
Abstract
Summary
In order to update data underlying the Italian version of FRAX, we computed the national hip fracture incidence in Italy from hospitalization records for the year 2008. Mortality data and 10-year probabilities of major osteoporotic fractures were also updated. This revision will improve FRAX accuracy and reliability.
Introduction
The original Italian version of FRAX® was based on five regional estimates of hip fracture risk undertaken up to 20 years previously. Our objective was to update hip fracture rates for the model with more recently derived data from the whole Italian population and more recent data on mortality.
Methods
We analyzed the Italian national hospitalization database for the year 2008 in order to compute age- and sex-specific hip fracture incidence rates. Re-hospitalisations of the same patients within 1 year were excluded from the analysis. Hip fracture incidence rates were computed for the age range of 40–100 years, whereas the original FRAX model lacked data on the youngest and oldest age groups. In addition, we used the national mortality data for the same year 2008 to update the model. Ten-year fracture probabilities were re-calculated on the basis of the new fracture incidence rates.
Results
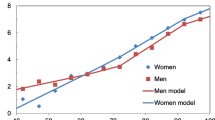
The new hip fracture age- and sex-specific incidence rates were close to those used in the original FRAX tool, although some significant differences (not exceeding 25–30 %) were found for men aged 65–75 years and women under 55 years of age. In general, the revision resulted in decreased estimated 10-year probabilities in the younger age groups, whilst those in the older age groups were slightly increased.
Conclusions
The Italian version of FRAX has been updated using the new fracture incidence rates. The impact of these revisions on FRAX is likely to increase the accuracy and reliability of FRAX in estimating 10-year fracture probabilities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Italian population is one of the oldest in Europe, with current life expectancy being 77.9 and 84.4 years for men and women, respectively [1]. About 20 % of the Italian population is over age 65 years and 4 % over the age of 80 years [1]. Since hip fracture incidence increases exponentially with age, hip fractures are a major public health issue in Italy.
Individual risk assessment as a criterion for treatment has been adopted in a number of areas such as cardiovascular diseases, where risk charts are commonly used [2, 3]. The goal of the WHO’s new fracture prediction algorithm—named FRAX®—is to provide risk assessment for osteoporotic fractures combining clinical risk factors with or without measurements of femoral neck BMD obtained using DXA. Individual risk using the FRAX algorithm is determined from the competing hazards of fracture and death and expressed as the 10-year probability of hip fracture and the 10-year probability of a major osteoporotic fracture. The FRAX algorithms in different countries use the same clinical risk factors but the fracture probability is calibrated to each country using country-specific fracture incidence and mortality rates. Ideally, each country will derive its own rates of hip and major osteoporotic fractures which can be incorporated into FRAX.
The implementation of FRAX in Italy in 2008 was based on hip fracture rates in four cities (Verona, Siena, Rome and Parma) [4] and one region (Friuli-Venezia) in Italy [5] using data collected 8–22 years ago. There are several limitations in the use of these data. The use of regional data is not ideal since there may be substantial differences in fracture rates in different regions of the same country [6]. More recent data are also preferable to account for possible secular trends in fracture and mortality [7]. The mortality rates used were based on 1999 estimates. In addition, data on fracture and mortality were not available over the whole age range included in the FRAX model (40–100 years). These considerations suggest that FRAX models should be updated from time to time based on the availability of more recent and/or on more accurate data. Indeed, updates of FRAX have been published for the Czech Republic, USA and Turkey [8–10], and revisions for Lebanon and Belgium are posted on the FRAX web site (http://www.shef.ac.uk/FRAX/). The aim of the present study was to update the incidence and mortality rates for use in the Italian version of FRAX with data which are more current, more accurate and based on national rather than regional estimates. We also wished to assess the impact of revised rates on the estimated FRAX 10-year probabilities of hip fractures and major osteoporotic fractures.
