeranyl pyrophosphate (GGPP) are pivotal intermediates for cholesterol homeostasis and cell signaling in the mevalonate pathway. We developed a sensitive and selective high-performance liquid chromatography tandem triple quadrupole mass spectrometry (LC-QQQ-MS) method for FPP in human plasma without the need for a derivatization process. We optimized the sample preparation procedure to extract FPP and 13C5-FPP (as internal standard) from sample fluids using methanol. Phosphate-buffered saline was used as the surrogate matrix for the preparation of calibration curves and quality control samples. Using an XBridge C18 column (3.5 μm, 2.1 × 100-mm ID) with gradient elution composed of 10 mmol/L ammonium carbonate/ammonium hydroxide (1000:5, v/v) and acetonitrile/ammonium hydroxide (1000:5, v/v) provided the sharp peaks of FPP and 13C5-FPP in human plasma. The calibration curve ranged from 0.2 to 20 ng/mL in human plasma with acceptable intra-day and inter-day precision and accuracy. The sensitivity of this bioanalytical method was sufficient for clinical analysis. The endogenous FPP plasma concentrations in 40 human healthy volunteers ascertained by LC-QQQ-MS and high-performance liquid chromatography tandem hybrid quadrupole Orbitrap high-resolution mass spectrometry (LC-Q-Orbi-MS) were comparable. Furthermore, the endogenous GGPP in human plasma was selectively detected for the first time by LC-Q-Orbi-MS. In conclusion, a sensitive bioanalytical method for FPP in human plasma by means of LC-QQQ-MS and LC-Q-Orbi-MS was developed in this study. Taking into account the versatility of LC-Q-Orbi-MS, the simultaneous detection of FPP and GGPP may be feasible in clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Farnesyl pyrophosphate (FPP) is one of the isoprenoid intermediates in the mevalonate pathway which contributes to cholesterol homeostasis, signal transduction, and cell proliferation [1]. FPP is also reported as a precursor for sterols, dolichols, geranylgeranyl pyrophosphate (GGPP), and ubiquinone [1]. Furthermore, the clinical importance of FPP has been extensively demonstrated for several diseases, such as hyperlipidemia [2], osteoclast-mediated bone resorption [3], neurodegenerative diseases [4–6], and cancers [7–9], because FPP plays a role as central branching points in the mevalonate pathway [2]. Therefore, the FPP concentrations in plasma and relevant tissues may be of great interest to monitor pathological conditions and modulation with therapeutic intervention.
Until now, there have been several bioanalytical methods to determine FPP concentrations in human biological samples [10]. High-performance liquid chromatography (HPLC) using fluorescent derivative with 9-anthroylcyanide for farnesol after cleavage of the pyrophosphate group of FPP enabled the determination of FPP in human plasma as 6.6 ± 0.5 ng/mL [11]. Hooff et al. reported that HPLC with fluorometric detection method using dansyl-labeled pentapeptides allowed the determination of FPP in human brain tissue over a linear calibration range of 10–400 ng/mL [12]. Besides that, an HPLC tandem triple quadrupole mass spectrometry with electrospray ionization (LC-QQQ-MS) method to detect dansyl-labeled pentapeptide FPP was developed with a calibration curve ranging from 5 to 250 ng/mL in human brain tissue [13]. Henneman et al. firstly proposed the direct analysis of FPP in HepG2 cells by means of LC-QQQ-MS in the negative ion mode [14, 15]. The detection limit of this bioanalytical method was approximately 10 ng/mL [14]. To the best of our knowledge, the currently available bioanalytical methods have insufficient sensitivity to accurately determine endogenous FPP in human plasma and are labor-intensive due to the requirement of a derivatization procedure followed by a dephosphorylation procedure in sample pretreatment. Therefore, a highly sensitive and simple bioanalytical method for determining FPP in human plasma will be required.
Recent advances in high-resolution accurate mass spectrometry (HRMS) have allowed performing sensitive and selective quantitative analyses using high-resolution full scan or product ion scan acquisition with precursor isolation [16–20]. In HPLC coupled to HRMS analysis, the quantification can be performed with the construction of an extracted ion chromatogram using a narrow mass extraction window centered on the analyte theoretical m/z. A number of head-to-head sensitivity comparisons between LC-QQQ-MS and HPLC tandem hybrid quadrupole Orbitrap high-resolution mass spectrometry (LC-Q-Orbi-MS) or HPLC tandem quadrupole time-of-flight mass spectrometry using high-resolution full scan or product ion scan acquisition mode have been reported for small molecule compounds [19, 21, 22], biomarkers [17, 23], and protein therapeutics [24–26] in human biological samples. Enhanced resolution can improve the selectivity of the assay; especially, co-eluting isobaric interference can more easily be distinguished from the analyte peak [27]. Thus, the use of HRMS may increase the signal-to-noise ratio and overall sensitivity in biological samples.
