
Abstract
Purpose
To achieve the desired alignment more accurately and improve postoperative outcomes, new techniques such as computer navigation (Navigation), patient-specific instruments (PSI) and surgical robots (Robot) are applied in Total Knee Arthroplasty (TKA). This network meta-analysis aims to compare the radiological and clinical outcomes among the above-mentioned techniques and conventional instruments (CON).
Methods
A PRISMA network meta-analysis was conducted and study protocol was published online at INPLASY (INPLASY202060018). Three databases (PubMed, EMBASE and Cochrane) were searched up to June 1, 2020. Randomised controlled trials (RCTs) comparing any two of the four techniques were included. A Bayesian network meta-analysis was performed focusing on radiological and clinical outcomes. The odds ratio (OR) or mean difference (MD) in various outcomes were calculated, and the interventions were ranked by the surface under the cumulative ranking area (SUCRA) value.
Results
Seventy-three RCTs were included, with a total of 4209 TKAs. Navigation and Robot could significantly reduce the occurrence of malalignment and malposition compared with PSI and CON, and Navigation could obtain higher medium-and-long-term KSS knee scores than CON. Robot had the greatest advantage in achieving the desired alignment accurately, followed by Navigation; Navigation had the greatest advantage in the KSS score.
Conclusion
Navigation and Robot did improve the accuracy of alignment compared with PSI and conventional instrument in TKA, but the above four techniques showed no clinical significance in postoperative outcomes.
Level of evidence
I
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The alignment and component position are key factors for the success of total knee arthroplasty (TKA) [12, 20, 24, 31, 35, 37]. To accurately achieve the desired alignment and component position, increasing new techniques have been applied in TKA, including computer navigation (Navigation) [9], patient-specific instruments (PSI) [36, 40] and surgical robots (Robot) [11]. In the past 20 years, there have been many reports on the comparison between these new techniques and conventional TKA (CON) with variable outcomes [1, 2, 6, 14, 17, 30, 34].
Up to now, there has been no literature conducting a comprehensive comparison and analysis of the above four surgical techniques. Network meta-analysis (NMA) can help to fill this gap. NMA is an extension of conventional pairwise meta-analysis. It can perform direct and indirect comparisons at the same time, even when the two measures have never been compared via head-to-head evaluation [22]. Besides, the best intervention measures can be evaluated by the value of surface under the cumulative ranking area (SUCRA) [10].
This study only included randomised controlled trials (RCTs) with level of evidence I, and conducted a thorough and comprehensive evaluation on the radiological and clinical outcomes of the four surgical techniques, i.e. Navigation, PSI, Robot, and CON, and attempted to rank the above surgical techniques. The authors hypothesised that Navigation, PSI, and Robot could improve the accuracy of alignment, but have no significant improvement on the clinical outcomes.
Methods
This NMA strictly complied with “PRISMA Extension Statement” [7]. The complete PRISMA checklist could be found in Appendix A. This NMA has been registered on the INPLASY (INPLASY202060018).
Search strategy
A comprehensive search was conducted in three databases (PubMed, EMBASE and Cochrane Library) from their inception to June 1, 2020 using a combination of MeSH terms and free words. Please refer to Appendix B for more details on search strategies.
Inclusion and exclusion criteria
Types of studies
This study only included RCTs; non-English articles, animal studies, cadaver studies, case reports, comments, letters, editorials, protocols, guidelines, unpublished articles, and review papers were excluded.
Types of participants
Patients who underwent primary TKA and were ≥ 18 years old were included, regardless of gender and race. Only the most recently published articles among the multiple articles on the same research subjects by the same author or team were included. However, if the study subjects or outcome indicators were different, they would be separately included in this NMA.
Types of interventions
RCTs containing two or more interventions of Navigation, PSI, Robot and CON were included in this NMA; the included studies were not limited to two-arm RCTs.
Types of outcomes
The radiological outcomes included: (1) mechanical axis outliers; (2) coronal femoral component angle outliers; (3) coronal tibial component angle outliers; (4) sagittal femoral component angle outliers; and (5) sagittal tibial component angle outliers. Deviations of more than 3° from the target value were defined as outliers. The clinical outcomes included: (1) short-term Knee Society Score (KSS) knee scores (follow-up period < 5 years); (2) short-term KSS function scores; (3) medium-and-long-term KSS knee scores (follow-up period ≥ 5 years); and (4) medium- and long-term KSS function scores.
