
Abstract
Despite the fact that the choice of bearing design has been thought to influence the functional outcomes and longevity of unicompartimental knee arthroplasty (UKA), there is a lack of clinical evidence supporting the decision-making process in patients who have undergone high tibial osteotomy (HTO). A systematic review of studies was carried out that reported the outcomes of fixed-bearing (FB) or mobile-bearing (MB) medial UKA in patients with a previous HTO. A random effect meta-analysis using a generalized linear mixed-effects model to calculate revision rates was done. Seven retrospective cohort studies were included for this study. Regarding the fixation method, 40 were the FB-UKA and 47 were MB-UKA. For both groups, the mean post-operative follow-up was 5.8 years. The survival rates were 92% for the FB-UKA with a mean follow-up of 10 years. For the MB-UKA, it ranged from 35.7 to 93%, with a mean follow-up of 4.2 years. For the FB, the time to revision was reported as 9.3 years, while 1.2, 2.5 and 2.91 years was reported for the MB. The results of the meta-analysis showed that the revision rate for the patients receiving a FB-UKA after failed HTO was 8%, compared to 17% in those who received an MB-UKA. The results of the review suggest that the use of the FB-UKA is associated with lower revision rates and a longer survival time than the MB-UKA and have similar functional ability scores.
Level of evidence: III (systematic review of level-III studies).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is scarce knowledge as to whether and under what conditions a medial unicompartimental knee arthroplasty (UKA) is possible after a prior open wedge high tibial osteotomy (OWHTO). Even less evidence is provided about the outcomes of the mobile-bearing (MB) and fixed-bearing (FB) UKA after an OWHTO [14, 20, 21]. Implantation of a UKA after an OWHTO can involve three problems: preoperative valgus alignment, abnormal proximal tibial geometry and residual medial laxity [16, 21,22,23]. In valgus correction osteotomy for the treatment of medial osteoarthritis, overcorrection to valgus alignment used to be requisite [6].
However, a more individualized approach with less overcorrection is currently recommended to decrease the risk of preoperative valgus alignment and abnormal proximal tibial geometry [15]. Partial release of the superficial medial collateral ligament (MCL) has been demonstrated to be of great importance when performing an OWHTO for two reasons. The first reason is that the release helps achieve the goal of reducing medial cartilage pressure in an OWHTO. Then, there is the fact that retaining the MCL in OWHTO mostly results in post-operative intra-articular gap reduction [17].
As a result, increased medial laxity due to a distinct cause is always present after an OWHTO. Using an FB-UKA, there is no risk of inlay dislocation, and some kind of medial laxity can be tolerated to prevent adding excessive intra-articular correction to the extra-articular correction of the previous OWHTO. This would result in post-operative mechanical valgus axis and cause progredient lateral degeneration [20]. On the contrary, using medial UKA with a mobile-bearing inlay does not offer the possibility of keeping much medial laxity because of the risk of inlay dislocation. A thicker inlay may be needed that may result in even more valgus alignment [14, 21]. Both of these facts may lead to failure or bad results in an MB-UKA after OWHTO. There is a lack of clinical evidence supporting a decision-making process in patients who have undergone OWHTO. This justifies the uncertainty and controversy surrounding MB or FB-UKA implantation in patients who have already had an HTO.
Despite the fact that the choice of bearing design has been thought to influence the functional outcomes and longevity of UKA [12], a lack of clinical evidence supporting a decision-making process in patients who underwent HTO still exists. Considering the specificity of the MB-UKA surgical technique, we hypothesized that the use of a FB-UKA leads to better results than using a MB-UKA in cases of a prior HTO. Therefore, a systematic review of the available published literature was carried out to assess the outcomes of FB-UKA and MB-UKA after a failed HTO.
Methods
This systematic review adhered to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and followed the registered protocol (PROSPERO registration: CRD42020207858) and its preparation was approved by the Systematic Reviews and Meta-Analysis Unit of the Ethics Committee and Research Committee of the Research Sub-Directorate of the U.A.N.L. School of Medicine with registration number RVS20-029.
