
Abstract
Purpose
The purpose of this study was to compare the effectiveness of a flexion spacer in the clinical and radiological outcomes of patients who underwent total knee arthroplasty (TKA) and to compare these patients to a group of patients subjected to the same type of surgery but without the use of a flexion spacer. It was hypothesized that patients who underwent TKA using a flexion spacer would have better clinical and radiological outcomes than those without a flexion spacer in both short- and medium-term follow-ups.
Methods
A consecutive series of patients undergoing TKA were included, yielding 20 patients in the study group. The control group was identified from the consultant database of the senior author, yielding 21 patients who underwent the same operation. All 41 patients received a Vanguard Knee System (Zimmer-Biomet, Warsaw, Indiana, USA). Cases were defined as those patients who had undergone TKA using a flexion spacer device for gap balancing; controls were defined as patients who had undergone TKA without the support of a flexion spacer device. Patients were clinically and radiographically evaluated at two consecutive follow-ups: T1—13.1 ± 1.3 months and T2—108 ± 6 months. Clinical evaluation was performed using the Knee Society Scoring System and the Western Ontario, McMaster Universities Osteoarthritis Index score. Radiographic evaluation included the femoral angle (α), the tibial angle (β), the sagittal femoral (γ) angle and the tibial slope (δ). Furthermore, the lateral patellofemoral angle (LPFA) and the Caton-Deschamps index were evaluated.
Results
No statistically significant clinical differences were found between the two groups at T1 and T2; moreover, the clinical outcomes of the two groups were stable between the two follow-ups, with no significant improvement or worsening. Radiographic evaluation showed no difference in the two groups between T1 and T2; the only significant radiographic difference between the two groups concerned the LPFA (both at 30° and 60°) at each follow-up, which was significantly greater in cases than in controls (p = 0.001).
Conclusions
The current study demonstrates that the use of a flexion spacer significantly improves radiographic patello-femoral tracking, although no significant clinical differences were found between the two groups.
Level of evidence
Case–control study, level III.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Creation of symmetrical and balanced flexion and extension gaps is a surgical goal of total knee arthroplasty. One critical step is the correct sizing and alignment of the femoral component in three dimensions, mainly in the sagittal plane and when considering rotational alignment [18]. The rotational alignment establishes the symmetry of the flexion gap, which is the key point to obtaining a stable knee throughout the range of motion and correct joint kinematics [15]. Any asymmetric flexion gap will lead to varus or valgus instability during knee flexion with pain, particularly during mid-flexion [14]. A knee with medial laxity in flexion is normally painful, while it is more tolerant of a little lateral laxity. The femoral component rotational alignment also influences correct patellar tracking [16]. Various patellofemoral complications are observed when the femoral components are rotated internally, such as lateral tilting, subluxation and dislocation of the patella and patellar maltracking. Increased lateral flexion laxity is associated with increased internal rotation of the femoral component and a less favorable clinical outcome [27]. In contrast, excessive external rotation of the femoral component will increase the medial flexion gap and could lead to symptomatic flexion instability. Several bony landmarks and surgical techniques have been described to obtain a correct alignment [4].
In recent years, to overcome this problem, a spacer has been developed for the purpose of determining, in flexion, the resection level of the posterior condyles that forms an angle parallel to the tibial osteotomy line and matches in volume and dimension the wedge that was cut in extension. Despite the several surgical techniques described, currently in the literature, there are no studies evaluating the clinical and radiographic results of TKA performed using a flexion spacer for femoral rotation.
The purpose of this study was to compare the effectiveness of a flexion spacer in the clinical and radiological outcomes of patients who underwent TKA and to compare these patients to a group of patients subjected to the same type of surgery but without the use of a flexion spacer.
It was hypothesized that patients who underwent TKA using a flexion spacer would have better clinical and radiological outcomes in both short- and medium-term follow-ups.
Materials and methods
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was conducted following the STROBE Checklist for Case Series [26].
A consecutive series of patients undergoing TKA under the care of the senior author between June 2009 and October 2011 were included, yielding 20 patients in the study group. The control group was identified from the consultant database of the senior author, yielding 21 patients who underwent the same operation. All patients were operated on by the senior author. All 41 patients received a Vanguard Knee System (Zimmer-Biomet, Warsaw, IN, USA). All patients had previously consented to participate in the unit arthroplasty database and follow-up system. Appropriate ethical approval was achieved from the local ethics committee.
Inclusion criteria were as follows: final follow-up ≥ 8 years; TKA performed by a single surgeon; patients aged between 60 and 77 years at surgery; body mass index (BMI) < 35; varus–valgus deformity ≤ 5°.