This work presents the development of a highly sensitive and reliable bioanalytical method for FPP plasma concentrations in humans and its application for the determination of FPP plasma in male and female human volunteers without derivatization using LC-QQQ-MS. We also discuss the application of HRMS for the quantification of mevalonate-derived isoprenoid intermediates, including FPP and GGPP, in human plasma.
Materials and methods
Chemicals and reagents
The reference standards of farnesyl pyrophosphate (FPP; farnesyl diphosphate, purity ≥95%, tris-ammonium salt) and geranylgeranyl pyrophosphate (GGPP; geranylgeranyl diphosphate, purity ≥95%, tris-ammonium salt) were purchased from Echelon Biosciences (Salt Lake City, UT, USA). 13C-labeled FPP (13C5-FPP, triethylamine salt) was from NARD Institute (Kobe, Japan). Untreated human plasma samples containing K2EDTA as an anticoagulant from volunteers were from Nippon Bio-Support Center (Tokyo, Japan) and Bioreclamation (Westbury, NY, USA). Ammonium hydroxide (25% ammonia solution) was from Wako Pure Chemicals Industries (Osaka, Japan). Dulbecco’s phosphate-buffered saline (PBS) was from DS Pharma Biomedical (Osaka, Japan). All the other chemicals, reagents, and solvents were of analytical grade.
Preparation of stock solution, calibration standards, QC, and IS samples
The stock solutions for the free acids of FPP, GGPP, and 13C5-FPP as internal standard (IS) were prepared in 50% methanol at a concentration of 200 μg/mL. The stock solutions of FPP and GGPP were mixed and serially diluted with 50% methanol to prepare the working standard solutions. The working IS solutions were prepared at 10 ng/mL. All solutions were stored in polypropylene tubes at 4 °C. The calibration standards in the surrogate matrix (PBS) were prepared at the final concentrations of 0.2, 0.4, 0.8, 2, 4, 8, and 20 ng/mL. The final concentrations of FPP for quality control (QC) samples in PBS were 0.2 (lower limit of quantification, LLOQ), 0.6 (low-QC, LQC), 3 (medium-QC, MQC), and 16 ng/mL (high-QC, HQC). To confirm how well a set of calibration standards in the surrogate matrix track the response of the authentic analyte in the biological matrix (parallelism) [28], unspiked and spiked QC samples in human plasma were also analyzed. The spiked QC samples in human plasma were prepared with an additional FPP solution corresponding to 0.6, 3, and 16 ng/mL. All QC samples in PBS and human plasma were stored in polypropylene tubes at −30 °C until use.
Instrumentation and conditions for LC-MS/MS analysis
The LC-MS/MS consisted of a Nexera ultra high-performance liquid chromatograph system (UHPLC; Shimadzu, Kyoto, Japan) and a hybrid triple quadrupole linear ion trap mass spectrometer QTRAP® 5500 system (LC-QQQ-MS; Sciex, Redwood City, CA, USA) or a high-performance liquid chromatograph system (Dionex UltiMate 3000; Thermo Fisher Scientific, San Jose, CA, USA) and a hybrid quadrupole Orbitrap high-resolution mass spectrometry (LC-Q-Orbi-MS; Q-Exactive plus, Thermo Fisher Scientific). C18 analytical column XBridge (3.5 μm, 2.1 × 100-mm ID; Waters, Milford, MA, USA) equipped with an L-column pre-column filter (Chemicals Evaluation and Research Institute, Tokyo, Japan) was used at 30 °C. The mobile phases were composed of (A) 10 mmol/L ammonium carbonate/ammonium hydroxide (25% ammonia solution) (1000:5, v/v) and (B) acetonitrile/ammonium hydroxide (1000:5, v/v), respectively. The stepwise gradient program used was as follows: 0–10.0 min, B 10–90%; 10.0–12.0 min, B 90%; 12.0–12.1 min, B 90–10%; and 12.1–15.0 min, B 10%. The flow rate of the mobile phase was 0.3 mL/min.
On the LC-QQQ-MS, each precursor and product ion pair transition was selected for multiple reaction monitoring (MRM) with a 100-ms dwell time. The ionization mode was electrospray ionization (ESI) in negative ion mode and the source temperature was set at 600 °C. A nitrogen curtain gas, ion source gas 1, ion source gas 2, and ion source voltage were set at 20, 65, and 65 psi and at −4000 V, respectively. Mass spectrometric data were acquired and processed using the software Analyst version 1.5.2 (Sciex). The optimized mass spectrometric parameters of FPP, GGPP, and 13C5-FPP for LC-QQQ-MS are summarized in Table 1.