Materials and methods
Information for all hospitalizations in Italian hospitals is recorded in the national hospital discharge records and maintained centrally at the Italian Ministry of Health. This information is anonymous and includes the patient’s age, diagnosis, procedures performed and length of the hospitalization. We assumed that all hip fractures resulted in hospitalization [11–17]. The analyses of hospital discharge records were carried out for the latest available year (2008) and were performed by searching for the following ICD-9CM codes of hip fracture (major diagnosis): 820.0–820.1 (femoral neck fractures), 820.2–820.3 (per-trochanteric femoral fractures) and 820.8, 820.9 and 821.1 (other femoral fractures). These data were subject to a systematic completeness and accuracy quality assessment performed by the Ministry of Health. The matching with social security codes showed a percentage of correct linkage of 99.8 % in 2008 (58,367 records matched out of 58,492). Re-hospitalisations of the same patient within the same year 2008, including admissions to rehabilitation facilities (estimated to represent 15–20 % of total hospitalizations), were excluded by the Italian Ministry of Health. Population and mortality data were obtained by the Italian Institute for Statistics, stratified by gender and 5-year age groups (40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, 85–89, 90–94 and 95–100 years) [1]. Age- and sex-specific hip fracture incidence and mortality rates were computed and then compared with current rates used in FRAX. We have also revised the incidence rates of major osteoporotic fractures (vertebral, humeral and forearm fractures) by using the Italian revised hip fractures incidence rates from 2008 and the ratios between hip fracture and other major osteoporotic fractures as previously computed for the city of Malmö in Sweden [18].
Ten-year probabilities for hip fracture and major osteoporotic fractures were calculated by age and sex from the death and fracture hazard by Poisson models [19, 20]. Ten-year fracture probabilities were computed using body mass index (BMI) as a continuous function. The relationship between BMI and fracture risk was obtained from a previously published meta-analysis of 12 population-based cohorts [21]. For any given age, probabilities were derived assuming the expected mix of the clinical risk factors. The approach uses a simpler model than FRAX in that probabilities were population-based. Thus, for any given age, probabilities were derived assuming the expected distribution of the clinical risk factors and the score derived from them [22].
Results
Table 1 shows the number of new hip fracture cases, the population base and age- and sex-specific incidence of hip fracture for 2008 in Italy. The total number of hip fracture cases in men and women aged 40 to 100 years was 91,494 (22,693 men and 68,801 women; F/M ratio = 3). Hip fracture rates were higher in men than in women up to the age of 55 years and thereafter were consistently higher in women. As expected, the incidence increased exponentially in the older age groups to approximately 2.4 % per year in men aged 95 to 100 years and to 3.2 % in women of the same age. Age-adjusted rates standardised to the world population aged 50 years or more were 140/100,000 and 334/100,000 in men and women, respectively.
Table 1 also compares the incidence rates per 100,000 inhabitants for the year 2008 with those used in the original FRAX model. In general, for women, the rates used in the original model overestimated the fracture risk compared to the more recent estimates, although the effect was small in women over the age of 70 years. The largest differences were observed in women aged 50 to 70 years old, with the maximum difference found between the ages of 50 and 54 years (–23 %). In men, the rates used in the original model underestimated the fracture risk for 2008 between 55 and 64 years of age but overestimated the risk in those over 65 years, with the largest difference observed among men aged 65–74 years (approximately 30 %). The present study also provides hip fracture incidence for men and women aged 40–49 and 95–100 years, for whom incidence data were not available for the original FRAX model.
Table 2 summarises the distribution of hip fractures by age group in Italy in 2008. Men and women aged ≥65 years accounted for about 92 % of the total number of hip fractures (n = 83,941). Those between 85 and 100 years represented 37.5 % of hip fracture cases (34,277; 6,881 cases in men and 27,396 cases in women), although they accounted for only 4.4 % of the total Italian population aged 40 to 100 years. It is notable that older women ≥75 years old accounted for the vast majority of fractures (n = 55,952 or 61 % of the total fractures). Very old women (aged 90–100) were about 12 % of total hip fractures (n = 10,991), despite representing only 1 % of the entire population between 40 and 100 years old.
The update of hip fractures incidence rates also resulted in a change in the incidence of other major osteoporotic fractures. Table 3 shows the incidence rates of these fractures in the present study compared to those used in the original FRAX model. Differences ranged from −31 to +13 %. The greatest difference between the rates used in the original FRAX model and the present study was observed in men aged 65–74 years (up to −31 %) and in younger women aged 50–54 years (−23 %) reflecting the lower incidence of hip fracture at these ages compared with the original estimates.
Table 4 shows mortality rates due to all causes in the Italian population in 2008 compared to the mortality rates originally used in FRAX model, which were based on UN data for 1999. Mortality rates were substantially and consistently lower in both men and women aged 40–89 years old. Mortality data for oldest age groups (>85 years old) were lacking in the original FRAX model, so that mortality was underestimated in the very elderly.
