
Abstract
Purpose
NexGen Legacy Posterior Stabilized high-flexion prostheses (LPS-Flex) have been popularized as an alternative to NexGen standard prostheses (LPS) in total knee arthroplasty (TKA). Advocates of this new generation prosthesis suggest improved postoperative knee flexion. The purpose of this study was to summarize the best evidence for comparing the range of motion (ROM) and functional outcomes of LPS-Flex prostheses and LPS in TKA.
Methods
Electronic databases were systematically searched to identify relevant randomized controlled trials (RCTs). The last date for our research was July 2014. Our search strategy was followed the requirements of the Cochrane Library Handbook. The methodological quality was assessed, and the data were extracted independently by two authors.
Results
Nine studies that included 978 knees met our inclusion criteria for review. The results showed that there was larger postoperative ROM (1.62, 95 % CI 0.52–2.72) in the LPS-Flex group than in the LPS group. There was not a statistically significant difference in the clinical functional scores and complications between the LPS-Flex group and the LPS group in TKA. The pooled mean differences were as follows: total KSS, −0.64 (95 % CI −1.41 to 0.13); functional KSS, −0.53 (95 % CI −1.51 to 0.45); HSS, 0.23 (95 % CI −0.87 to 1.33); complications, 0.49 (95 % CI 0.20–1.24); and radiolucent lines, 1.56 (95 % CI 0.68–3.55).
Conclusions
The preliminary results indicate that the NexGen LPS-Flex prosthesis provides an alternative to the NexGen LPS prosthesis, with greater range of motion and without severe complications or radiographic outcomes. The clinical advantages were not shown in the KSS or the HSS. Thus, the selection of a high-flexion prosthesis should depend on the characteristics of the patient, particularly high motivation and poor preoperative ROM. The potential benefits in the medium- and long-term outcomes require confirmation by larger, multicenter and well-conducted RCTs.
Level of evidence
Therapeutic study, Level I.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Range of motion (ROM) is a key factor in determining patient satisfaction because it is closely related to the overall functional outcome in patients after TKA [36]. However, the flexion of the traditional prostheses rarely exceeds 120° after surgery [4]. Recent studies showed that patient demands have increased and deeper knee flexion might be required, particularly for young patients [2, 32]. The Ontario Joint Replacement Registry and the Swedish Knee Registry have demonstrated that 17 and 20 % of total knee arthroplasty patients remain uncertain or not satisfied, respectively, with their total knee arthroplasty. Up to 10 % of the patients were dissatisfied, and poor ROM was listed as a leading cause of dissatisfaction [35, 37]. The desire to achieve greater flexion is the driving force for prosthetic modifications, and many knee arthroplasty manufactures have responded with design changes [27].
High-flexion implants (HF-TKA) have been produced to theoretically allow a greater ROM and offer better functional outcomes and increase patient satisfaction compared with standard TKA (STD-TKA). Thus, high-flexion prostheses have become increasingly accepted in recent years, particularly for those requiring high flexion, including young patients and patients in Middle Eastern and Asian populations [22, 43]. However, in the academic field, a pronounced controversy persists regarding high-flexion implants, with many clinical studies, including prospective studies and randomized, controlled trials, suggesting conflicting results [2, 11, 17, 44]. As evidence-based medicine (EBM) has become customary in the clinical field, an increasing number of doctors think that meta-analysis provides the most reliable evidence. One systematic review [29] and four meta-analyses [9, 26, 28, 42] were published from 2009 to 2011 on this subject. These studies have many limitations, and their conclusions are conflicting (Table 1). These studies included retrospective studies and various high-flexion implant brands. The design of high-flexion implants varies by the manufacturer. Additionally, surgical techniques differ. The accuracy and reliability of their outcomes were obviously low because there were many confounding factors. Whether high-flexion implants offer greater ROM and better clinical outcomes is unknown.