High-resolution mass spectrometry full scan analysis was performed in multiple targeted selected ion monitoring (t-SIM) mode by LC-Q-Orbi-MS. The ionization mode was ESI in negative ion mode and the source temperature was set at 450 °C. The ion source spray voltage, ion transfer tube temperature, sheath, auxiliary nitrogen flow rate, automatic gain control, and resolution were set at 3000 V, 275 °C, 40 arbitrary units, 10 arbitrary units, 1 × 105 ions, and 140,000 (at m/z 200), respectively. Extracted ion chromatograms were based on ±5 ppm of mass extraction window centered on the theoretical m/z for FPP (381.1241), GGPP (449.1867), and 13C5-FPP (386.1407), respectively. Mass spectrometric data were acquired and processed using Xcalibur software (Thermo Fisher Scientific).
Sample preparation
A preliminary investigation of sample pretreatment for FPP determination in surrogate matrix and human plasma was conducted using several procedures for solid phase extraction (SPE) and protein precipitation (PP). The recovery of FPP spiked in PBS and human plasma was evaluated. FPP in the surrogate matrix and human plasma (100 μL) spiked with FPP at a level of 10 ng/mL was loaded into Oasis® HLB (30 mg/1 cm3, Waters), Oasis® WAX (30 mg/1 cm3, Waters), and Monospin® Phospholipid (GL Sciences, Tokyo, Japan) cartridges, which were pre-conditioned with 1 mL of methanol and each aqueous solution such as 10 mmol/L ammonium acetate, 2% formic acid, and 0.1% trifluoroacetic acid, respectively. Hydrophilic compounds were washed out by 1 mL of 10 mmol/L ammonium acetate, 2% formic acid, and 0.1% trifluoroacetic acid, respectively, and then FPP was eluted using 1 mL of methanol or methanol containing ammonium hydroxide, as summarized in Table 2. The centrifugation condition was at 185×g set at 4 °C for 2 min. Furthermore, extraction of FPP in the surrogate matrix and human plasma additionally spiked with FPP at a level of 10 ng/mL was also performed by PP. FPP in the surrogate matrix and human plasma (100 μL) spiked with FPP was extracted by adding 500 μL of the extract solvent such as acetonitrile, methanol, butanol/75 mmol/L ammonium hydroxide/ethanol (1:1.25:2.75, v/v/v) and 2-propanol/100 mmol/L ammonium hydrogen carbonate/acetonitrile (1:1:2, v/v/v). The sample was mixed for deproteinization and centrifuged at 1662×g set at 4 °C for 20 min. The eluate was evaporated to dryness under a stream of nitrogen gas at room temperature. The residue was reconstituted in 200 μL of 50% methanol and filtered with a centrifugal filter unit (Merck, Darmstadt, Germany) with a pore size of 0.45 μm at 9600×g set at 4 °C for 1 min. After the addition of 13C5-FPP (100 ng/mL, 5 μL), 20-μL aliquots of the resulting solution were injected into the LC-MS/MS.
For the method qualification study, the optimized sample pretreatment procedure was employed as follows. A 500-μL aliquot of human plasma or PBS was mixed with 50 μL of 10 ng/mL 13C5-FPP and 2500 μL of methanol. The supernatant after centrifugation at 1662×g set at 4 °C for 20 min was evaporated to dryness under a stream of nitrogen gas at room temperature. The residue was dissolved again in 100 μL of 50% methanol and then filtered with a centrifugal Ultrafree® MC HV filter unit at 9600×g set at 4 °C for 1 min; the filtered solution (20 μL) was injected into the LC-MS/MS.
Bioanalytical assay performance
The methodological assay performance was evaluated based on the general principles in the FDA Guidance for Industry regarding bioanalytical method validation [29]. Specific issues for the method qualification of endogenous compounds in the biological matrix were also addressed according to previous work [30–32]. Briefly, a linear model fitted by least-squares linear regression with weighting factor 1/x 2 was used to describe the calibration curve based on the area ratios of FPP to 13C5-FPP versus the nominal concentrations of the analyte. The criterion of the relative error (%RE) of the back-calculated concentrations to the nominal concentrations was set as within ±15% of nominal values (for LLOQ, ±20%). The precision and accuracy were assessed at four concentrations in five replicates in surrogate matrix (LLOQ, LQC, MQC, and HQC) and human plasma (unspiked, additionally LQC, MQC, and HQC spiked plasma) in three analytical runs. Intra- and inter-day precision was calculated by the coefficient of variation (%CV) and accuracy was calculated by %RE. Each acceptance criterion was set within 15% of the %CV (for LLOQ, 20%) and within ±15% of the %RE (for LLOQ, ±20%). Matrix variability was assessed by a matrix factor (MF) using six different lots of human plasma spiked with FPP at a level of 3 ng/mL. The MF was calculated by the following equations, where the peak area of the sample for matrix effect was determined by human plasma spiked with FPP standard solution at a level of 3 ng/mL in the processed sample and the peak area of the sample for reference was determined by standard solution at the concentration of the endogenous level plus 3 ng/mL of FPP in 50% methanol solution.