Table 5 shows the effect of differences in fracture risk and mortality on fracture probabilities at different percentile of probability distribution by age category in the general population. The differences in probability estimates were relatively small. In general, the revision resulted in a lower estimated 10-year probability in the younger age groups, whilst those in the older age groups were slightly higher. For example, for a 50-year-old woman, the probability using the revised rates was about 20 % lower than if the original rates were used for both hip and major osteoporotic fractures. In 80-year-old women, the revision resulted in slightly higher 10-year probabilities (by about 10 %) compared to the original rates. Figure 1 summarises the overall impact (expressed as ratios of median fracture probability) of the revised fracture incidence and mortality data on 10-year fracture probabilities (both hip and major osteoporotic fractures), as resulted from the updated FRAX model for Italy.

Ratios of median fracture probabilities (older version 3.3 vs. revised version 3.4) of a major osteoporotic fracture and a hip fracture in White men and women for Italy
Table 6 shows 10 year fracture probabilities (FRAX v3.3 and v3.4) for specific clinical scenarios in Italy and an ad hoc selection of other countries. The modest change in the FRAX revision for Italy had no effect on the rank order of fracture probabilities.
Discussion
The FRAX algorithms aim to provide individual estimates of fracture risk that would be helpful for clinical decision making in specific countries. More than 40 models are available and FRAX has already been incorporated into treatment guidelines in several countries in Europe and North America [23–28]. In addition to the development of new models, existing models should be updated when new information becomes available. In the present study, we have replaced the hip fracture rates based on regional estimates with more recent data based on national statistics for Italy. We also substituted more recent data on mortality. In addition, a significant advancement in the accuracy of the FRAX model for Italy is that data are now available on hip fracture rates at the extremes of age (below 50 and over 95 years). This is important because FRAX provides estimates of fracture risk for individuals aged between 40 and 90 years. Therefore, in order to compute the 10-year probabilities at the age of 90 years, it is preferable to have fracture incidence and mortality data up to the age of 100 years.
In the present study, we excluded re-hospitalisations of the same patient in the same year that mainly includes re-admission for the same fracture into rehabilitation hospitals. We would have missed a small minority of cases in whom a contralateral hip fracture occurred within the same year. Thus, our results should be considered as estimates more closely reflecting the current situation than previously used in the Italian model.
We found substantial differences in the risk of hip fracture compared with the previous regional estimates. In general, the national data showed lower hip fracture incidence rates than those used in the original FRAX implementation. It is not known whether this is due to regional differences in hip fracture rates that are well documented within countries [6] or due to a national decrease in age- and sex-specific incidence—also described in several Western countries [7]. We also showed substantial and consistent differences in mortality which was lower at all ages in 2008 than in 1999. It is of interest that the WHO mortality estimates were higher than those given by the Italian Institute for Statistics for 1999.
Despite differences in fracture risk and mortality, the effect on fracture probability was modest. This is because probability depends on the competing hazards of death and fracture risk. Lower fracture rates are expected to decrease fracture probability whereas lower mortality will increase probability of fracture. However, some significant differences (by up to 20 %) were found for probability estimates in younger women and for men aged 65 to 80 years. Based on our more comprehensive and current data, we found that—in these groups—the original rates used in the FRAX model overestimated fracture risk as much as 20 %. A significant advancement in the accuracy of the FRAX model for Italy is that data are now available on hip fracture incidence rates at the extremes of age (below 50 and over 95 years). The pattern of the results is similar to those of the US revision in that in the revised Italian FRAX model younger postmenopausal women present lower incidence rates than in the original version of the algorithm [8]. However, in USA the overestimations were generally more extreme than we found for Italy. The most extreme discrepancy we found was in Italian men between 65 and 80 years old in whom the revised incidence rates were dissimilar by as much as 30 % compared to the original FRAX data.
When comparing the 2008 mortality with that data from 1999 previously used in the original model, the rates significantly decreased in all the age groups below 85 years old. As observed after updating of the US version of FRAX, the revisions resulted in small shifts of estimated probabilities but did not modify the rank order of fracture probability in the population. In the clinical scenarios presented in this paper (Table 5), the correlation coefficients between versions 3.3 and 3.4 probabilities exceeded 0.99, so that the one can be accurately predicted from the other. In other words, an individual at the 90th percentile of risk for their gender and age would still remain at the 90th percentile of risk using the revised FRAX tool. Thus, as in the revision of the US model [8], the consequences of improving the accuracy of the algorithm reside in the absolute probability generated and not in the rank order of risk.