A number of randomized controlled trials have been performed recently to compare NexGen LPS-Flex and NexGen LPS implants in TKA [1, 10, 17, 29, 31, 33, 40, 44, 45]. Thus, a meta-analysis was conducted to investigate whether the NexGen LPS-Flex implant offers greater ROM and better clinical outcomes.
Materials and methods
Literature search
A prospective protocol defined the search strategy, eligibility criteria, quality assessment, data elements of interest and plans for data synthesis and analysis, according to the guidelines described in the Cochrane Handbook for Systematic Reviews. The electronic medical databases were searched, including PubMed, EMBASE, Web of Science and the Cochrane Library, using the following search terms: (total knee arthroplasty OR total knee replacement) AND (flexion OR range of flexion) AND (high-flexion OR high flexion). The last date for our research was July 2014. Additionally, the reference lists of the retrieved studies and relevant reviews were scrutinized.
Eligibility criteria
The study selection was performed by two reviewers, who scanned the titles and abstracts of all the citations, according to the following inclusion criteria: (1) prospective RCTs; (2) human studies; (3) studies comparing NexGen LPS-Flex implants (HF group) with NexGen LPS implants (STD group); and (4) studies reporting clinical outcomes and/or complications. Nonrandomized or retrospective studies, animal or cadaver studies, letters, comments, case reports, guidelines and review papers were excluded.
Quality assessment
Two reviewers independently assessed the methodological quality of the studies. If any disagreements occurred, a third reviewer joined the discussion until a consensus was obtained. Methodological quality included six items: sequence generation; allocation sequence concealment; blinding; incomplete outcome data; selective outcome reporting; and other potential risks. Each domain was rated as yes, no or unclear guidelines: yes = low risk of bias; no = high risk of bias; and unclear = unclear risk of bias.
Data extraction
A data extraction form was predesigned, and the data were independently extracted by two investigators, including the data on the patient demographics, surgical technique, follow-up, methodology, clinical outcomes and complications (Table 4). The data were checked by a third investigator, and any disagreements were resolved through discussion. The authors of these articles were contacted whether necessary to obtain information. Missing standard deviations were calculated based on the other values provided in the articles, according to the formula reported by Hozo et al. [14]. In addition, one article compared the following four implants: the LPS-Flex mobile, LPS-Flex fixed, LPS mobile and LPS fixed [31], and we separated them into a paired comparison: (LPS-Flex mobile vs. LPS mobile) and (LPS-Flex fixed vs. LPS fixed). Although the times at which the outcomes were measured differed among these studies, the outcomes at the final follow-up were selected for analysis because most of the patients were in the early postoperative stages (less than 5 years).
Statistical analysis
The statistical analysis was performed by RevMan 5.0 software (The Nordic Cochrane Center, The Cochrane Collaboration), and a p value of <0.05 was considered statistically significant. The weighted mean difference (WMD) and the odds of risks (OR) for continuous variables and dichotomous variables with 95 % CIs were calculated, respectively. Statistical heterogeneity was tested using the chi-square test and I 2 statistic. The χ 2 test <0.1 or the I 2 > 50 % was indicative of statistical heterogeneity. Depending on the heterogeneity, meta-analysis was performed using fixed-effect or random-effect models. When there was no statistical evidence of heterogeneity, a fixed-effect model was adopted; otherwise, a random effect was used.
Results
Description of studies
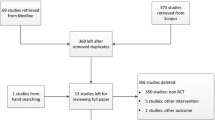
The results of the initial search retrieved 1,042 citations, and 84 articles were considered potentially eligible for further evaluation after removing the duplications and scanning the titles and abstracts. After reading the full texts for detailed evaluation, nine studies were included based on our inclusion and exclusion criteria (Fig. 1). The number of participants ranged from 50 to 278. There were 978 patients undergoing 978 TKA procedures with a weighted mean follow-up time of 46.9 months. NexGen LPS-Flex implants were used for 488 knees, and NexGen LPS implants were used for 490 knees. Table 2 summarizes the characteristics of the included trials, and the demographics of the patients were comparable in each trial.