Search strategy
An experienced librarian, in collaboration with the main investigators of the study, designed the search strategy. A thorough and comprehensive search was executed to find articles that suited the objective of the review. It included several databases covering the period from 1976, when the first use of unicompartimental knee prostheses was first introduced, to September 2020 [10]. The general databases included MEDLINE via PubMed, Elsevier via Scopus, EMBASE and Web of Science. We complemented the initial search strategy by looking at the references of the eligible selected studies for possible missing studies. Specific keywords and MeSH terms were used to assess studies evaluating the effect of the placement of an FB-UKA vs an MB-UKA on the functionality of OA in patients with a previous history of HTO. The complete search strategy is shown in Appendix 1.
Eligibility criteria
Our review used a search strategy designed to collect clinical studies reporting outcomes of FB or MB medial UKA in patients with a previous HTO. The primary outcome measures were reoperation or UKA failure (conversion to a TKA) and the time between the surgery and the failure. Secondary outcomes included functional improvement [Western Ontario and McMaster Universities Arthritis Index (WOMAC), the knee society score (KSS), the oxford knee score (OKS), the hospital for special surgery knee score (HSS)] and complications related to UKA surgery.8
The inclusion criteria adopted in our systematic review protocol were (1) single- or double-arm studies, regardless of whether it had a prospective or retrospective design; (2) studies of patients who underwent MB or FB medial UKA; (3) a previous failed HTO; (4) a report of outcome measurements in the studies in terms of failure rates, clinical and functional scores; and (5) an average follow-up of at least 2 years. No language or data restriction was adopted in our search strategy. A failed HTO was defined as persistent medial pain with radiological grade 3–4 osteoarthritis in the medial compartment of the knee [16].
Selection and data extraction process
A total of two reviewers worked independently, in duplicate, through each phase to assess eligibility for the studies. Prior to each phase, a pilot test was carried out to standardize reviewer criterion until a chance adjusted inter-rater agreement (Kappa index) of > 0.7 was arrived at. In the first phase, the title and abstracts were screened, and discordant decisions were passed to the full text phase. Following that phase, eligibility was assessed by means of full-text screening and disagreements were resolved through consensus. We used the Distiller Systematic Review Software (Distiller SR Evidence Partners) for the selection process described above.
Data collection process
For the data collection process, a pilot model was independently performed by the two reviewers, in duplicate, to assess possible disagreements or approaches to extraction and to calibrate the extraction. A web-based data extraction form was designed to standardize data extraction. This form included the following items: a section addressing the bibliographic information on the study (year, authors, country etc.), another section addressing the study question (baseline characteristics of patients, intervention, comparison and outcomes of interest) as well as the main results reported in each study. Finally, a third section was designed to address the risk of bias in each individual study. After the pilot model, the two reviewers again worked independently, in duplicate, extracting the data from each individual study. Disagreements were resolved through consensus.
Outcomes of interest
The main outcomes of interest measured in this review were the following (1) reoperation and failure of the UKA, defined as conversion to a TKA, (2) time from surgery to failure, (3) functional improvement measured with WOMAC, KSS, OKS, HSS and range of motion, (4) complications, intraoperative and post-operative, and (5) pain assessed with VAS.
Risk of bias
We assessed the risk of bias in individual studies by conducting independent in duplicate appraisals by two reviewers using the risk of bias in non-randomized studies of interventions (ROBINS-I) tool. The items used for the assessment of each study included: bias due to confounding, bias in the selection of study participants, bias in the classification of interventions, bias due to deviations from the intended interventions, bias due to missing outcome data, bias in the measurement of the outcome and bias in the selection of the reported results. Disagreements were resolved through consensus.