The analyte stability in stock solution was evaluated after storage at 4 °C by comparing the freshly prepared stock solutions. The stability tests of FPP in human plasma (blank plasma and plasma spiked with 3 ng/mL of FPP) were conducted after three freeze/thaw cycles. The stability in the post-preparation for 2 days in the autosampler (set at 10 °C) and in a freezer set at −30 °C for 33 days was also investigated. Stability was evaluated as the difference from the initial peak area ratio. The acceptance criteria were set within 100 ± 15% of that remaining.
Results and discussion
The present work describes several important elements to successfully determine endogenous FPP in human plasma by LC-MS/MS, such as the selection of precursor and product ions, optimization of the sample pretreatment procedure, and the chromatographic conditions for the direct analysis of FPP. The structure of mevalonate-derived isoprenoids (i.e., FPP and GGPP) solely consisting of isoprene units and a pyrophosphate moiety indicates the potential risk of poor ionization efficiency with electrospray ionization mass spectrometry and difficulty in the extraction from biological matrix. In addition, a highly selective bioanalytical assay will always be required to determine the endogenous biomarker in the biological matrix [33].
Selection of precursor and product ions
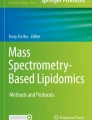
Optimization of the mass spectrometric parameters of FPP, GGPP, and 13C5-FPP using LC-QQQ-MS was conducted in the negative ion mode. The fragment ions at m/z 79 and 159 were formed by elimination of a phosphate or pyrophosphate moiety from FPP, GGPP, and 13C5-FPP. FPP, GGPP, and 13C5-FPP were most abundantly detected at m/z 381.1 > 79, 386.1 > 79, and 449.1 > 79, respectively. The postulated fragmentation is shown in Fig. 1.

Chemical structure and negative product ion spectra for FPP (A), 13C5-FPP (B), and GGPP (C). Asterisk indicates 13C-labeled carbon position
Chromatographic conditions
Although Saisho et al. previously reported the determination of endogenous FPP in human plasma by HPLC with fluorescence detection, this analytical method required a derivatization process with 9-anthroylcyanide after cleavage of the pyrophosphate group of FPP [11]. As described previously, a derivatization method may result in poor qualitative performance and the formation of residual products influenced by complex biological matrices [30–32]. Therefore, we optimized the chromatographic condition to detect FPP in human plasma using a C18 analytical column with the gradient mobile phase comprising 10 mmol/L ammonium carbonate/ammonium hydroxide (25% ammonia solution) (1000:5, v/v) and acetonitrile/ammonium hydroxide (1000:5, v/v) without any derivatization procedure in the negative ion mode. It is worth noting that the mobile phases described in detail in “Materials and methods” should be freshly prepared on the day of sample analysis and the LC-MS/MS should be adequately equilibrated. Otherwise, the FPP chromatographic peak is prone to tailing due to the change of the pH condition of the mobile phases.
Optimization of the sample pretreatment procedure
A preliminary investigation of the sample pretreatment for FPP determination in human plasma was conducted using several procedures for SPE and PP. The recovery of FPP spiked in PBS and human plasma was evaluated. Oasis® HLB was first tested because this cartridge contains a universal polymeric reversed-phase sorbent that can be applied for various types of acidic, basic, and neutral compounds. Oasis® WAX was tested because this cartridge contains weak anion exchange mixed-mode sorbent which is selective for the sample preparation of acidic compounds. Indeed, Van den Eede et al. reported that the recoveries of dialkyl and diaryl phosphates were in the acceptable range from 69 to 119% in pooled human urine [34]. Monospin® phospholipid coated with titanium dioxide and zirconium dioxide was also tested because these metal oxides have been used for the selective enrichment of phospholipids with specific Lewis acid–base interactions [35, 36].