Flowchart shows how articles were selected
Table 3 summarized the methodological quality and the level of evidence of the trials. The included studies were level I. There were six studies reporting adequate methods of randomization generation, including sealed envelopes, randomized table numbers and computer-generated randomized numbers. Of the nine articles, seven studies had blinding methods, and only two citations reported allocation concealment. There was a minimal indication of publication bias because the funnel plot reporting the postoperative ROM was symmetrical (Table 4).
Outcomes of the meta-analysis
Clinical outcomes
Range of motion was as our primary outcome for this meta-analysis (Table 5; Fig. 2). Eight studies [1, 10, 17, 29, 31, 33, 40, 45] reporting preoperative and postoperative ROM were eligible for this outcome. Our study suggested that there were advantages of high-flexion TKA (HF-TKA) over standard TKA. Patients achieved a significantly greater postoperative ROM when using high-flexion implants compared to those using a standard implant.

ROM forest plot analysis (pre- and postoperation, respectively)
As other authors have reported [9, 26, 29], there were no significant differences between the two designs with regard to the total Knee Society score, the functional Knee Society score or the Hospital for Special Surgery knee score (Figs. 3, 4, 5, respectively). Additionally, the WOMAC and SF-36 were used for the clinical assessments of the patients; however, the data were insufficient to pool for analysis.

Total KSS forest plot analysis (pre- and postoperation, respectively)

Functional KSS forest plot analysis (pre- and postoperation, respectively)

Postoperative HSS forest plot analysis
As Table 5 shows, the synthetic outcomes had no significant statistical heterogeneity among the included studies, and a fixed-effects model was selected for them.
Complications
Our meta-analysis showed that there were no significant differences in the surgical complications including delayed wound healing, superficial infection, deep infection, DVT, anterior knee pain, periprosthetic fracture, patellar fracture, postoperative stiffness and knee instability. There was no significant statistical heterogeneity among these studies, and a fixed-effects model was used (Fig. 6).

Complications forest plot analysis
Radiographic outcomes
In contrast to the concerns of the authors [12, 34], our meta-analysis showed that there were no significant differences in the radiolucent lines without heterogeneity (Fig. 7). One study reported implant loosening, and three studies reported a two-stage revision. Nieuwenhuijse et al. [31] reported that one patient was revised for aseptic loosening of the tibial component 2.7 years postoperatively in the NexGen LPS-fixed group, and one patient was revised for septic loosening 1 year after surgery. Wohlrab et al. [45] reported that one patient in the LPS-Flex group had a painful mid-flexion instability that needed to be revised. Kim et al. [20] reported that one patient had a two-stage revision because of infection.

Radiolucent lines forest plot analysis
Discussion
The most significant finding of this meta-analysis is that the NexGen LPS-Flex prosthesis provides an alternative to the NexGen LPS prosthesis with a greater range of motion and no severe complications or radiographic outcomes. Superior ROM in the high-flexion group has been previously reported by a number of authors predominantly in prospective or retrospective case series (level III or IV) [8, 12, 13, 18, 23, 38]. Clinical advantages of high-flexion prosthesis were not found by KSS or HSS.