The exclusion criteria were as follows: follow-up < 8 years; multiple comorbidities and neurological illness (e.g., diabetic neuropathy, multiple sclerosis, and lateral amyotrophic sclerosis); revision surgery; and previous surgery to the affected knee (except arthroscopy for meniscectomy).
Cases were defined as those patients who had underwent a primary TKA between 2009 and 2011 using a flexion spacer device for gap balancing; controls were defined as patients who had underwent a primary TKA between 2009 and 2011 balanced without the support of a flexion spacer device.
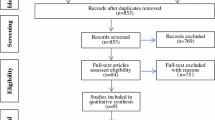
A flow chart regarding patient selection is reported in Fig. 1. The control group consisted of 21 patients, while the case group consisted of 20 patients. Patients were clinically and radiographically evaluated at two consecutive follow-ups: T1—13.1 ± 1.3 months and T2—108 ± 6 months. Detailed demographic data of the patients are reported in Table 1.

Study flowchart
Flexion spacer and surgical technique
The flexion spacer is composed of three modular elements (Fig. 2):
-
an angled element that defines the appropriate femoral external rotation (1°, 3°, 4°, 5°, 6°, 8°)
-
a support base
-
a symmetrical element that reproduces the resection volume (10, 12, 14, 16 mm).

Components of the flexion spacer, the angled elements, the base and the symmetrical elements
The stability of the assembly of the three elements is achieved through two magnets at the base.
The spacer is assembled in the volumetric configuration corresponding to that defined by the spacer block in extension and in the angular configuration considered the most appropriate; in this way, the surgeon is able to test the tension created by the femoral component on the soft tissue in flexion and then determine the point at which to cut at the correct angle to achieve correct balancing of the implant (Fig. 3). The flexion spacer allows the surgeon to obtain more precise cuts by acting on the rotation (internal or external) of the femoral component.

The flexion spacer with two different angular elements
All procedures were performed by the senior author. Surgeries were performed without the use of a tourniquet using the bone balancing technique and therefore did not require soft tissue releases [3]. All the patients included in the study were implanted with the same model of knee prosthesis [Vanguard® cruciate retaining (CR) or posterior stabilized (PS)—Zimmer-Biomet, Warsaw, Indiana, USA].
Clinical evaluation
The clinical evaluation included the official Italian version of the Knee Society Knee Scoring System (KSS), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score and the visual analog score (VAS) for pain; moreover, active and passive flexion and extension were evaluated [7, 21, 22].
Radiographic evaluation
An X-ray panel was used to assess alignment of the prosthetic components and their relations with the patella. Lateral view and axial X-rays of the patella at 30° and 60° were performed. The radiological evaluation was based on the Knee Society Roentgenographic Evaluation System [5, 12]. Four angles were measured: the femoral angle (α), the tibial angle (β), the sagittal femoral angle (γ) and the tibial slope (δ) (Fig. 4) [5, 12]. Furthermore, the lateral patellofemoral angle (LPFA) and the Caton-Deschamps index were evaluated [1, 19]. The LPFA was used to evaluate the patello-femoral joint (Fig. 5); while, the Caton-Deschamps index was used to evaluate the patellar height.

Graphical representation of α, β, γ and δ for the evaluation of the position of the prosthetic components. α: formed between the femoral axis and the tangent to the prosthesis condyles; β: formed between the tibial axis and the tangent to the prosthesis tibial plateau; γ: formed between the femoral axis and the line perpendicular to the central part of the femoral component and the tibial slope; δ: formed by the tibia axis and the tangent to the tibia plateau

Lateral patellofemoral angle. LPFA: formed by the tangent to the two condyles and the line tangent to the lateral facet of the patella
After extracting the Digital Imaging and Communications in Medicine (DICOM) data from the picture archiving and communications system (PACS), it was inserted into OsiriX® imaging software (version 4.1.2 32-bit).
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics ver. 21 (IBM SPSS, Armonk, NY, USA). Outcomes are expressed as the means ± standard deviation (SD). The Shapiro test was used to define data distribution curves and calculate frequency. Student’s t test was used for analysis of Gaussian distributions; results with a varied distribution were analyzed with the Mann–Whitney test. Statistical significance was set at p < 0.05. To ensure our sample size would yield significant results, an a priori power analysis was performed to determine the number required to prove a 10-point difference in KSS, one of our primary outcome measures. A statistical significance of p < 0.05 and power of 0.85 would require 20 patients per group. All statistical analyses were carried out using SPSS software, version 23 (IBM SPSS, Armonk, NY, USA).