The recovery for FPP was evaluated in comparison with the peak area ratio of FPP to 13C5-FPP for the extracted samples by means of different SPE or PP methods and the unextracted FPP solution. The endogenous concentration of FPP in human plasma was determined in advance with PP using methanol. Extraction of FPP in the surrogate matrix (10 ng/mL) and human plasma additionally spiked with FPP at a level of 10 ng/mL was carried out by SPE, as summarized in Table 2. Furthermore, the recovery of FPP in the surrogate matrix and human plasma additionally spiked with FPP at a level of 10 ng/mL was confirmed by PP. Briefly, FPP in the surrogate matrix and human plasma spiked with FPP was extracted by adding extract solvents such as acetonitrile, methanol, butanol/75 mmol/L ammonium hydroxide/ethanol (1:1.25:2.75, v/v/v) [37] and 2-propanol/100 mmol/L ammonium hydrogen carbonate/acetonitrile (1:1:2, v/v/v) [38]. As indicated in Fig. 2, the recovery of FPP in the surrogate matrix and human plasma by PP with methanol ranging from 71.5 to 86.6% was stable and better than the other sample pretreatment procedures using PP. The recovery of FPP pretreated by Oasis® WAX cartridge ranging from 35.1 to 69.3% was the highest among the SPE procedures; however, the recovery of FPP in the surrogate matrix was relatively low, probably due to adsorption losses to the SPE cartridge and/or polypropylene tube. Therefore, the sample pretreatment with PP using methanol was used in this study.

Recovery of FPP in PBS and human plasma extracted by different SPE and PP methods. Each data point represents the mean ± standard deviation (n = 3)
Method qualification
The use of an authentic analyte as a calibrator in the surrogate matrix is the most common strategy for the quantification of biomarker by LC-MS/MS, especially when only a single stable isotope-labeled analyte is available [28, 39]. The calibration standards were prepared in PBS as the simple surrogate matrix for the quantification of FPP in human plasma. Confirmation of parallelism of the response between the calibration standards in PBS and authentic analyte in human plasma is described in this section.
The calibration curves fitted by least-squares linear regression with 1/x 2 weight on the peak area ratios of FPP to 13C5-FPP were obtained for FPP in the method qualification. The calibration curves of FPP ranged from 0.2 to 2 ng/mL in PBS solution to adequately cover the range of endogenous human plasma concentrations. The correlation coefficients (r) were higher than 0.996. All of the back-calculated concentrations of the calibration standards satisfied the criteria. Representative MRM chromatograms for blank, LLOQ, and ULOQ samples in PBS are shown in Fig. 3A–C. The FPP peak had enough signal-to-noise ratio for quantitation of the LLOQ. The precision and accuracy of the QC samples in PBS at four concentration levels (LLOQ, LQC, MQC, and HQC) and QC samples in human plasma (unspiked and additionally spiked at LQC, MQC, and HQC) were assessed on three different days. The precision (%CV) and accuracy (%RE) in intra- and inter-assays were within 6.1% and within −1.6 to 8.4% of the nominal values, respectively (Table 3). These data demonstrated consistent assay performance across analytical runs and also parallelism by precise and accurate quantification of FPP in spiked QC samples in the surrogate and actual biological matrices. The IS-normalized MF was evaluated for six lots of blank human plasma from male (n = 3) and female (n = 3) volunteers. The IS-normalized MF ranged from 1.21 to 1.42 within the CV of 6.0% (Table 4). These results indicated the robustness of this analytical method for FPP in human plasma and ascertained the suitability of the use of PBS as a surrogate matrix.

Representative MRM chromatograms of FPP and 13C5-FPP in blank sample (A), LLOQ sample (B), ULOQ sample (C), and human plasma sample (D) and representative MRM chromatograms of GGPP and 13C5-FPP in human plasma sample (E)
The stability of FPP in relevant solvents and human plasma was evaluated. The stock solution of FPP (200 μg/mL) was stable in a refrigerator at 4 °C for 4 months. FPP in human plasma (blank plasma and plasma spiked with 3 ng/mL of FPP) was also stable after three freeze/thaw cycles and 33 days in a freezer set at −30 °C.
Determination of FPP plasma concentrations in male and female volunteers by LC-QQQ-MS
The bioanalytical method by LC-QQQ-MS was applied to determine the plasma concentrations of FPP in male (n = 20) and female (n = 20) volunteers. A typical MRM chromatogram of FPP in human plasma is shown in Fig. 3D indicating enough sensitivity and chromatographic separation from interfering peaks for the quantification of FPP in human plasma. However, the selective detection of GGPP was not achieved by LC-QQQ-MS because of the presence of endogenous interfering peaks and relatively high background noise (Fig. 3E). The eluting position of GGPP was confirmed by the additional spike of GGPP solution in human plasma samples. The plasma concentrations of FPP were 1.61 ± 0.40 and 1.49 ± 0.38 ng/mL in male and female volunteers, respectively. The obtained concentrations in this study were a few times lower than the previously published value of 6.6 ± 0.5 ng/mL [11]. Although the specific reason for the difference is still unclear, the published method required a fluorescent derivatization step after cleavage of the pyrophosphate group of FPP. In addition, the baseline was not stable in the previous method, which may have caused the measurement error during the sample pretreatment and data processing.