The NexGen LPS-Flex total knee system was introduced to increase knee flexion and improve clinical outcomes. Compared with the standard NexGen LPS prosthesis, the NexGen LPS-Flex total knee system has three principle design modifications, including an extension of the posterior femoral condyles and posterior condylar radii to increase the contact area, a modification of the cam and tibial spine, and a cut-out in the polyethylene insert to prevent patellar tendon impingement [10, 17, 20]. Based on these design changes, patients might theoretically achieve greater ROM and better functional outcomes when using NexGen LPS-Flex prostheses. Recently, an increasing number of patients select high-flexion implants, particularly younger patients who are eager to return to demanding activities [43]. Klein et al. [21] reported that the intraoperative ROM of the HF-TKAs was greater by 5°º than that of STD-TKAs. A review article [16] published in 2013 reported that the HF-TKA improves the knee range of motion compared to the STD-TKA by 15°–25° and facilitates many daily deep flexion activities. Although some randomized controlled trials and one meta-analysis [17, 20, 28, 33, 45] reported no difference between the two designs, many prospective studies and randomized controlled trials [2, 15, 18, 23, 30, 44] have supported that the HF-TKA cloud significantly improves knee flexion and enhance the ability of a patient to kneel, squat and sit cross-legged, with a good early and mid-term survivorship of the implant, with very few complications. Among the 9 RCTs included in our analysis, two studies [40, 44] suggested that patients achieved greater ROM with no better KSS or HSS scores with the HF-TKAs than with the STD-TKA, whereas the remaining seven studies [1, 10, 17, 20, 31, 33, 45] found no difference in the ROM or knee scores (KSS, HSS, WOMAC and SF-36) between the two groups. Except that different high-flexion implants were used, the differences in the study design, surgical techniques and patient characteristics, including age, gender, BMI, preoperative ROM, preoperative deformity, preoperative knee scores, diagnosis, rehabilitation protocol and life style, might account for the different results. The published meta-analyses [26, 28, 29, 42] on this subject found no difference in the ROM or knee scores between the HF-TKAs and STD-TKAs. The studies included low-quality studies such as retrospective studies and prospective studies as well as different brands of high-flexion implants, which would cause extensive confounding and statistical bias.
Our study only included RCTs comparing NexGen LPS-Flex with NexGen LPS, so that the level of evidence of our study is higher and our result is more reliable. Our meta-analysis suggested that there are advantages of the NexGen LPS-Flex over NexGen LPS prosthesis, in terms of greater ROM, and no severe complications or radiographic outcomes. The clinical benefits were not shown by the KSS or HSS. The Western Ontario and McMaster University Arthritis Index (WOMAC) and the Short Form-36 (SF-36) have been reported to be more responsive measures of TKA outcomes [25]. However, there were only two studies [20, 33] reporting on the WOMAC and two studies [9, 33] reporting on the SF-36, yielding insufficient data to analyse. In addition, two meta-analyses [24, 41] on other subjects regarding TKA suggested that greater ROM did not produce significant improvement in the knee scores and that the ROM and knee scores might not have a close relationship. Chaudhary et al. [6] suggested that a difference of less than 5° for the knee ROM is not clinically relevant. Various factors influence the postoperative ROM and functional outcomes such as the preoperative ROM, age, BMI and lifestyle.
Some concerns have been suggested regarding potential deleterious effects such as increased bone resection and edge-loading, increased insert wear and increased implant loosening and revision rates [34]. However, many authors [3, 5, 19, 20] disagree and argue that the high-flexion implant modifications increase the articular contact area and improve the patellar kinematics at a high-flexion angle, which could theoretically decrease the stress concentration on the tibial polyethylene surface and potentially result in decreased wear, less osteolysis and loosening, and a low revision rate. Our meta-analysis found that there was no significant difference in the radiolucent lines between the LPS-Flex group and the LPS group, and the component loosening and revision rates were very low. Han et al. [12] reported that 38 % of patients had accepted loosening of the femoral component and up to 21 % required revision in the high-flexion group at the short-term follow-up. However, Kim et al. [18] suggested that high-flexion implants provided satisfactory results at 3–4.8 years of follow-up with an extremely low incidence of complications or adverse radiological events. The authors followed the identical patients for a minimum of 10 years and showed that there was no significant difference between the two designs with regard to the radiolucent lines, loosening and survivorship [20]. The high revision rate in Han’s study was most likely related to the surgical technique instead of the prosthesis design.