Data synthesis and analysis
A description from the findings of each study included in the review has been provided in the summary of findings that considers the type of intervention, target population and outcome of interest. It also included data on study characteristics like the population, sample size for each group and other descriptive variables (Table 1). For each study, a summary of the intervention effect was reported with frequencies for categorical variables and the mean or median for continuous variables. Cochrane’s handbook formula for combining groups was used for combining mean and standard deviation (SD) [8]. When possible, a random effect meta-analysis, using a generalized linear mixed-effects model to calculate revision rates, was done using R (Version 4.0) with R studio (version 1.2.5001).
Results
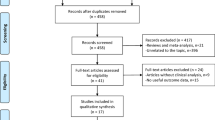
The search strategy identified 204 publications. Of those, 176 studies did not meet the inclusion criteria and were excluded. A total of 27 full-text articles were reviewed for eligibility and 20 were excluded. Finally, 7 retrospective cohort studies were included for this systematic review. Of those 7, the study by Vorlat et al. [22] included patients from two of the studies included [21, 23]. To avoid patient repetition and bias in this review, we opted to synthesize the information of those three studies into one. All the articles were written in English and published between 2000 and 2020. The complete work-flow and reasons for exclusion are shown in Fig. 1.

PRISMA 2009 Flow Diagram showing studies identified, included and excluded with relative reasons for exclusion. UKA Unicompartimental knee arthroplasty
Characteristics of included studies
Overall, 1428 UKA were performed on 1403 patients. Of those 1428, there were 87 that had had an HTO before a UKA. The indication for HTO in all studies was the treatment of medial unicompartmental osteoarthritis of the knee and a varus alignment of the limb.
The mean age of the patients was 60.3 years. Regarding gender, only three studies mentioned the distribution (male/female), two for the MB group (25/5) [16] and (2/5) [23], and one study for the FB group (13/9) [20]. As for the BMI, this was only reported by two studies: one for the MB group (23.9 ± 4.0 kg/m2) [16] and one for the FB group (27.4 kg/m2) [20]. Relative to the removal of implants previously used for osteotomy, only two studies specify it. There was one for the MB group in which the implant was not removed [22] and another for the FB group in which it was removed without specifying when the implant had been removed) [7]. In terms of the number of surgeons involved in each study, this was mentioned in four studies. There were two studies for the MB group having one surgeon [21] and four surgeons [23] and two studies for the FB group, having only one surgeon in both studies [7, 20].
Only three studies reported the time interval between HTO and UKA [14, 16, 20] with a 9-year interval for the fixed-bearing [20] and a weighted mean interval of 5.49 for the mobile-bearing [14, 16] (Table 1). With regard to the type of bearing, 40 were FB-UKA [7, 20] and 47 MB-UKA [14, 16, 22]. The mean post-operative follow-up was 5.8 years. The Oxford Unicompartimental Prosthesis was used in all MB cases. Relative to the FB-UKA, the Genesis Unicondylar implant (Smith & Nephew, Memphis, TN, USA) was used in in 18 cases [7] and the Miller–Galante metal-backed fixed-bearing prosthesis (Zimmer, Warsaw, Indiana) was used in 22 cases [20].
The survival rates were 92% for the FB-UKA with a mean follow-up of 10 years [7] and it ranged from 35.7 [22] to 93%[16] for the MB-UKA with a mean follow-up of 4.2 years. The study by Valenzuela et al. [20] and two of the previous studies from Vorlat et al. [21, 23] did not provide information on survival.
Revision
The mean time to revision was of 4.5 years. For the FB, the time to revision was reported as 9.3 years [7], unlike the MB that reported 1.2 [16], 2.5 [22] and 2.91 [14] years. Mechanical axis overcorrection brings on lateral compartment osteoarthritis as causes of the revision surgery was found in all the studies [7, 14, 16, 20, 22]. Tibial loosening and patellofemoral degeneration [16], persistent pain and effusion and the feeling of instability [14] were also described in the MB group.