Data extraction and quality assessment
Two reviewers (KL and LML) conducted the screening process of the article by reading the title and abstract, and then further evaluated the article by reading the full text. Data were extracted from the included literature according to the pre-designed table, including study characteristics, patient demographics and the risk of bias. If the data that needed to be included in the meta-analysis were lost or were only shown in the form of pictures, the authors would try to contact the author for further information. If no responses were received, data would be extracted by digital ruler software or excluded. Two investigators (KL and LML) used the Cochrane Risk of Bias Tool for RCTs to independently evaluate the bias of the included literature. Different opinions in the process were resolved by discussion or passed to a third person (LG).
Data analysis
An NMA was conducted for outcomes of the four surgical techniques in a Bayesian approach. Data were combined with a random-effects model and Markov Chain Monte Carlo was implemented to the model. In the analysis process, the prior distribution was set as normal distribution and three chains were used for simulation. The number of iterations was set to 50,000, and the first 5000 were used for the annealing algorithm to eliminate the impact of the initial value. For binary and continuous variables, odds ratios (OR) and mean differences (MD) were selected, respectively. When the 95% confidence interval (95% CI) of OR contained 1 or the 95% CI of MD contained 0, the result was considered to have no statistical significance. The interventions were ranked by the SUCRA value, which showed the percentage of effectiveness of each treatment and ranged from 0 to 100%. Intervention with larger SUCRA values was generally considered to have a better effect [10]. A network graph was drawn to reflect the number and distribution of the included literature. Meanwhile, funnel plots were applied to reflect the publication bias of outcomes that included more than 10 RCTs. Inconsistency factor (IF) and node-splitting method were used to evaluate the consistency. The I2 statistic was used to statistically assess the presence of heterogeneity. Subgroup analyses or sensitivity analyses were planned if necessary. The calculation was performed by WinBUGS (Version 1.4.3, Biostatistics the Medical Research Council, Cambridge, United Kingdom), R software (Version 4.0.2, R foundation for statistical Computing, Vienna, Austria), and Stata software (Version 15.0, Stata Corp, Texas, USA).
Results
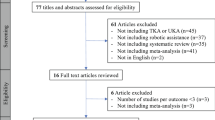
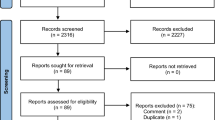
A total of 73 RCTs with 4209 TKAs were included in this NMA (Fig. 1). The characteristics and risk of bias assessment of the included literature are shown in Table 1 and Fig. 2, respectively; the network graph was shown in Fig. 3. For more details on the included literature and the risk assessment of bias, see Appendix C.

PRISMA flow diagram for selection of included RCTs

Risk of bias assessment of included RCTs

Network graph of different outcomes. a Mechanical axis outliers; b coronal femoral component angle outliers; c coronal tibial component angle outliers; d sagittal femoral component angle outliers; e sagittal tibial component angle outliers; f short-term KSS knee scores; g short-term KSS function scores; h medium-and-long-term KSS knee scores; i medium-and-long-term KSS function scores
Robot and Navigation were significantly better than PSI and CON in the control of lower limb alignment and component position (Table 2). Robot had the lowest probability of the outlier of lower limb alignment and component position, followed by Navigation (Table 3). Except for Navigation that had statistically significant difference compared to CON in medium-and-long-term knee scores, the four techniques showed no significant difference in KSS scores (Table 2). Navigation had the greatest probability of obtaining better KSS scores after surgery through ranking analysis (Table 3). The assessment revealed that heterogeneity and inconsistency were low for most outcomes (Appendix D). For more details on data analysis and publication bias, please refer to Appendix E and F, respectively.
Discussion
The most important finding of this study is that Navigation and Robot could significantly reduce the occurrence of malalignment and malposition compared with PSI and CON, but the above four techniques showed no clinical significance in postoperative outcomes.
Referring to the Knee Society roentgenographic evaluation system [5], this study evaluated alignment and component position from the following five aspects: mechanical axis outliers, coronal femoral component angle outliers, coronal tibial component angle outliers, sagittal femoral component angle outliers and sagittal tibial component angle outliers. The results showed that Robot and Navigation were significantly better than PSI and CON in the alignment and component position, and Robot had the lowest probability of outliers (Tables 2 and 3). Rhee et al. reported that Navigation could improve postoperative alignment compared with CON [34]. Van der List and Rebal also expressed the same view [33, 41]. The latest meta-analysis also agreed that Robot could significantly improve alignment and component position [1, 2, 29]. As of PSI, two latest meta-analyses also supported the views of this study [6, 17]. Besides, Pietsch et al. found a higher frequency of recuts with PSI [32]. Suggestions from PSI manufacturers for component sizes and positioning were often not accurate enough and intraoperative revision was required [4, 16, 38, 42]. Maybe these were the reasons why there was no significant difference between PSI and CON in alignment.