Results
No statistically significant clinical differences were found between the two groups at T1 and T2; moreover, the clinical outcomes of the two groups were stable between the two follow-ups, with no significant improvement or worsening. Detailed clinical results are reported in Table 2.
Radiographic evaluation showed no difference in the two groups between T1 and T2; the only significant radiographic difference between the two groups concerned the LPFA (both at 30° and 60°) at each follow-up and was significantly greater in cases than in controls (p = 0.001). Detailed radiographic results are reported in Table 3.
No complications or revision surgeries were reported in either group.
Discussion
The most important finding of the present study was the statistically significant difference in LPFA (both at 30° and 60°) in patients who had underwent TKA using a flexion spacer device for gap balancing; moreover, no clinical differences were noted between the groups, showing that good to excellent results were achieved in patients without the use of a flexion spacer.
Currently, no article has compared clinical and radiological results in patients undergoing TKA with or without the use of a flexion spacer to achieve precise cut resection.
The patello-femoral joint plays a key role in knee kinematics; in a recent study, a mathematical model was developed to calculate the equilibrium position of the extensor mechanism for a particular tibiofemoral position. With this mathematical model, it was highlighted that the patellar tendon angle/knee flexion angle relationship is an effective indicator of abnormal kinematics post-knee arthroplasty. However, the use of the patellar tendon angle and patellar flexion angle together provided a more informative overview of the sagittal plane kinematics of the knee [25].
The influence of TKA and prosthesis designs on patellar kinematics and patellofemoral pressure was recently assessed using fresh-frozen cadavers and measuring patellofemoral pressure, patella offset, and patella tilt under the following four conditions: normal knee (patella replacement only), cruciate-retaining TKA, condylar-stabilizing TKA, and posterior-stabilized TKA [23]. The study demonstrated that although the femoral components were designed to reproduce anatomical patellar tracking, physiological patellar kinematics were not observed. Relatively high patellofemoral pressure and kinematic change after TKA may be associated with postoperative complications such as anterior knee pain [23].
In the present study, patella resurfacing was not performed in either group, and as reported in the literature, comparable outcomes were found when comparing patellar resurfacing and non-resurfacing in TKA [6].
This was confirmed by an in vitro study which showed that despite correct implantation of the patellar implants and a largely unchanged patellofemoral offset, a highly significant increase in pressure after patellar resurfacing was measured. Therefore, from a biomechanical point of view, the preservation of the native patella seems reasonable if there is no higher-grade patellar cartilage damage [13].
However, an article published in 2017 investigated the effects of patellar shape on the postoperative patellofemoral joint in TKA without patellar resurfacing and found that for a patella with a small patellar facet angle, lateral tilt was significantly increased after TKA and that a high rate of osteosclerosis was evident more than 3 years after operation [9]. Performing TKA without patellar resurfacing on a patella with a small patellar facet angle may entail a higher risk of postoperative anterior knee pain; preoperative evaluation of the shape of the patella is, therefore, important [9].
The use of a flexion spacer in total knee arthroplasty allows surgeons to achieve accurate knee balancing only with the use of bone cuts, without the need for soft tissue releases. This was also supported by a recent study reporting clinical and radiological outcomes on 914 consecutive TKAs using bone balancing [3]. At the final follow-up, the coronal alignment profile produced matches with that of the normal population, confirming that bone balancing improves satisfaction compared to that reported in the literature for mechanically aligned TKAs [3]. These results appear to be in contrast with the results of a meta-analysis performed in 2017 in which the authors found that gap balancing techniques resulted in statistically significant improvements in the restoration of mechanical and rotational alignment and mean Knee Society scores and Knee Society function scores two years postoperatively but resulted in greater elevation of the position of the joint line; no statistically significant differences were found in radiographic parameters [8].
Although the flexion spacer seems to be an effective and simple device for balancing the knee, its limitation is that it is operator dependent; in fact, the correct use and balance depends on the sensibility and experience of the first surgeon when performing the correct maneuvers. This can be considered a limitation, making the technique operator dependent.
An important role in patellar tracking is played by the prosthetic design; in the present study, the femoral component presents a trochlear groove designed to sweep back posteriorly for better patellar performance. The trochlear floor has been widened to reduce the constraining forces in extension [10, 11].