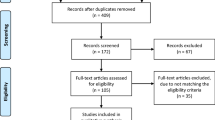
A meta-analysis was possible in five studies [7, 14, 16, 20, 22]. The results of the meta-analysis are shown in Fig. 2. Revision rates for the patients receiving the FB-UKA after a failed HTO was 8 vs. the 17% in the studies with patients that received the MB-UKA.

Generalized linear mixed-effects model for the revision rates of a mobile-bearing and b fixed-bearing
Complications
Intraoperative complications were described in one study [20] and in only two situations with the FB-UKA: a tibial plateau fracture and an osseous loose body. Additionally, Schlumberg et al. reported one prosthetic infection and one post-operative hematoma with the MB-UKA [16].
Functional scores
All the studies analyzed used different scores to evaluate the functional outcomes. Four studies used the KSS [7, 16, 20, 22], two the OKS [16, 20], one the HSS [21] and another one the WOMAC [16]. Regarding the MB-UKA, only two studies [16, 22] reported the KSS score. One of them had a mean score of 82.9 ± 10.1 (knee) and 93.3 ± 9.7 (function scores) [16] and the other only reported the score of 114 belonging to one patient [22]. Schlumberger et al. was the only study to report on other outcomes for the MB. It was the WOMAC with a score of 7.9 ± 15.69, OKS of 42.7 ± 6. Verdonk et al. reported an HSS score of 155 ± 58, but the data provided was for only 2 of the 6 patients with prior HTO [21]. One study did not provide any information on functional outcomes [14].
On the other hand, the FB-UKA reported an excellent KSS (91.49 ± 9.29 for knee scores and 89.1 ± 12.54 for function scores) [7, 20] with only one study reporting an OKS of 43.73 ± 4.43 [20].
Risk of bias
The overall risk of bias was appraised as moderate. A moderate risk of bias was assessed for three studies [7, 20, 22] and serious for two [14, 16]. The main sources of bias in the studies were confounding, missing data and the selection of reported results. The complete Risk of Bias assessment is in Table 2.
Discussion
The most important finding of this study was that the revision rates were shown to be twice as frequent in the MB-UKA group (17% revision rate) than in the FB-UKA group (8% revision rate). Additionally, the time to revision appears to be longer for the FB-UKA group than the MB-UKA group. Moreover, the FB appears to have better post-operative functional scores [11].
These results suggest that the main concern with the MB should be early failure. Furthermore, in the case of optimal implantation without early failure, patients may have similar functional outcomes as with the FB-UKA. There was not enough information to make a judgement on survival rates, complications and other functional outcomes for either type of UKA.
Our study shows similar results to those put forward by previous studies comparing the FB and MB in primary UKA [1, 3]. Cao et al. [3] reported that there were no differences in complications, knee function or revision rates between groups. However, earlier failure was seen in the MB-UKA group, which agrees with our results and previous reports. Moreover, Huang et al. [9] reported that the MB-UKA group achieved the expected post-operative limb alignment, while the FB-UKA group showed higher knee scores and superior ROM than the MB-UKA group. Lastly, Abu Al-Rub et al. found no differences between implant survival in mid and long-term in medial UKA [1].
The aforementioned suggests similar results between a primary UKA and a UKA following a failed HTO, with the only difference being that the MB-UKA seems to fail twice as much in the latter [2, 5, 13]. Thus, we can reinterpret the results initially presented by Rees et al. [14]. The recommendation would be that a prior HTO be considered a contraindication for medial UKA, suggesting that it is not an absolute contraindication. Nevertheless, each case should be evaluated individually to determine which UKA model is the most appropriate. The risk of failure of the MB-UKA may be due to its intrinsic limitation in this specific population (post-HTO) given that the inlay is not allowed to have much medial laxity with the mobile-bearing because of the risk of inlay dislocation. Additionally, using a thicker inlay to restore the tension of the medial collateral ligament may result in valgus alignment. Both of these scenarios may lead to early prosthetic failure. For these reasons Schlumberger et al. [16] have already suggested using the MB-UKA after an HTO only in cases without medial laxity or preoperative valgus alignment.