Knee Society clinical rating system [8] was adopted in this study to evaluate clinical outcomes; clinical scores were divided into short-term and medium-and-long-term. Except for significant difference in medium-and-long-term knee scores of Navigation compared to CON, these four techniques showed no significant difference in KSS scores. Navigation had the greatest probability of obtaining better KSS scores after surgery through ranking analysis (Tables 2 and 3). Navigation was better than CON in KSS and Western Ontario and McMaster University osteoarthritis index scores (WOMAC) during 5–8 years of follow-up [30]. Robot was also superior to CON in few postoperative clinical scores [29]. Kizaki and Mannan found that PSI did not significantly improve clinical scores compared with CON [13, 23]. The reason why so many studies showed no difference could be the commonly used scoring system nowadays, which is not sensitive enough [18]. Still, the statistical significance of patient reported outcome measures (PROM) does not necessarily represent clinical significance. Lee et al. believed that the minimal clinically important difference (MCID) of KSS knee score after TKA was 5.3–5.9 points [15], while Lizaur–Utrill’s research suggested it should be 9 points [19]. The statistical significances of Navigation with CON in medium-and-long-term knee scores (1.380 points) in this study were far from clinical significance. Navigation performed well in alignment and obtained higher scores in KSS scores, which validated the views that inaccurate alignment could result in poor clinical outcomes [12, 20, 24, 31, 35, 37]; after all, various factors could affect postoperative clinical outcomes, such as age, BMI, psychological status, soft tissue balance, component design, and rehabilitation.
This study has the following strengths compared with other meta-analyses. First, most of the previous articles were head-to-head two-arm studies. Second, the previous studies had either limited number of literatures [14, 34] or included non-RCTs, which enlarged the number [1, 2, 30]. Third, some previous articles focused only on medium-and-long-term clinical outcomes [14, 34], but RCTs with shorter follow-up are still meaningful for analysing the accuracy of alignment.
This study also has limitations. First, the prostheses in these included RCTs were different, and the navigation systems, robot systems, and PSI systems used were also diverse. Second, the biases of the included RCTs might also influence the results. Third, the indicators for evaluating clinical outcomes were various, so the authors could only the outliers and KSS scores to evaluate outcomes. Finally, there are few RCTs on Robot with long-term follow-up.
Navigation and Robot are much more expensive and require longer operation time than conventional TKA [18, 21, 39]. Besides, complications of these techniques are occasionally reported [3]. These disadvantages make the application of Navigation and Robot on normal primary TKA not so cost-efficient. However, for extremely challenging deformities [26], the advantages of Navigation and Robot may be more obvious [25,26,27,28].
Conclusion
Navigation and Robot did improve the accuracy of alignment compared with PSI and conventional instruments in TKA. Robot has the greatest advantage in achieving the desired alignment accurately, followed by Navigation; Navigation has the greatest advantage in postoperative clinical outcomes. However, the above four techniques showed no clinical significance in postoperative outcomes.