The current study presents several limitations. First, both PS and CR knee arthroplasty were included, although their procedures are not identical. Second, the patients were not randomized. Moreover, extremely selective inclusion parameters were used (varus/valgus < 5°; age) to avoid possible bias and make the groups as homogeneous as possible. In fact, for patients with angles greater than 3°, the mobilization rate of the implant in the 8th year after TKA could be as high as 24% [20, 24]. In the same way, age plays a key role; in fact, in older patients, there is a high rate of surgical complications after knee arthroplasties, and these patients achieved a statistically significant lower median Short Form-12 physical score than the younger patients [2, 17].
Furthermore, the hip–knee angle and the angle between the surgical epicondylar line and posterior condylar line were not evaluated, and there is a lack of preoperative knee deformity or alignment data.
The results of the study demonstrate how the use of a flexion spacer can be considered a valid and effective alternative to obtain the best possible femoral positioning; due to its relative simplicity, it can be of help above all for young surgeons who are new to knee prosthetic surgery.
Conclusions
The current study demonstrates that the use of a flexion spacer significantly improves radiographic patello-femoral tracking, although no significant clinical differences were found between the two groups.
References
Aït-Si-Selmi T, Marie-Hardy L, O'Loughlin PF, Kobayashi K, Müller JH, Saffarini M, Bonnin MP (2020) Patellar facet ratio affects knee pain, stair climbing and stair descent after TKA without patellar resurfacing. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-05868-y
Easterlin MC, Chang DG, Talamini M, Chang DC (2013) Older age increases short-term surgical complications after primary knee arthroplasty. Clin Orthop Relat Res 471:2611–2620. https://doi.org/10.1007/s11999-013-2985-8
Firer P, Gelbart B (2018) Balancing of total knee arthroplasty by bone cuts achieves accurately balanced soft tissues without the need for soft tissue. J ISAKOS 3:263–268. https://doi.org/10.1136/jisakos-2018-000217
Fitz W, Jäger S, Rieger JS, Seebach E, Bitsch RG (2017) Femoral rotation in total knee arthroplasty: a comparison of patient individualized jigs with gap balancing in relation to anatomic landmarks. Knee Surg Sports Traumatol Arthrosc 25:1712–1719. https://doi.org/10.1007/s00167-015-3836-9
Gao F, Ma J, Sun W, Guo W, Li Z, Wang W (2017) Radiographic assessment of knee-ankle alignment after total knee arthroplasty for varus and valgus knee osteoarthritis. Knee 24:107–115. https://doi.org/10.1016/j.knee.2016.09.023
Grassi A, Compagnoni R, Ferrua P, Zaffagnini S, Berruto M, Samuelsson K, Svantesson E, Randelli P (2018) Patellar resurfacing versus patellar retention in primary total knee arthroplasty: a systematic review of overlapping meta-analyses. Knee Surg Sports Traumatol Arthrosc 26:3206–3218. https://doi.org/10.1007/s00167-018-4831-8
Heller GZ, Manuguerra M, Chow R (2016) How to analyze the Visual Analogue Scale: myths, truths and clinical relevance. Scand J Pain 13:67–75. https://doi.org/10.1016/j.sjpain.2016.06.012
Huang T, Long Y, George D, Wang W (2017) Meta-analysis of gap balancing versus measured resection techniques in total knee arthroplasty. J Bone Jt Surg Br 99-B:151–158. https://doi.org/10.1302/0301-620X.99B2.BJJ-2016-0042.R2
Inoue A, Arai Y, Nakagawa S, Inoue H, Yoshihara Y, Yamazoe S, Kubo T (2017) Differences in patellofemoral alignment as a result of patellar shape in cruciate-retaining total knee arthroplasty without patellar resurfacing at a minimum three-year follow-up. Knee 24:1448–1453. https://doi.org/10.1016/j.knee.2017.08.050
Ip D, Wu WC, Tsang WL (2002) Comparison of two total knee prostheses on the incidence of patella clunk syndrome. Int Orthop 26:48–51. https://doi.org/10.1007/s00264-001-0316-2
Kavolus CH, Hummel MT, Barnett KP, Jennings JE Jr (2008) Comparison of the Insall-Burstein II and NexGen legacy total knee arthroplasty systems with respect to patella complications. J Arthroplasty 23:822–825. https://doi.org/10.1016/j.arth.2007.07.016
Kumar N, Yadav C, Raj R, Anand S (2014) How to interpret postoperative X-rays after total knee arthroplasty. Orthop Surg 6:179–186. https://doi.org/10.1111/os.12123
