
Abstract
A new method for the simultaneous quantitative determination in human urine of 3-monochloropropane-1,2-diol (3-MCPD), a toxic food contaminant, and its metabolite, 2,3-dihydroxypropyl mercapturic acid (DHPMA), was developed and validated. After urine dilution, the analytes were separated on an Atlantis®dC18 column and quantified by liquid chromatography–tandem mass spectrometry using isotopically labelled internal standards. The limits of quantification (S/N = 10) were 1.90 and 2.21 μg/L for 3-MCPD and DHPMA, respectively. Intra- and inter-day precision were lower than 6 % for each compound. Matrix effects were evaluated. Due to the high sensitivity and good accuracy of the method, 3-MCPD and DHPMA were found in 67 and 100 % of urine samples of healthy subjects, respectively.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
3-Monochloropropane-1,2-diol (3-MCPD), a contaminant formed during processing and manufacture of foods, could derive from the reaction of chloride salts with various glycerides or from the direct reaction of hydrochloric acid with the residual vegetable oil in food and from 3-MCPD esters by lipase-catalysed hydrolysis during digestion in the gastrointestinal tract in vivo [1]. 3-MCPD was classified by the European Scientific Committee on Food in 2001 as a non-genotoxic, threshold carcinogen with a tolerable daily intake (TDI) of 2 μg/kg body weight per day [2], and its toxicity has been reviewed by the Joint FAO/WHO Expert Committee on Food Additives (JECFA) [3]. Genotoxicity data available for 3-MCPD suggest different effects related to different metabolism of this compound in bacteria [4] and mammals [5].
3-MCPD is excreted unchanged in urine (8.5 %), exhaled as CO2 (30 %), or metabolized to glycidol, followed by glutathione conjugation to raise N-acetyl-S-(2,3-dihydroxypropyl)cysteine (DHPMA), the first metabolite identified in rat urine [6]. Another pathway converted 3-MCPD in β-chlorolactic acid and finally in oxalic acid (23 %). Recently, in a 90-day toxicological study with 3-MCPD and its dipalmitate ester in rats [7], a similar urinary metabolic profile was observed for both compounds, indicating that dipalmitate ester is rapidly hydrolysed and enter in the same metabolic pathway as 3-MCPD, confirming the ester forms as a source of 3-MCPD intake.
3-MCPD was quantified both in food and biological samples, mainly by gas chromatographic mass spectrometric techniques [1]. The methods described different sample purification steps and derivatization approaches, necessary due to the matrices complexity and analytical characteristics of the compound. Even if 3-MCPD and its esters are widespread food contaminants and their toxicity is studied, no data on human biological samples are available for 3-MCPD. DHPMA, the mercapturic acid of 3-MCPD, was quantified in human urine using a liquid chromatography tandem mass spectrometry method [8].
The aims of this study were to develop and validate a new LC–MS–MS method for the simultaneous determination of 3-MCPD and DHPMA in human urines and to quantify the background concentrations in the healthy general population.
Experimental
Subjects and sampling
Spot urine samples were collected from 255 healthy subjects (114 males), mean aged 39.9 ± 11.4 (range 24–68) years enrolled among students, professors and employees of the University of Parma. There were 51 current smokers (20 %). Health status was assessed by collection of medical history, medical examination and general laboratory tests. The study was carried out according to the Declaration of Helsinki. Spot urine samples were divided into several aliquots and frozen at −20 °C until analysis.
Materials
The analytical reference standards of 3-chloropropane-1,2-diol (3-MCPD, 98 %), 3-chloropropane-1,2-diol-1,1,2,3,3-d5 (3-MCPD-d5, 97 %) as all the reagents utilized in the synthesis procedure as l-cysteine hydrochloride (≥98 %), triethylamine (≥98 %), acetic anhydride, sulphuric acid, butanol, acetone, ethanol and acetic acid were purchased from Sigma-Aldrich. HPLC-grade water, methanol and acetonitrile, used for preparing the mobile phase and for sample treatments, were supplied by Merck (VWR International srl). All the standards were used without further purification. Mercapturic acid of 3-MCPD, N-acetyl-S-(2,3-dihydroxypropyl)cysteine (DHPMA) as its isotope-labelled DHPMA-d5, were synthesized in our laboratory [7].