As far as we know, no prior attempts have been made to evaluate whether the MB-UKA was better than the FB-UKA in patients who had previously undergone an HTO. Only a few retrospective cohort studies have focused on this topic in the literature even though HTO is increasingly used for the treatment of symptomatic varus knee and UKA might be the proper rescue surgery in cases of a failed HTO. Consequently, it is our opinion that the topic deserves new and particular consideration. This study provides insight into an unexplored sample of patients in which the UKA is still viewed by many as a contraindication after a failed HTO.
Retrospective studies such as the one presented by Chalmers et al. [4] reveal comparable TKA results after an HTO and a UKA, they report a 9% TKA revision rate. It is comparable to the 8% FB-UKA revision rate in the present study. Additionally, excellent post-operative KSS scores were reported (mean KSS: 93), just like the ones in the present study. Therefore, the UKA may be a more cost-effective option than the TKA after a failed HTO given that it has been suggested that the UKA results in reduced operative time, fewer transfusions and shorter hospital stays [2, 18, 19]. Although a cost-effectiveness analysis is beyond the scope of this paper, the possible value of these economic implications should not be ignored but should be taken into consideration for future studies.
Several limitations need to be acknowledged. First of all, there is the high heterogeneity of the studies that does not permit an appropriate analysis of the data (functional tests applied, follow-up time, type of implant used in the case of the FB group, etc.). Even though the most common report on functional outcomes was using the KSS scale, no comparison could be made with the WOMAC, HSS and OKS due to lack of data. Second, the limited number of studies presented represent a remarkable limitation since its design is mainly of a retrospective nature with inherent methodological weaknesses. Lastly, the risk of bias in the studies included limits the generalizability of the results. Hence, the results should be interpreted with caution.
Conclusions
The FB-UKA appears to have lower revision rates as well as superior functional abilities scores than the MB-UKA. Additionally, time to revision appears to be longer for the FB-UKA group than the MB-UKA group. Well-designed clinical trials are necessary to confirm our findings and to further expand on the subject of complications and functional outcomes.
References
Abu Al-Rub Z, Lamb JN, West RM, Yang X, Hu Y, Pandit HG (2020) Survivorship of fixed vs mobile bearing unicompartmental knee replacement: a systematic review and meta-analysis of sixty-four studies and National Joint Registries. Knee 27:1635–1644
Campi S, Tibrewal S, Cuthbert R, Tibrewal SB (2018) Unicompartmental knee replacement—current perspectives. J Clin Orthop Trauma 9:17–23
Cao Z, Niu C, Gong C, Sun Y, Xie J, Song Y (2019) Comparison of fixed-bearing and mobile-bearing unicompartmental knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty 34:3114–3123
Chalmers BP, Limberg AK, Tibbo ME, Perry KI, Pagnano MW, Abdel MP (2019) Total Knee arthroplasty after high tibial osteotomy results in excellent long-term survivorship and clinical outcomes. J Bone Jt Surg 101:970–978
Cheng T, Chen D, Zhu C, Pan X, Mao X, Guo Y, Zhang X (2013) Fixed- versus mobile-bearing unicondylar knee arthroplasty: are failure modes different? Knee Surg Sports Traumatol Arthrosc 21:2433–2441
Fujisawa Y, Masuhara K, Shiomi S (1979) The effect of high tibial osteotomy on osteoarthritis of the knee. an arthroscopic study of 54 knee joints. Orthop Clin North Am 10:585–608
Heyse TJ, Khefacha A, Peersman G, Cartier P (2012) Survivorship of UKA in the middle-aged. Knee 19:585–591
Higgins J, Li T (2019) Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook. Accessed on 6 Jul 2021
