
Abstract
Purpose
Medial opening wedge high tibial osteotomy (HTO) has become increasingly popular as an alternative to lateral closing wedge osteotomy for the treatment of medial compartment knee osteoarthritis with varus deformity. The present systematic review was conducted to provide an objective analysis of total knee arthroplasty (TKA) outcomes following previous knee osteotomy (medial opening wedge vs. lateral closing wedge).
Methods
A literature search of online databases (MEDLINE, EMBASE, Cochrane Library database) was made, in addition to manual search of major orthopaedic journals. The methodological quality of each of the studies was assessed on the Newcastle–Ottawa Scale and Effective Practice and Organization of Care. A total of ten studies were included in the review. There were eight studies with Level IV and two studies with Level III evidence.
Results
Eight studies reported clinical and radiologic scores. Comparative studies between TKA following medial opening and lateral closing wedge HTO did not demonstrate statistically significant clinical and radiologic differences. The revision rates were similar. However, more technical issues during TKA surgery after lateral closing wedge HTO were mentioned than the medial open wedge group. The quadriceps snip, tibial tubercle osteotomy, and lateral soft tissue release were more frequently needed in the lateral closing wedge HTO group. In addition, because of loss of proximal tibia bone geometry in the lateral closing wedge HTO group, concerns such as tibia stem impingement in the lateral tibial cortex was noted.
Conclusion
The present systematic review suggests that TKA after medial opening and lateral closing wedge HTO showed similar performance. Clinical and radiologic outcome including revision rates did not statistically differ from included studies. However, there are more surgical technical concerns in TKA conversion from lateral closing wedge HTO than from the medial opening wedge HTO group.
Level of evidence
IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Valgization high tibial osteotomy (HTO) was first described in 1960s [7] It has been considered a successful procedure for varus osteoarthritis in young and active adults shifting the weight-bearing axis into the nonaffected lateral knee compartment [7, 13, 17]. The two most common approaches to valgus-producing HTOs are the lateral closing wedge and the medial opening wedge. Although known to be successful, however, osteoarthritis often progresses necessitating total knee arthroplasty (TKA). Insall et al. [13] reported that 23 % of patients previously underwent HTO needed TKA.
Given the change in mechanical axis of limb alignment and proximal tibia geometry after HTO, performance of TKA following HTO has been studied previously. Most of the studies reported outcomes after closing wedge HTO converted to TKA [1, 2, 10, 14, 20, 24]. In comparison with primary TKAs, most studies reported similar outcomes of TKAs converted from HTO [23, 25].
Traditionally, lateral closing wedge HTOs were more common; however, in the late 1990s and early 2000s, medial opening wedge HTOs became increasingly popular as an alternative to lateral closing wedge HTO. Its potential advantages include easier correction of varus deformities, preservation of proximal tibia bone stock and no disruption of the proximal tibiofibular joint, avoidance of peroneal nerve injury, and less incidence of compartment syndrome [12]. Because of preservation of proximal tibia bone stock after medial opening wedge HTO, it has been reported to have lesser technical issues during TKA procedure than the lateral closing wedge HTO [3].
The present systematic review was conducted to provide an objective analysis of TKA outcomes following previous knee osteotomy (medial opening wedge vs. lateral closing wedge). To the authors’ knowledge, this is the first review written in English directly comparing the TKA results after medial opening wedge and lateral closing wedge HTO. The hypothesis was that medial opening wedge HTO enables easier conversion to TKA than does lateral closing wedge HTO and thus superior performance of TKA.
Materials and methods
Eligibility criteria
Published studies meeting the selection criteria listed in Table 1 were included in the systematic review.
Search strategy
A literature search of online databases (MEDLINE, EMBASE, Cochrane database) was performed. For each databases, search protocol was employed. Citations in the included studies were screened, and relevant experts in the field were contacted in order to identify additional studies. Two review authors independently selected from citations based on the corresponding titles and abstracts. The eligibilities of the relevant full papers were then assessed. In cases where consensus could not be reached, a third review author was consulted.
Data extraction
Each of the selected studies was evaluated by the two independent review authors for methodological quality. Data were extracted according to the following standardized protocol: study type, level of evidence, demographic information, prostheses used, surgical details, outcome measures, clinical and radiographic findings, complications, and survival rates. The extracted data were then cross-checked for accuracy. Any disagreements, again, were settled by the third review author.
Quality assessment
The methodological quality of each of the studies was assessed on the Newcastle–Ottawa Scale (NOS) [27]. The assessment proceeded within three domains: study group selection, intergroup comparability, and ascertainment of exposure and outcome of interest. Within the “selection” (four numbered items) and “outcome” (three numbered items) domains, each assessed study could be awarded a maximum of one star for each numbered item. Within the “comparability” (one numbered item) domain, a maximum of two stars could be awarded. On the NOS, the higher the score, the higher the study quality. All of the scores were determined by the two review authors, first independently and then by consensus. An assessment tool suggested by the Effective Practice and Organization of Care (EPOC) review for case series was utilized. Seven standard criteria are used for interrupted time series.