Instrumentation and analysis
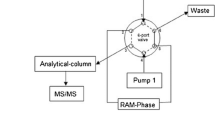
All samples and calibrators were analysed on a Agilent HP 1100 Series HPLC apparatus coupled with an AB Sciex API 4000™ triple-quadrupole mass spectrometer equipped with a TurboIonSpray® (TISP) source. Analyst® software 1.5.1 was employed for instrument control. Chromatography was performed on an Atlantis®dC18 column (2.1 × 100 mm i.d., 3 μm; Waters, Milford, MA, USA) using variable proportion of 20 mM aqueous acetic acid and methanol/acetonitrile (95/5, v/v; MeOH/AcCN) as the mobile phase [7]. The injection volume was 5 μL and each analysis required 22 min, including the re-equilibration time.
TISP–MS–MS parameters were optimized by infusing a 1 mg/L solution of 3-MCPD in 0.1 % aqueous acetic acid and a 1 mg/L solution of DHPMA in 50/50 (v/v) 0.1 % aqueous acetic acid/MeOH. The analytes were ionized in negative ion mode, and the detection was obtained in selected reaction mode (SRM) monitoring the transitions m/z 169 → 95 and m/z 236 → 107 for 3-MCPD and DHPMA, and m/z 174 → 95 and m/z 241 → 112 for 3-MCPD-d5 and DHPMA-d5, respectively. Stable isotope-labelled compounds were used as internal standards (ISs).
The concentration of DHPMA in urine samples was expressed as a function of creatinine concentration, measured by the Jaffe’s method [9].
Standard stock solutions of 3-MCPD (1000 mg/L) and DHPMA (2000 mg/L) were prepared in methanol. A fresh working solution containing 2 mg/L of 3-MCPD and 40 mg/L of DHPMA was prepared daily in aqueous acetic acid solution (0.2 %). ISs mixture (Mix ISs) was prepared in the same way (200 μg/L of 3-MCPD-d5 and 4 mg/L of DHPMA-d5).
Sample preparation
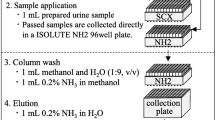
After thawing, the sample was centrifuged at 10,000 rpm for 5 min and 45 μL of supernatant were added with 5 μL of Mix ISs, diluted (1:5, v/v) with aqueous acetic acid solution (0.2 %), and then injected into the HPLC system.
Method validation
Linearity and limits of detection
Calibration standard curves were obtained by spiking a urine sample with standard mixtures at five different concentration levels, 5–200 μg/L for 3-MCPD and 100–4000 μg/L for DHPMA, respectively, with fixed concentration of Mix ISs and diluted 1/5 with aqueous acetic acid solution. Since a “blank” urine for DHPMA is not available, the detection limits (LODs, S/N = 3) and the limit of quantifications (LOQs, S/N = 10) of the analytes were determined in water and compared with those obtained in matrix using the internal standards.
Precision
The intra- and inter-day precision were calculated at two concentration levels (corresponding to the lowest and the highest values of the calibration ranges) by determining the concentrations of the analytes in a urine sample injected six fold on the same day and three fold on five different days, respectively.
Matrix effects and accuracy
Spot urine samples from five healthy subjects, chosen in order to cover the normal range (0.30–3.00 g/L) of the creatinine concentration, were collected to evaluate matrix effects, spiking each sample with the same levels of the calibration range. Matrix effects were reported as the variation coefficient of the slopes (slope CV%). Accuracy was calculated by subtracting the background concentration of the respective 3-MCPD and DHPMA obtained by analysing the un-spiked sample from analyte concentration in the spiked ones.
Statistical analysis
Statistical analysis was carried out using the SPSS/PC+ (20.0 for Windows) software. Distribution of variables was assessed by the one-sample Kolmogorov–Smirnov test. Due to the not-normal distribution of the data, urinary 3-MCPD and DHPMA concentrations were expressed as median and interquartile range [25th–75th percentile]. Differences between groups were assessed by the Mann–Whitney test for independent samples. Relationships between urinary 3-MCPD and DHPMA levels and creatinine and age were assessed by two-sided nonparametric methods (Spearman’s correlation).