Application of LC-Q-Orbi-MS for the quantification of mevalonate-derived isoprenoid intermediates, including FPP and GGPP, in human plasma
High-resolution mass spectrometry may improve the sensitivity of the assay because co-eluting isobaric interferences can be removed using narrow mass extraction windows (±5 ppm). The t-SIM mode was performed by LC-Q-Orbi-MS for FPP (m/z 381.1241), 13C5-FPP (m/z 386.1407), and GGPP (m/z 449.1867). Although the targeted MS/MS (parallel reaction monitoring, PRM) mode was also utilized for the detection of FPP and GGPP in human plasma, the selectivity and sensitivity were less than those in the t-SIM mode. The fragment ions in the PRM mode, which were mainly formed by the elimination of a phosphate (m/z 78.9591), are relatively small so that the selectivity and sensitivity may not be increased due to the background noise. Figure 4 indicates typical extracted ion chromatograms for FPP, 13C5-FPP, and GGPP with the t-SIM mode indicating enough sensitivity and selectivity for the simultaneous determination of FPP and GGPP in human plasma. The calibration curve was linear throughout the range from 0.2 to 20 ng/mL for FPP in human plasma with a correlation coefficient (r 2) of 0.9999. The accuracies of the QC samples in PBS at three concentration levels (LQC, MQC, and HQC) and of the spiked QC samples in human plasma samples were within −0.1 to 7.5% of the nominal values. The relationship of the endogenous FPP concentrations in 40 human healthy volunteers ascertained by LC-QQQ-MS and LC-Q-Orbi-MS was described in Fig. 5. These data indicate that FPP concentrations determined by LC-QQQ-MS and LC-Q-Orbi-MS are equivalent. Since the stable isotope-labeled internal standard for GGPP was not available this time and 13C5-FPP was insufficient as an internal standard for GGPP due to the difference in the retention time (Fig. 4), accurate concentrations of GGPP in human plasma were not determined. Assuming that the difference in the peak area ratios of GGPP to 13C5-FPP in the surrogate matrix and human plasma is negligible, the interim concentration of GGPP was less than a low single-digit nanogram per milliliter. The combination of the capability of long precursor sampling times and high-resolution MS full scans with high scan speed by LC-Q-Orbi-MS may provide intensive and also selective detection of FPP and GGPP even in complex biological matrices. To the best of our knowledge, this is the first investigation to provide a bioanalytical method without derivatization for FPP and GGPP in human plasma. Since the current data provided qualitative evaluation for GGPP due to the lack of an appropriate internal standard, further investigation for the determination of GGPP in human plasma using a stable isotope-labeled GGPP will be preferred.

Representative extracted ion chromatograms of FPP (A), 13C5-FPP (B), and GGPP (C) in human plasma sample in targeted selected ion monitoring mode by LC-Q-Orbi-MS

Comparison of FPP plasma concentrations from male (open circle) and female (closed circle) volunteers determined by LC-QQQ-MS and LC-Q-Orbi-MS (n = 20 individual human plasma each)
Conclusions
A highly sensitive, specific, and direct bioanalytical method by LC-QQQ-MS using PBS as a surrogate matrix for the preparation of calibration curves to determine the endogenous level of FPP in human plasma was developed. The calibration curve ranging from 0.2 to 20 ng/mL adequately covered the endogenous level of FPP in human plasma. This bioanalytical method was successfully applied for the determination of FPP in male and female volunteers. Although the selective detection of GGPP using LC-QQQ-MS was not feasible due to the endogenous interfering peaks, application of LC-Q-Orbi-MS with narrow mass extraction windows enabled the simultaneous detection of FPP and GGPP in human plasma. This bioanalytical method may facilitate monitoring mevalonate-derived isoprenoids such as FPP and GGPP in clinical practice.
References
Goldstein JL, Brown MS. Regulation of the mevalonate pathway. Nature. 1990;343(6257):425–30.
Liao JK. Isoprenoids as mediators of the biological effects of statins. J Clin Invest. 2002;110(3):285–8.
Buhaescu I, Izzedine H. Mevalonate pathway: a review of clinical and therapeutical implications. Clin Biochem. 2007;40(9–10):575–84.
Cole SL, Vassar R. Isoprenoids and Alzheimer’s disease: a complex relationship. Neurobiol Dis. 2006;22(2):209–22.
Eckert GP, Hooff GP, Strandjord DM, Igbavboa U, Volmer DA, Muller WE, et al. Regulation of the brain isoprenoids farnesyl- and geranylgeranylpyrophosphate is altered in male Alzheimer patients. Neurobiol Dis. 2009;35(2):251–7.