Huang F, Wu D, Chang J, Zhang C, Qin K, Liao F, Yin Z (2021) A Comparison of mobile and fixed-bearing unicompartmental knee arthroplasties in the treatment of medial knee osteoarthritis: a systematic review and meta-analysis of 1861 patients. J Knee Surg 34:434–443
Johal S, Nakano N, Baxter M, Hujazi I, Pandit H, Khanduja V (2018) Unicompartmental knee arthroplasty: the past, current controversies, and future perspectives. J Knee Surg 31:992–998
Lizaur-Utrilla A, Gonzalez-Parreño S, Martinez-Mendez D, Miralles-Muñoz FA, Lopez-Prats FA (2020) Minimal clinically important differences and substantial clinical benefits for Knee Society Scores. Knee Surg Sport Traumatol Arthrosc 28:1473–1478
Mittal A, Meshram P, Kim WH, Kim TK (2020) Unicompartmental knee arthroplasty, an enigma, and the ten enigmas of medial UKA. J Orthop Traumatol 21:15
Price AJ, Svard U (2011) A second decade lifetable survival analysis of the Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res 469:174–179
Rees JL, Price AJ, Lynskey TG, Svärd UCG, Dodd CAF, Murray DW (2001) Medial unicompartmental arthroplasty after failed high tibial osteotomy. J Bone Joint Surg Br 83:1034–1036
Sabzevari S, Ebrahimpour A, Roudi MK, Kachooei AR (2016) High tibial osteotomy: a systematic review and current concept. Arch Bone Jt Surg 4:204
Schlumberger M, Oremek D, Brielmaier M, Buntenbroich U, Schuster P, Fink B (2020) Prior high tibial osteotomy is not a contraindication for medial unicompartmental knee arthroplasty. Knee Surg Sport Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06149-4
Seitz AM, Nelitz M, Ignatius A, Dürselen L (2019) Release of the medial collateral ligament is mandatory in medial open-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 27:2917–2926
Shankar S, Tetreault MW, Jegier BJ, Andersson GB, Della Valle CJ (2016) A cost comparison of unicompartmental and total knee arthroplasty. Knee 23:1016–1019
Smith WB 2nd, Steinberg J, Scholtes S, Mcnamara IR (2017) Medial compartment knee osteoarthritis: age-stratified cost-effectiveness of total knee arthroplasty, unicompartmental knee arthroplasty, and high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 25:924–933
Valenzuela GA, Jacobson NA, Buzas D, Korecki TD, Valenzuela RG, Teitge RA (2013) Unicompartmental knee replacement after high tibial osteotomy: Invalidating a contraindication. Bone Joint J 10:1348–1353
Verdonk R, Cottenie D, Almqvist KF, Vorlat P (2005) The Oxford unicompartmental knee prosthesis: A 2–14 year follow-up. Knee Surg Sports Traumatol Arthrosc 13:163–166
Vorlat P, Putzeys G, Cottenie D, Van Isacker T, Pouliart N, Handelberg F, Casteleyn P-P, Gheysen F, Verdonk R (2006) The Oxford unicompartmental knee prosthesis: an independent 10 year survival analysis. Knee Surg Sports Traumatol Arthrosc 14:40–45
Vorlat P, Verdonk R, Schauvlieghe H (2000) The Oxford unicompartmental knee prosthesis: a 5 year follow-up. Knee Surg Sport Traumatol Arthrosc 8:154–158
Funding
No funds, grants, or other support was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical approval
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and followed the registered protocol: (PROSPERO registration: CRD42020207858) and its preparation was approved by the Systematic Reviews and Meta-Analysis Unit of the Ethics Committee and Research Committee of the Research Sub-Directorate of the U.A.N.L. School of Medicine with registration number RVS20-029.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Morales-Avalos, R., Perelli, S., Raygoza-Cortez, K. et al. Fixed-bearing unicompartmental knee arthroplasty provides a lower failure rate than mobile-bearing unicompartimental knee arthroplasty when used after a failed high tibial osteotomy: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 30, 3228–3235 (2022). https://doi.org/10.1007/s00167-021-06707-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06707-4