Leichtle UG, Wünschel M, Leichtle CI, Müller O, Kohler P, Wülker N, Lorenz A (2013) Increased patellofemoral pressure after TKA: an in vitro study. Knee Surg Sports Traumatol Arthrosc 22:500–508. https://doi.org/10.1007/s00167-013-2372-8
Liebs TR, Kloos SA, Herzberg W, Rüther W, Hassenpflug J (2013) The significance of an asymmetric extension gap on routine radiographs after total knee replacement: a new sign and its clinical significance. J Bone Jt Surg Br 95-B:472–477. https://doi.org/10.1302/0301-620X.95B4.31080
Manning WA, Ghosh KM, Blain A, Longstaff L, Rushton SP, Deehan DJ (2018) Internal femoral component rotation adversely influences load transfer in total knee arthroplasty: a cadaveric navigated study using the Verasense device. Knee Surg Sports Traumatol Arthrosc 26:1577–1585. https://doi.org/10.1007/s00167-017-4640-5
Matsumoto K, Ogawa H, Yoshioka H, Akiyama H (2017) Postoperative anteroposterior laxity influences subjective outcome after total knee arthroplasty. J Arthroplasty 32:1845–1849. https://doi.org/10.1016/j.arth.2016.12.043
Murphy BPD, Dowsey MM, Spelman T, Choong PFM (2018) The impact of older age on patient outcomes following primary total knee arthroplasty. J Bone Jt Surg Br 100-B:1463–1470. https://doi.org/10.1302/0301-620X.100B11.BJJ-2017-0753.R6
Nagai K, Muratsu H, Kanda Y, Tsubosaka M, Kamenaga T, Miya H, Matsushita T, Niikura T, Kuroda R, Matsumoto T (2018) Intraoperative soft tissue balance using novel medial preserving gap technique in posterior-stabilized total knee arthroplasty: comparison to measured resection technique. Knee Surg Sports Traumatol Arthrosc 26:3474–3481. https://doi.org/10.1007/s00167-018-4945-z
Prudhon JL, Caton JH, Aslanian T, Verdier R (2018) How is patella height modified after total knee arthroplasty? Int Orthop 42:311–316. https://doi.org/10.1007/s00264-017-3539-6
Rajgopal A, Dahiya V, Vasdev A, Kochhar H, Tyagi V (2011) Long-term results of total knee arthroplasty for valgus knees: soft-tissue release technique and implant selection. J Orthop Surg (Hong Kong) 19:60–63. https://doi.org/10.1177/230949901101900114
Salaffi F, Leardini G, Canesi B, Mannoni A, Fioravanti A, Caporali R, Lapadula G, Punzi L, GOnorthrosis, and Quality Of Life Assessment (GOQOLA) (2003) Reliability and validity of the Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index in Italian patients with osteoarthritis of the knee. Osteoarthr Cartil 11:551–560. https://doi.org/10.1016/s1063-4584(03)00089-x
Scuderi GR, Bourne RB, Noble PC, Benjamin JB, Lonner JH, Scott WN (2012) The new Knee Society Knee Scoring System. Clin Orthop Relat Res 470:3–19. https://doi.org/10.1007/s11999-011-2135-0
Tanikawa H, Tada M, Harato K, Okuma K, Nagura T (2017) Influence of total knee arthroplasty on patellar kinematics and patellofemoral pressure. J Arthroplasty 32:280–285. https://doi.org/10.1016/j.arth.2016.06.044
Tian F, Zang XH, Sun YS (2018) Impact of knee varus and valgus deformity on alignment in lower extremities after total knee arthroplasty (TKA). Eur Rev Med Pharmacol Sci 22:83–89. https://doi.org/10.26355/eurrev_201807_15368
van Duren BH, Pandit H, Pechon P, Hart A, Murray DW (2018) The role of the patellar tendon angle and patellar flexion angle in the interpretation of sagittal plane kinematics of the knee after knee arthroplasty: a modelling analysis. Knee 25:240–248. https://doi.org/10.1016/j.knee.2018.01.006
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Initiative STROBE (2008) The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61:344–349. https://doi.org/10.1016/j.jclinepi.2007.11.008
Westerman RW, Bhangoo NS, James P (2016) When and how is patella tracking best assessed in total knee arthroplasty surgery? J Knee Surg 29:337–340. https://doi.org/10.1055/s-0035-1554924
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors contributed equally.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interest.
Ethical approval
Ethical approval was achieved from the local ethics committee.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
D’Elicio, D.G., Attanasio, M., Ruffo, G. et al. Improving radiographic patello-femoral tracking in total knee arthroplasty with the use of a flexion spacer: a case–control study. Knee Surg Sports Traumatol Arthrosc 29, 586–593 (2021). https://doi.org/10.1007/s00167-020-05991-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-020-05991-w