Fonseca AC, Resende R, Oliveira CR, Pereira CM. Cholesterol and statins in Alzheimer’s disease: current controversies. Exp Neurol. 2010;223(2):282–93.
Chan KK, Oza AM, Siu LL. The statins as anticancer agents. Clin Cancer Res. 2003;9(1):10–9.
Mijimolle N, Velasco J, Dubus P, Guerra C, Weinbaum CA, Casey PJ, et al. Protein farnesyltransferase in embryogenesis, adult homeostasis, and tumor development. Cancer Cell. 2005;7(4):313–24.
Swanson KM, Hohl RJ. Anti-cancer therapy: targeting the mevalonate pathway. Curr Cancer Drug Targets. 2006;6(1):15–37.
Nürenberg G, Volmer DA. The analytical determination of isoprenoid intermediates from the mevalonate pathway. Anal Bioanal Chem. 2012;402(2):671–85.
Saisho Y, Morimoto A, Umeda T. Determination of farnesyl pyrophosphate in dog and human plasma by high-performance liquid chromatography with fluorescence detection. Anal Biochem. 1997;252(1):89–95.
Hooff GP, Volmer DA, Wood WG, Muller WE, Eckert GP. Isoprenoid quantitation in human brain tissue: a validated HPLC-fluorescence detection method for endogenous farnesyl- (FPP) and geranylgeranylpyrophosphate (GGPP). Anal Bioanal Chem. 2008;392(4):673–80.
Hooff GP, Patel N, Wood WG, Muller WE, Eckert GP, Volmer DA. A rapid and sensitive assay for determining human brain levels of farnesyl- (FPP) and geranylgeranylpyrophosphate (GGPP) and transferase activities using UHPLC-MS/MS. Anal Bioanal Chem. 2010;398(4):1801–8.
Henneman L, van Cruchten AG, Denis SW, Amolins MW, Placzek AT, Gibbs RA, et al. Detection of nonsterol isoprenoids by HPLC-MS/MS. Anal Biochem. 2008;383(1):18–24.
Henneman L, van Cruchten AG, Kulik W, Waterham HR. Inhibition of the isoprenoid biosynthesis pathway; detection of intermediates by UPLC-MS/MS. Biochim Biophys Acta. 2011;1811(4):227–33.
Ramanathan R, Jemal M, Ramagiri S, Xia YQ, Humpreys WG, Olah T, et al. It is time for a paradigm shift in drug discovery bioanalysis: from SRM to HRMS. J Mass Spectrom. 2011;46(6):595–601.
Bruce SJ, Rochat B, Beguin A, Pesse B, Guessous I, Boulat O, et al. Analysis and quantification of vitamin D metabolites in serum by ultra-performance liquid chromatography coupled to tandem mass spectrometry and high-resolution mass spectrometry—a method comparison and validation. Rapid Commun Mass Spectrom. 2013;27(1):200–6.
Fedorova G, Randak T, Lindberg RH, Grabic R. Comparison of the quantitative performance of a Q-Exactive high-resolution mass spectrometer with that of a triple quadrupole tandem mass spectrometer for the analysis of illicit drugs in wastewater. Rapid Commun Mass Spectrom. 2013;27(15):1751–62.
Grund B, Marvin L, Rochat B. Quantitative performance of a quadrupole-orbitrap-MS in targeted LC-MS determinations of small molecules. J Pharm Biomed Anal. 2016;124:48–56.
Kaufmann A, Butcher P, Maden K, Walker S, Widmer M. Comprehensive comparison of liquid chromatography selectivity as provided by two types of liquid chromatography detectors (high resolution mass spectrometry and tandem mass spectrometry): “where is the crossover point?”. Anal Chim Acta. 2010;673(1):60–72.
Dahmane E, Boccard J, Csajka C, Rudaz S, Decosterd L, Genin E, et al. Quantitative monitoring of tamoxifen in human plasma extended to 40 metabolites using liquid-chromatography high-resolution mass spectrometry: new investigation capabilities for clinical pharmacology. Anal Bioanal Chem. 2014;406(11):2627–40.
Leis HJ, Fauler G, Windischhofer W. Enantioselective quantitative analysis of amphetamine in human plasma by liquid chromatography/high-resolution mass spectrometry. Anal Bioanal Chem. 2014;406(18):4473–80.
Fung EN, Xia YQ, Aubry AF, Zeng J, Olah T, Jemal M. Full-scan high resolution accurate mass spectrometry (HRMS) in regulated bioanalysis: LC-HRMS for the quantitation of prednisone and prednisolone in human plasma. J Chromatogr B Analyt Technol Biomed Life Sci. 2011;879(27):2919–27.