The limitations of this meta-analysis are as follows. Only studies published in English were included, which might have caused a language bias. The included studies did not evaluate every clinical result, and we could not investigate other factors related to the high-flexion implants. In addition, most of the trials focused on short-term outcomes (the weighted mean follow-up time was 46.9 months), which might have been insufficient for comparing the differences in the medium- and long-term outcomes between the two designs. Our meta-analysis had several advantages. First, the funnel plots for the pooled estimates were significantly symmetrical, indicating no publication bias. Second, only randomized, controlled trials were included, which could effectively decrease the confounding factors and other bias between the study groups. Third, only one brand of high-flexion prosthesis was included for analysis for the first time, which eliminated the heterogeneity of different prostheses. Thus, the heterogeneity was not statistically significant, and the fixed model was suited to all the statistical indicators. We theorized and showed that the patients who underwent HF-TKAs would achieve greater ROM without severe complications or radiographic outcomes.
The results of this meta-analysis are consistent with that of another meta-analysis [9], suggesting that there are advantages of the HF-TKA over the standard TKA, in terms of greater ROM and severe complications or radiographic outcome. The high-flexion implant was recommended to arthroplasty surgeons and patients based on this most current evidence. Patients would benefit and achieve markedly better functional outcomes if doctors use patient selection when recommending a high-flexion implant. Patient motivation and the need to achieve deep knee flexion could contribute to the postoperative ROM and functional outcomes. Many authors have demonstrated that patients with more high-flexion activities in daily life, such as young patients and those in Middle Eastern and Asian populations, would benefit significantly from a HF-TKA [7, 39]. The preoperative ROM is another important factor. Lee et al. [22] and Bin et al. [5] reported that high-flexion implants are more effective in restoring maximal knee flexion than standard implants and that the results were more notable when the patient had severe preoperative flexion limitations. We suggest that the selection of a high-flexion prosthesis should depend on the characteristics of the patient.
Conclusions
Our meta-analysis of the available evidence suggested that there are advantages of the NexGen LPS-Flex prosthesis over the NexGen LPS prosthesis, in terms of greater range of motion and no severe complications or radiographic outcomes. The clinical advantages were not shown by the KSS or HSS. Thus, the selection of a high-flexion prosthesis should depend on the patient characteristics, particularly high motivation and limited preoperative ROM. Determining the potential benefits in medium- and long-term outcomes requires confirmation by larger, multicenter and well-conducted RCTs.
References
Ahmed I, Gray AC, van der Linden M, Nutton R (2009) Range of flexion after primary TKA: the effect of soft tissue release and implant design. Orthopedics 32:811
Argenson JN, Komistek RD, Mahfouz M, Walker SA, Aubaniac JM, Dennis DA (2004) A high flexion total knee arthroplasty design replicates healthy knee motion. Clin Orthop Relat Res 428:174–179
Barink M, DeWaalMalefijt M, Celada P, Vena P, Van Kampen A, Verdonschot N (2008) A mechanical comparison of high-flexion and conventional total knee arthroplasty. Proc Inst Mech Eng H 222:297–307
Bellemans J, Banks S, Victor J, Vandenneucker H, Moemans A (2002) Fluoroscopic analysis of the kinematics of deep flexion in total knee arthroplasty. Influence of posterior condylar offset. J Bone Joint Surg Br 84:50–53