Results and discussion
Liquid chromatography–mass spectrometry
LC–MS–MS operative parameters were carefully optimized. In particular, to increase sensitivity for 3-MCPD, [M+CH3COOH–H]− was selected by first mass filter adding acetic acid to the mobile phase. The optimal concentration of acetic acid in the mobile phase was set at 20 mM. Moreover, the urine samples were diluted 1/5 with aqueous acetic acid solution (0.2 %) in order to standardize the formation of acetic adduct of 3-MCPD. Mass spectra of compounds and related ISs were reported in Fig. 1. We selected the transitions m/z 169 → 95 and m/z 236 → 107 as quantifier ions for 3-MCPD and DHPMA, respectively, and the m/z 171 → 97 and m/z 236 → 89 as qualifier ones. For 3-MPCD, the most intensive fragment was m/z 59, corresponding to [CH3COO]−; we decided to monitor the transition m/z 169 → 95, considered more specific because it included the chlorine atom.

Q1 scans (left) and product ion scans (right) of 3-MCPD (a), DHPMA (c) and related deuterated compounds (b 3-MCPD-d5 and d DHPMA-d5, respectively)
Method validation
No “blank” urine samples were found for DHPMA. Therefore, both LODs and LOQs were estimated directly in urine matrix, by using the corresponding deuterated ISs. LODs for 3-MCPD and DHPMA were 0.73 and 0.71 μg/L, respectively, and the corresponding LOQs being 1.9 and 2.21 μg/L, respectively. The intra- and inter-day precision, expressed as CV%, were 3.8 and 5.9 % for 3-MCPD and 2.2 and 4.0 % for DHPMA, respectively.
To quantitatively assess the relative matrix effect, we determined the slopes of standard curves constructed in five urine samples, characterized by different creatinine concentrations during the method validation, and calculated as “slope CV (%).” For 3-MCPD, this parameter was 4.6 %, the corresponding figure for DHPMA being 3.1 %. Considering that the inter-day precision was higher than the slope CV% and that the sample manipulation required only a centrifugation step followed by dilution before the injection in the LC–MS–MS system, the method could be considered practically free from any matrix effect.
Application
This study reported for the first time the background levels of 3-MCPD in human urines using an LC–MS–MS method. The identity of the analytes (3-MCPD and DHPMA) was confirmed using specific mass transitions and retention times in association with the deuterated internal standards. Moreover, for the 3-MCPD, the chlorine isotopical ratio was monitored.
The concentrations of 3-MCPD and of its metabolite, DHPMA, in urines from 255 healthy subjects (45 % men) are summarized in Table 1, reporting median and interquartile range. Although the method is quite sensitive, 3-MCPD concentration was below the LOQ (1.90 μg/L) in 85 urine samples (33.3 %), 36.0 % of which from males and 31.2 % from females. DHPMA was detectable in all urine samples.
As an ancillary study of a 90-day toxicity experimental exposure by gavage [7], four groups of rats (10 males and 10 females) were treated with corn oil or 3-MCPD (1.84, 7.37 and 29.5 mg/kg b.w.). At all dose levels, the concentrations of free 3-MCPD were higher in female than in male rats, whereas the opposite trend was observed for DHPMA; moreover, the amounts of 3-MCPD and DHPMA excreted in urines were inversely correlated with the administered doses. In humans, 3-MCPD concentrations were similar in urines from male and female subjects (2.46 vs 2.54 μg/L, respectively).
A weakly positive correlation between creatinine and DHPMA was observed (Spearman coefficient r = 0.265, p < 0.0001), such a correlation being accounted for by samples from males only (r = 0.521, p < 0.0001). The weakly positive correlation between 3-MCPD and DHPMA found in the whole group (r = 0.176, p < 0.022) was mostly accounted for by samples from females (r = 0.257, p < 0.011). Age and smoking habits did not influence the urinary excretion amounts of both 3-MCPD and DHPMA (data not shown).