In addition to the well-recognised problems in register studies, the present study has several limitations. A minority of countries that have a FRAX model also have robust information on the risk of the other major fractures (clinical spine, forearm and humerus). Where available, these are incorporated in the models (e.g. UK, USA, Switzerland, Sweden, Japan and Mexico). In the absence of information, FRAX models are based on the assumption that the age- and sex-specific pattern of these fractures is similar to that observed in Sweden. For example, if at a specific age and sex, the hip fracture risk is 50/10,000 in Sweden and 25/10,000 in an index country, then the incidence of forearm fractures in the index country is half that seen in Sweden at that age and sex. The computation of major osteoporotic fracture risk is more challenging than that of hip fractures because only a minority of them require hospital admission. In both the original implementation and in the current version of the FRAX in Italy, estimates of a major osteoporotic fracture were imputed from the ratio of hip fractures to major osteoporotic fractures in Sweden [29, 30] because of the absence of suitable empirical data. The available information suggests that the pattern of fractures is similar in the Western world and Australia, despite differences in incidence [18]. Further studies are needed in order to provide specific Italian data on the incidence of wrist, humerus, and clinical vertebral fractures. An additional improvement to FRAX might be the use of hip fracture and mortality rates by 1-year age intervals rather than the 5-year intervals. Other accuracy errors could be possibly overcome as fracture rates should ideally be based on the incidence of a first fracture at any one site, whereas current estimates are based on the incidence of fracture irrespective whether this is a first or subsequent fracture at the same skeletal site. The overestimate that arises has been characterised for Sweden [29] but not for other countries. Although the use of hospitalization records makes it possible to do this for hip fracture, the other outcome fractures used in FRAX are not consistently hospitalised.
Our study confirms previous findings from other countries showing that hip fractures are most frequently found in older people and particularly in women [11–16]. We found that about 40 % of hip fractures occurred in individuals over the age of 85 years, a group representing only 4.4 % of the Italian population aged 40 years or more. Since this segment of the population is increasing rapidly in Italy, it has important implications for the future focus of preventive strategies.
Conclusion
We have updated information on the incidence of hip fractures and mortality in Italy to allow the Italian version of FRAX to more accurately assess fracture probability. The impact of these revisions on FRAX resulted in a lowering of 10-year fracture probabilities in younger age groups and a slight increase in the older age groups. In order to keep the FRAX estimates accurate, it will be important for all countries to periodically provide updated fracture incidence and mortality data.
References
Italian Statistics 2008 (2009) National Institute of Statistics, Rome
Ferrario M, Chiodini P, Chambless LE et al (2005) Prediction of coronary events in a low incidence population. Assessing accuracy of the CUORE cohort study prediction equation. Int J Epidemiol 34:413–21
Conroy RM, Pyörälä K, Fitzgerald AP et al (2003) Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J 24:987–1003
Elffors L, Allander E, Kanis JA et al (1994) The variable incidence of hip fracture in southern Europe: the MEDOS study. Osteoporos Int 4:253–263
Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Oglesby A (2002) International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res 17:1237–1244
Kanis JA, Hans D, Cooper C et al (2011) Interpretation and use of FRAX in clinical practice. Osteoporos Int 22:395–411
Cooper C, Cole ZA, Holroyd CR et al (2011) Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int 22:1277–1288
Ettinger B, Black DM, Dawson-Hughes B et al (2010) Updated fracture incidence rates for the US version of FRAX®. Osteoporos Int 21:25–33
Tuzun S, Eskiyurt N, Akarırmak U et al (2012) Incidence of hip fracture and prevalence of osteoporosis in Turkey: the FRACTURK study. Osteoporos Int 23(3):949–955
Stepan JJ, Vaculik J, Pavelka K, Zofka J, Johansson H, Kanis JA (2012) Hip fracture incidence between years 1981 and 2009 and construction of a FRAX® model for the assessment of fracture probability in the Czech Republic. Calcified Tissue International (in press)