Bin SI, Nam TS (2007) Early results of high-flex total knee arthroplasty: comparison study at 1 year after surgery. Knee Surg Sports Traumatol Arthrosc 15:350–355
Chaudhary R, Beaupre LA, Johnston DW (2008) Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am 90:2579–2586
Dennis DA, Heekin RD, Clark CR, Murphy JA, O’Dell TL, Dwyer KA (2013) Effect of implant design on knee flexion. J Arthroplasty 28:429–438
Endres S (2011) High-flexion versus conventional total knee arthroplasty: a 5-year study. J Orthop Surg 19:226–229
Gandhi R, Tso P, Davey JR, Mahomed NN (2009) High-flexion implants in primary total knee arthroplasty: a meta-analysis. Knee 16:14–17
Guild GN, Labib SA (2014) Clinical outcomes in high flexion total knee arthroplasty were not superior to standard posterior stabilized total knee arthroplasty. A multicenter, prospective, randomized study. J Arthroplasty 29:530–534
Hamilton WG, Sritulanondha S, Engh CA Jr (2011) Results of prospective, randomized clinical trials comparing standard and high-flexion posterior-stabilized TKA: a focused review. Orthopedics 34:e500–e503
Han HS, Kang SB, Yoon KS (2007) High incidence of loosening of the femoral component in legacy posterior stabilised-flex total knee replacement. J Bone Joint Surg Br 89:1457–1461
Hepinstall MS, Ranawat AS, Ranawat CS (2010) High-flexion total knee replacement: functional outcome at one year. HSS J 6:138–144
Hozo SP, Djulbegovic B, Hozo I (2005) Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 5:13–23
Huang HT, Su JY, Wang GJ (2005) The early results of high-flex total knee arthroplasty: a minimum of 2 years of follow-up. J Arthroplasty 20:674–679
Jain S, Pathak AC, Kanniyan K, Kulkarni S, Tawar S, Mane P (2013) High-flexion posterior-stabilized total knee prosthesis: is it worth the hype? Knee Surg Relat Res 25:100–105
Kim YH, Sohn KS, Kim JS (2005) Range of motion of standard and high-flexion posterior stabilized total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am 87:1470–1475
Kim TH, Lee DH, Bin SI (2008) The NexGen LPS-flex to the knee prosthesis at a minimum of three years. J Bone Joint Surg Br 90:1304–1310
Kim YH, Choi Y, Kim JS (2009) Range of motion of standard and high-flexion posterior cruciate-retaining total knee prostheses a prospective randomized study. J Bone Joint Surg Am 91:1874–1881
Kim YH, Park JW, Kim JS (2012) High-flexion total knee arthroplasty: survivorship and prevalence of osteolysis: results after a minimum of ten years of follow-up. J Bone Joint Surg Am 94:1378–1384
Klein GR, Restrepo C, Hozack WJ (2006) The effect of knee component design changes on range of motion evaluation in vivo by a computerized navigation system. J Arthroplasty 21:623–627
Lee BS, Kim JM, Lee SJ, Jung KH, Lee DH, Cha EJ, Bin SI (2011) High-flexion total knee arthroplasty improves flexion of stiff knees. Knee Surg Sports Traumatol Arthrosc 19:936–942
Lee BS, Chung JW, Kim JM, Kim KA, Bin SI (2013) High-flexion prosthesis improves function of TKA in Asian patients without decreasing early survivorship. Clin Orthop Relat Res 471:1504–1511
Li N, Tan Y, Deng Y, Chen L (2014) Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: a meta-analysis of randomized controlled trials. Knee Surg Sports Traumatol Arthrosc 22(3):556–564
Lingard EA, Katz JN, Wright RJ, Wright EA, Sledge CB (2001) Validity and responsiveness of the Knee Society Clinical Rating System in comparison with the SF-36 and WOMAC. J Bone Joint Surg Am 83-a:1856-1864
Luo SX, Su W, Zhao JM, Sha K, Wei QJ, Li XF (2011) High-flexion vs conventional prostheses total knee arthroplasty: a meta-analysis. J Arthroplasty 26:847–854
McCalden RW, MacDonald SJ, Bourne RB, Marr JT (2009) A randomized controlled trial comparing “high-flex” vs “standard” posterior cruciate substituting polyethylene tibial inserts in total knee arthroplasty. J Arthroplasty 24:33–38