Plumb RS, Fujimoto G, Mather J, Potts WB, Rainville PD, Ellor NJ, et al. Comparison of the quantification of a therapeutic protein using nominal and accurate mass MS/MS. Bioanalysis. 2012;4(5):605–15.
Morin LP, Mess JN, Garofolo F. Large-molecule quantification: sensitivity and selectivity head-to-head comparison of triple quadrupole with Q-TOF. Bioanalysis. 2013;5(10):1181–93.
Mekhssian K, Mess JN, Garofolo F. Application of high-resolution MS in the quantification of a therapeutic monoclonal antibody in human plasma. Bioanalysis. 2014;6(13):1767–79.
Kellie JF, Kehler JR, Szapacs ME. Application of high-resolution MS for development of peptide and large-molecule drug candidates. Bioanalysis. 2016;8(3):169–77.
Jones BR, Schultz GA, Eckstein JA, Ackermann BL. Surrogate matrix and surrogate analyte approaches for definitive quantitation of endogenous biomolecules. Bioanalysis. 2012;4(19):2343–56.
FDA (2013) Guidance for Industry. Bioanalytical method validation. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Center for Veterinary Medicine (CVM). www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM292362.pdf
Sugimoto H, Kakehi M, Jinno F. Bioanalytical method for the simultaneous determination of d- and l-serine in human plasma by LC/MS/MS. Anal Biochem. 2015;487:38–44.
Sugimoto H, Kakehi M, Jinno F. Method development for the determination of D- and L-isomers of leucine in human plasma by high-performance liquid chromatography tandem mass spectrometry and its application to animal plasma samples. Anal Bioanal Chem. 2015;407(26):7889–98.
Sugimoto H, Kakehi M, Satomi Y, Kamiguchi H, Jinno F. Method development for the determination of 24S-hydroxycholesterol in human plasma without derivatization by high-performance liquid chromatography with tandem mass spectrometry in atmospheric pressure chemical ionization mode. J Sep Sci. 2015;38(20):3516–24.
Arnold ME, Booth B, King L, Ray C. Workshop Report: Crystal City VI—Bioanalytical Method Validation for Biomarkers. AAPS J. 2016;18:1366–72.
Van den Eede N, Neels H, Jorens PG, Covaci A. Analysis of organophosphate flame retardant diester metabolites in human urine by liquid chromatography electrospray ionisation tandem mass spectrometry. J Chromatogr A. 2013;1303:48–53.
Calvano CD, Jensen ON, Zambonin CG. Selective extraction of phospholipids from dairy products by micro-solid phase extraction based on titanium dioxide microcolumns followed by MALDI-TOF-MS analysis. Anal Bioanal Chem. 2009;394(5):1453–61.
Gonzalvez A, Preinerstorfer B, Lindner W. Selective enrichment of phosphatidylcholines from food and biological matrices using metal oxides as solid-phase extraction materials prior to analysis by HPLC-ESI-MS/MS. Anal Bioanal Chem. 2010;396(8):2965–75.
Tong H, Holstein SA, Hohl RJ. Simultaneous determination of farnesyl and geranylgeranyl pyrophosphate levels in cultured cells. Anal Biochem. 2005;336(1):51–9.
Takami T, Fang Y, Zhou X, Jaiseng W, Ma Y, Kuno T. A genetic and pharmacological analysis of isoprenoid pathway by LC-MS/MS in fission yeast. PLoS One. 2012;7(11):e49004.
Lee JW, Devanarayan V, Barrett YC, Weiner R, Allinson J, Fountain S, et al. Fit-for-purpose method development and validation for successful biomarker measurement. Pharm Res. 2006;23(2):312–28.
Acknowledgements
We are thankful to Mr. Koichi Iida at Drug Metabolism and Pharmacokinetics Research Laboratories, Pharmaceutical Research Division, Takeda Pharmaceutical Company Limited, for fruitful discussion about the application of high-resolution mass spectrometry for the quantification of mevalonate-derived isoprenoid intermediates. We appreciate Mr. Shio Watanabe at the Application Group, LC-MS Chromatography & MS Department, Thermo Fisher Scientific, Japan, for his excellent analytical support with LC-Q-Orbi-MS.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Sugimoto, H., Iguchi, M. & Jinno, F. Bioanalysis of farnesyl pyrophosphate in human plasma by high-performance liquid chromatography coupled to triple quadrupole tandem mass spectrometry and hybrid quadrupole Orbitrap high-resolution mass spectrometry. Anal Bioanal Chem 409, 3551–3560 (2017). https://doi.org/10.1007/s00216-017-0293-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-017-0293-y