Piscitelli P, Guida G, Iolascon G et al (2007) Incidence and costs of hip fractures vs. acute myocardial infarction in the Italian population: a 4 years survey. Osteoporos Int 18:211–219
Icks A, Haastert B, Becker C, Meyer G (2008) Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int 19:1139–1145
Maravic M, Le Bihan C, Landais P, Fardellone P (2005) Incidence and cost of osteoporotic fractures in France during 2001. A methodological approach by the national hospital database. Osteoporos Int 16:1475–1480
Dimai HP, Svedbom A, Fahrleitner-Pammer A et al (2011) Epidemiology of hip fractures in Austria: evidence for a change in the secular trend. Osteoporos Int 22(2):685–92
Lippuner K, von Overbeck J, Perrelet R et al (1997) Incidence and direct medical costs of hospitalizations due to osteoporotic fractures in Switzerland. Osteoporos Int 7:414
Johnell O, Gullberg B, Allander E, Kanis JA (1992) The apparent incidence of hip fracture in Europe: a study of national register sources. Osteoporos Int 2:298–302
Pervez H, Bhargwa A, Parker MJ (2003) Accuracy and reliability of the clinical indicators related to hip fractures. Injury 34:522–524
Kanis JA, Oden A, Johnell O et al (2001) The burden of osteoporotic fractures: a method for setting intervention thresholds. Osteoporos Int 12:417–427
Kanis JA, Johnell O, Oden A, Johansson H, McCloskey E (2008) FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19(4):385–397
Oden A, Dawson A, Dere W, Johnell O, Jonsson B, Kanis JA (1998) Lifetime risk of hip fractures is underestimated. Osteoporos Int 8(6):599–603
De Laet C, Kanis JA, Oden A et al (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 16:1330–38
Kanis JA, Oden A, Johnell H et al (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos Int 18:1033–46
Compston J, Cooper A, Cooper C et al (2009) Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 62:105–108
Grossman JM, Gordon R, Ranganath VK et al (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res (Hoboken) 62:1515–26
Dawson-Hughes B (2008) A revised clinician's guide to the prevention and treatment of osteoporosis. J Clin Endocrinol Metab 93:2463–65
Association Suisse contre l’Ostéoporose ASCO (2010) Ostéoporose—Recommandations 2010. Available at http://www.svgo.ch/content/documents/ASCO_Recommandation2010_V19avril2010.pdf
Papaioannou A, Morin S, Cheung AM et al (2010) 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. CMAJ 182:1864–73
Kanis JA, Burlet N, Cooper C et al (2008) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 19:399–428
Kanis JA, Johnell O, Oden A et al (2000) Long-term risk of osteoporotic fracture in Malmo. Osteoporos Int 11:669–674
Kanis JA, Johnell O, Oden A et al (2005) Intervention thresholds for osteoporosis in men and women: a study based on data from Sweden. Osteoporos Int 16:6–14
Acknowledgments
This study has been designed at Florence University, Department of Internal Medicine and it has been supported by ONDA national observatory on women’s health through a special fellowship provided by Amgen Dompè. We are grateful to the FRAX group for the assistance in implementing this study. We thank the President of the Italian Senate Inquiry Commission on the Efficacy and Efficiency of Healthcare System, Senator I.R. Marino, Dr. L. Lispi (General Direction for Planning Affairs, Italian Ministry of Health) and Prof. A. Giordano (SHRO) for their contribution in the collection of national hospitalizations data upon which this revision is based. We also thank the OSTEOLAB research group at the Euro Mediterranean Scientific Biomedical Institute, ISBEM (Brindisi) and ORTOMED (Italian Society of Orthopaedics and Medicine).
Conflicts of interest
PP has received grants for consulting/speaking by Amgen Dompè, Ely Lilly and Servier; MLB has received research grant and funding for consulting/speaking by Novartis, Stroder, Servier, Ely Lilly, Roche, Nicomed and Amgen Dompè; JAK has declared no competing interests with respect to this paper; DMB has received research funding from Novartis, Merck and Roche/Genentech and consulting fees from Nycomed, Amgen and Zosano; GC has received a fellowship from ONDA Italian National Women’s Health Observatory supported by a grant from Amgen Dompè for this project; HJ declares no disclosures.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Piscitelli, P., Chitano, G., Johannson, H. et al. Updated fracture incidence rates for the Italian version of FRAX®. Osteoporos Int 24, 859–866 (2013). https://doi.org/10.1007/s00198-012-2021-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-012-2021-y