Abbreviations
- TKA:
-
Total knee arthroplasty
- Navigation:
-
Computer navigation
- Robot:
-
Surgical robots
- PSI:
-
Patient-specific instruments
- CON:
-
Conventional TKA
- NMA:
-
Network meta-analysis
- RCTs:
-
Randomised controlled trials
- OR:
-
Odds ratio
- MD:
-
Mean difference
- SUCRA:
-
Surface under the cumulative ranking area
- PROM:
-
Patient-reported outcome measures
- MCID:
-
Minimal clinically important difference
- KSS:
-
Knee Society Knee Scoring System
- WOMAC:
-
Western Ontario and McMaster University osteoarthritis index scores
References
Agarwal N, To K, McDonnell S, Khan W (2020) Clinical and radiological outcomes in robotic-assisted total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty 35:3393-3409.e3392
Chin BZ, Tan SSH, Chua KCX, Budiono GR, Syn NL, O’Neill GK (2020) Robot-assisted versus conventional total and unicompartmental knee arthroplasty: a meta-analysis of radiological and functional outcomes. J Knee Surg. https://doi.org/10.1055/s-0040-1701440
Chun YS, Kim KI, Cho YJ, Kim YH, Yoo MC, Rhyu KH (2011) Causes and patterns of aborting a robot-assisted arthroplasty. J Arthroplasty 26:621–625
Cucchi D, Menon A, Compagnoni R, Ferrua P, Fossati C, Randelli P (2018) Significant differences between manufacturer and surgeon in the accuracy of final component size prediction with CT-based patient-specific instrumentation for total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 26:3317–3324
Ewald FC (1989) The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res 248:9–12
Gong S, Xu W, Wang R, Wang Z, Wang B, Han L et al (2019) Patient-specific instrumentation improved axial alignment of the femoral component, operative time and perioperative blood loss after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 27:1083–1095
Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C et al (2015) The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 162:777–784
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Jones CW, Jerabek SA (2018) Current role of computer navigation in total knee arthroplasty. J Arthroplasty 33:1989–1993
Khera R, Murad MH, Chandar AK, Dulai PS, Wang Z, Prokop LJ et al (2016) Association of pharmacological treatments for obesity with weight loss and adverse events: a systematic review and meta-analysis. JAMA 315:2424–2434
Khlopas A, Sodhi N, Sultan AA, Chughtai M, Molloy RM, Mont MA (2018) Robotic arm-assisted total knee arthroplasty. J Arthroplasty 33:2002–2006
Kim YH, Park JW, Kim JS, Park SD (2014) The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis. Int Orthop 38:379–385
Kizaki K, Shanmugaraj A, Yamashita F, Simunovic N, Duong A, Khanna V et al (2019) Total knee arthroplasty using patient-specific instrumentation for osteoarthritis of the knee: a meta-analysis. BMC Musculoskelet Disord 20:561
Lee DY, Park YJ, Hwang SC, Park JS, Kang DG (2020) No differences in mid- to long-term outcomes of computer-assisted navigation versus conventional total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 28:3183–3192
Lee WC, Kwan YH, Chong HC, Yeo SJ (2017) The minimal clinically important difference for Knee Society Clinical Rating System after total knee arthroplasty for primary osteoarthritis. Knee Surg Sports Traumatol Arthrosc 25:3354–3359
Levy YD, An VVG, Shean CJW, Groen FR, Walker PM, Bruce WJM (2017) The accuracy of bony resection from patient-specific guides during total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 25:1678–1685
Lin Y, Cai W, Xu B, Li J, Yang Y, Pan X et al (2020) Patient-specific or conventional instrumentations: a meta-analysis of randomized controlled trials. Biomed Res Int 2020:2164371
Liow MHL, Goh GS, Wong MK, Chin PL, Tay DK, Yeo SJ (2017) Robotic-assisted total knee arthroplasty may lead to improvement in quality-of-life measures: a 2-year follow-up of a prospective randomized trial. Knee Surg Sports Traumatol Arthrosc 25:2942–2951
Lizaur-Utrilla A, Gonzalez-Parreño S, Martinez-Mendez D, Miralles-Muñoz FA, Lopez-Prats FA (2020) Minimal clinically important differences and substantial clinical benefits for Knee Society Scores. Knee Surg Sports Traumatol Arthrosc 28:1473–1478
Longstaff LM, Sloan K, Stamp N, Scaddan M, Beaver R (2009) Good alignment after total knee arthroplasty leads to faster rehabilitation and better function. J Arthroplasty 24:570–578
Lonner JH, Fillingham YA (2018) Pros and Cons: a balanced view of robotics in knee arthroplasty. J Arthroplasty 33:2007–2013
Lumley T (2002) Network meta-analysis for indirect treatment comparisons. Stat Med 21:2313–2324
Mannan A, Akinyooye D, Hossain F (2017) A meta-analysis of functional outcomes in patient-specific instrumented knee arthroplasty. J Knee Surg 30:668–674