Mehin R, Burnett RS, Brasher PM (2010) Does the new generation of high-flex knee prostheses improve the post-operative range of movement?: a meta-analysis. J Bone Joint Surg Br 92:1429–1434
Murphy M, Journeaux S, Russell T (2009) High-flexion total knee arthroplasty: a systematic review. Int Orthop 33:887–893
Nam SW, Lee YS, Kwak JH, Kim NK, Lee BK (2012) A Comparison of the Clinical and Radiographic Results of Press Fit Condylar Rotating-Platform High-Flexion and Low Contact Stress Mobile Bearing Prosthesis in Total Knee Arthroplasty: short term Results. Knee Surg Relat Res 24:7–13
Nieuwenhuijse MJ, van der Voort P, Kaptein BL, Van der Linden-van der Zwaag HM, Valstar ER, Nelissen RG (2013) Fixation of high-flexion total knee prostheses: five-year follow-up results of a four-arm randomized controlled clinical and roentgen stereophotogrammetric analysis study. J Bone Joint Surg Am 95:e1411-11
Noble PC, Gordon MJ, Weiss JM, Reddix RN, Conditt MA, Mathis KB (2005) Does total knee replacement restore normal knee function? Clin Orthop Relat Res 431:157–165
Nutton RW, van der Linden ML, Rowe PJ, Gaston P, Wade FA (2008) A prospective randomised double-blind study of functional outcome and range of flexion following total knee replacement with the NexGen standard and high flexion components. J Bone Joint Surg Br 90:37–42
Ranawat CS (2003) Design may be counterproductive for optimizing flexion after TKR. Clin Orthop Relat Res 416:174–176
Report on the Ontario Joint Replacement Registry (2006) Edited (Toronto, Ontario, Canada)
Ritter MA, Campbell ED (1987) Effect of range of motion on the success of a total knee arthroplasty. J Arthroplasty 2:95–97
Robertsson O, Dunbar M, Pehrsson T, Knutson K, Lidgren L (2000) Patient satisfaction after knee arthroplasty: a report on 27,372 knees operated on between 1981 and 1995 in Sweden. Acta Orthop Scand 71:262–267
Sancheti KH, Laud NS, Bhende H, Reddy G, Pramod N, Mani JN (2009) The INDUS knee prosthesis—prospective multicentric trial of a posteriorly stabilized high-flex design: 2 years follow-up. Indian J Orthop 43:367–374
Seng C, Yeo SJ, Wee JL, Subanesh S, Chong HC, Lo NN (2011) Improved clinical outcomes after high-flexion total knee arthroplasty: a 5-year follow-up study. J Arthroplasty 26:1025–1030
Singh H, Mittal V, Nadkarni B, Agarwal S, Gulati D (2012) Gender-specific high-flexion knee prosthesis in Indian women: a prospective randomised study. J Orthop Surg 20:153–156
Smith TO, King JJ, Hing CB (2012) A meta-analysis of randomised controlled trials comparing the clinical and radiological outcomes following minimally invasive to conventional exposure for total knee arthroplasty. Knee 19(1):1–7
Sumino T, Gadikota HR, Varadarajan KM, Kwon YM, Rubash HE, Li G (2011) Do high flexion posterior stabilised total knee arthroplasty designs increase knee flexion? A meta analysis. Int Orthop 35:1309–1319
W-Dahl A, Robertsson O, Lidgren L (2010) Surgery for knee osteoarthritis in younger patients. Acta Orthop 81:161–164
Weeden SH, Schmidt R (2007) A randomized, prospective study of primary total knee components designed for increased flexion. J Arthroplasty 22:349–352
Wohlrab D, Hube R, Zeh A, Hein W (2009) Clinical and radiological results of high flex total knee arthroplasty: a 5 year follow-up. Arch Orthop Trauma Surg 129:21–24
Acknowledgments
This research was funded by the China Health Ministry Program (201302007). No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Li, C., Zeng, Y., Shen, B. et al. Patients achieved greater range of movement when using high-flexion implants. Knee Surg Sports Traumatol Arthrosc 23, 1598–1609 (2015). https://doi.org/10.1007/s00167-014-3314-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-014-3314-9