Under free dietary conditions, we observed that in human urines, DHPMA concentrations were hundred times higher than those of 3-MCPD, the median of DHPMA/3-MCPD ratio being 133. This ratio is 1 order of magnitude higher than that observed in the study on both control rats and animals treated with low doses (1.84 mg/kg b.w.). Although DHPMA is a metabolite of 3-MCPD and of its esters, it could also derive from metabolism of glycidol and glycidol-related fatty acid esters, both food contaminants [1].
Even if there is a lack of information about diet and food consumption, data collected in this study confirm that 3-MCPD is a widespread food contaminant, the intake of which can be monitored relying on both DHPMA and 3-MCPD in urine as suitable biomarkers of exposure.
Conclusions
The developed LC–MS–MS method enabled for the first time the simultaneous determination in urine of both 3-MCPD, a toxic contaminant associated with food processing, and its metabolite DHPMA. Determination was accomplished using isotopically labelled internal standards of both the analytes, which proved to be a successful method to compensate matrix effects. The method showed adequate sensitivity and selectivity for their quantitative determination in the vast majority of spot urine samples from a healthy group of the Italian general population, thus suggesting that 3-MCPD is a widespread food contaminant.
References
Baer I, de la Calle B, Taylor P (2010) 3-MCPD in food other than soy sauce or hydrolysed vegetable protein (HVP). Anal Bioanal Chem 396:443–456
SCF (Scientific Committee on Food), Opinion on 3-mono-chloro-propane-1,2-diol (3-MCPD), Updating the SCF opinion of 1994 adopted on 30 May 2001. European Commission, Brussels, 2001, http://ec.europa.eu/foof/fs/sc/scf/out91_en.pdf (accessed October 2010)
JECFA (Joint FAO/WHO Expert Committee on Food Additives). 3-Chloro-1,2-propanediol. WHO Food Add. Ser. 48, 2002, pp 401–432, WHO, Geneva. http://www.inchem.org/documents/jecfa/jecmono/v48je18.htm (accessed October 2010)
Silhánková L, Smíd F, Cerná M, Davídek J, Velísek J (1982) Mutagenicity of glycerol chlorohydrines and of their esters with higher fatty acids present in protein hydrolysates. Mutat Res 103(1):77–81
El Ramy R, OuldElhkim M, Lezmi S, Poul JM (2007) Evaluation of the genotoxic potential of 3-monochloropropane-1,2-diol (3-MCPD) and its metabolites, glycidol and beta-chlorolactic acid, using the single cell gel/comet assay. Food Chem Toxicol 45(1):41–48
Jones AR, Milton DH, Murcott C (1978) The oxidative metabolism of alfa-chlorohydrinin the male rat and the formation of spermatocoeles. Xenobiotica 8:573–582
EFSA (European Food Safety Authority) prepared by Barocelli E, Corradi A, Mutti A, Petronini PG (2011) Comparison between 3-MCPD and its palmitic esters in a 90-day toxicological study, Parma, Italy: University of Parma, Scientific report submitted to EFSA CFP/EFSA/CONTAM/2009/01
Eckert E, Schmid K, Schaller B, Hiddemann-Koca K, Drexler H, Göen T (2011) Mercapturic acids as metabolites of alkylating substances in urine samples of German inhabitants. Int J Hyg Environ Health 214(3):196–204
Kroll MH, Chesler R, Hagengruber C, Blank DW, Kestner J, Rawe M (1986) Automated determination of urinary creatinine without sample dilution: theory and practice. Clin Chem 32(3):446–452
Acknowledgments
This study was partially supported by the European Food Safety Authority (EFSA) within the project named “Comparison between 3-MCPD and its palmitic esters in a 90-day toxicological study.”
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Andreoli, R., Cirlini, M. & Mutti, A. Quantification of 3-MCPD and its mercapturic metabolite in human urine: validation of an LC–MS–MS method and its application in the general population. Anal Bioanal Chem 407, 4823–4827 (2015). https://doi.org/10.1007/s00216-015-8650-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00216-015-8650-1