Matsuda S, Kawahara S, Okazaki K, Tashiro Y, Iwamoto Y (2013) Postoperative alignment and ROM affect patient satisfaction after TKA. Clin Orthop Relat Res 471:127–133
Mullaji A, Lingaraju AP, Shetty GM (2012) Computer-assisted total knee replacement in patients with arthritis and a recurvatum deformity. J Bone Jt Surg Br 94:642–647
Mullaji AB, Shetty GM (2014) Correction of varus deformity during TKA with reduction osteotomy. Clin Orthop Relat Res 472:126–132
Mullaji AB, Shetty GM (2010) Lateral epicondylar osteotomy using computer navigation in total knee arthroplasty for rigid valgus deformities. J Arthroplasty 25:166–169
Mullaji AB, Shetty GM (2013) Surgical technique: computer-assisted sliding medial condylar osteotomy to achieve gap balance in varus knees during TKA. Clin Orthop Relat Res 471:1484–1491
Onggo JR, Onggo JD, De Steiger R, Hau R (2020) Robotic-assisted total knee arthroplasty is comparable to conventional total knee arthroplasty: a meta-analysis and systematic review. Arch Orthop Trauma Surg 140:1533–1549
Panjwani TR, Mullaji A, Doshi K, Thakur H (2019) Comparison of functional outcomes of computer-assisted vs conventional total knee arthroplasty: a systematic review and meta-analysis of high-quality, prospective studies. J Arthroplasty 34:586–593
Panni AS, Ascione F, Rossini M, Braile A, Corona K, Vasso M et al (2018) Tibial internal rotation negatively affects clinical outcomes in total knee arthroplasty: a systematic review. Knee Surg Sports Traumatol Arthrosc 26:1636–1644
Pietsch M, Djahani O, Hochegger M, Plattner F, Hofmann S (2013) Patient-specific total knee arthroplasty: the importance of planning by the surgeon. Knee Surg Sports Traumatol Arthrosc 21:2220–2226
Rebal BA, Babatunde OM, Lee JH, Geller JA, Patrick DA Jr, Macaulay W (2014) Imageless computer navigation in total knee arthroplasty provides superior short term functional outcomes: a meta-analysis. J Arthroplasty 29:938–944
Rhee SJ, Kim HJ, Lee CR, Kim CW, Gwak HC, Kim JH (2019) A comparison of long-term outcomes of computer-navigated and conventional total knee arthroplasty: a meta-analysis of randomized controlled trials. J Bone Jt Surg Am 101:1875–1885
Ritter MA, Davis KE, Meding JB, Pierson JL, Berend ME, Malinzak RA (2011) The effect of alignment and BMI on failure of total knee replacement. J Bone Jt Surg Am 93:1588–1596
Sassoon A, Nam D, Nunley R, Barrack R (2015) Systematic review of patient-specific instrumentation in total knee arthroplasty: new but not improved. Clin Orthop Relat Res 473:151–158
Slevin O, Hirschmann A, Schiapparelli FF, Amsler F, Huegli RW, Hirschmann MT (2018) Neutral alignment leads to higher knee society scores after total knee arthroplasty in preoperatively non-varus patients: a prospective clinical study using 3D-CT. Knee Surg Sports Traumatol Arthrosc 26:1602–1609
Stronach BM, Pelt CE, Erickson J, Peters CL (2013) Patient-specific total knee arthroplasty required frequent surgeon-directed changes. Clin Orthop Relat Res 471:169–174
Swank ML, Alkire M, Conditt M, Lonner JH (2009) Technology and cost-effectiveness in knee arthroplasty: computer navigation and robotics. Am J Orthop (Belle Mead NJ) 38:32–36
Thienpont E, Schwab PE, Fennema P (2017) Efficacy of patient-specific instruments in total knee arthroplasty: a systematic review and meta-analysis. J Bone Jt Surg Am 99:521–530
van der List JP, Chawla H, Joskowicz L, Pearle AD (2016) Current state of computer navigation and robotics in unicompartmental and total knee arthroplasty: a systematic review with meta-analysis. Knee Surg Sports Traumatol Arthrosc 24:3482–3495
Woolson ST, Harris AH, Wagner DW, Giori NJ (2014) Component alignment during total knee arthroplasty with use of standard or custom instrumentation: a randomized clinical trial using computed tomography for postoperative alignment measurement. J Bone Jt Surg Am 96:366–372
Funding
There was no financial conflict of interest with regards to this study.
Author information
Authors and Affiliations
Contributions
XC and KL composed the manuscript; LML and KL participated in the search, data extraction and quality assessment work; QF and KL completed the statistical analysis; LG and LY conceived the idea of the study. All the authors contributed to the writing of the manuscript and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors, and thus, ethical approval was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Lei, K., Liu, L., Chen, X. et al. Navigation and robotics improved alignment compared with PSI and conventional instrument, while clinical outcomes were similar in TKA: a network meta-analysis. Knee Surg Sports Traumatol Arthrosc 30, 721–733 (2022). https://doi.org/10.1007/s00167-021-06436-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06436-8