Results
Included studies
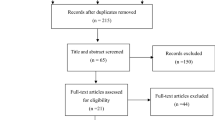
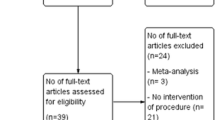
After the full-text review, ten studies were subjected to the final systematic review. The search strategy is outlined in Fig. 1, and an overview of the study characteristics is presented in Tables 2 and 3. All of the included studies had a minimum follow-up of at least 1 year. The rationale for conversion of HTO to TKA was progression of osteoarthritis.

PRISMA flow diagram
Quality assessment
Details on the NOS- and EPOC-based methodological quality assessment of the included studies are presented in Table 4. The nonrandomized comparative studies [1, 3, 6, 22] had cohort and control groups (within studies) that were well matched in terms of demographics, prognostic variables, and surgical technique.
Surgical intervention
The intraoperative results are shown in Table 5. Seven studies reported on knee prosthesis design. Regarding the operation time, Bastos et al. [3] found no significant differences in operation time between TKA after medial opening and lateral closing wedge HTO. For the soft tissue release during TKA procedure, Bastos et al. [3] reported that significantly more medial releases were required in the medial opening wedge HTO group and that there was no significant difference in the need for lateral release between the two groups. Regarding the exposure, there were more incidences of procedures such as a quadriceps snip or tibial tubercle osteotomy for the lateral closing wedge HTO group.
Clinical outcomes
The clinical outcomes are provided in Table 6. Eight studies reported clinical scores: a Hospital for Special Surgery (HSS) score in one study, a Knee Society Clinical Rating System score (KSS) in five studies, a Western Ontario and McMaster University Osteoarthritis Index (WOMAC) in one study, an Oxford knee score in one study, a SF-12 in one study, and an International Knee Society score (IKS) in one study. All of the case series [1, 2, 8, 10, 24] showed improvement in clinical scores. Between the use of CR- or PS-type prosthesis after lateral closing wedge HTO, Akasaki et al. [1] reported statistically significant inferior clinical outcome in CR-TKA group. However, Chen et al. [6] did not show difference between the use of CR- and PS-type prostheses. Comparative studies between TKA following medial opening and lateral closing wedge HTO did not demonstrate statistical significant clinical differences [3, 22].
Radiologic outcomes
The radiologic outcomes are shown in Table 7. Eight studies reported radiologic outcome [1–3, 8, 10, 14, 20, 24]. All studies demonstrated towards neutral alignment after performing TKA. Regarding the patella height, no significant differences were demonstrated between pre- and postoperation TKA in case series for lateral closing wedge HTO studies [2, 10, 20]. There was also no difference in patella height in medial opening wedge HTO case series [8].
Revision and complications
Two studies reported survival rates [10, 22]. Overall, there were no significant differences between groups. Detailed information regarding the reasons for revisional surgeries and complications is demonstrated in Table 8.
Discussion
The important finding of this systematic review is that although the TKA conversion from medial opening wedge HTO was technically easier than the lateral closing wedge HTO, the clinical and radiologic outcome including revision rates (survival rate) did not statistically differ between two groups. The initial hypothesis failed to demonstrate superior performance of TKA following medial opening wedge HTO than the lateral closing wedge HTO group.
Total knee arthroplasty (TKA) after failed HTO is known to be a technically demanding procedure [4, 5, 9, 21]. A number of studies have emphasized issues including soft tissue problems, difficulty with patella eversion, management of retained hardware, handling of coronal and sagittal plane deformities of the proximal tibia, and difficulties with ligament balancing. When performing TKA after either medial opening or lateral closing HTO, surgeons should consider the following factors: higher rates of preoperative limb malalignment, instability, stiffness, patellar maltracking, patella infera, surgical approaches, and previous hardware. Careful preoperative planning is required, and intraoperative difficulties should be anticipated [3, 9].
Specific knee prosthesis choice may be one of the important factors relevant to knee implant longevity [16]. Walther et al. [26] reported that posterior cruciate ligament (PCL) substituting implants seem to produce more predictable results, with less pain, and provide more stability in the anteroposterior direction, especially in cases with severe bone loss and a tenuous PCL. They suggested that inadequate PCL function would be observed more often in post-HTO arthroplasty than in patients without previous surgery. Akasaki et al. [1] performed comparative study between PS- and CR-type prostheses following failed HTO. They concluded that the midterm clinical results following CR-TKA were inferior to those after PS-TKA. They suggested that postoperative knee instability might be due in part to postoperative PCL insufficiency and that PCL-substituting TKA would be more suitable after HTO. However, Chen et al. [6] recently reported that although PS prostheses offer better range of motion in TKA after previous HTO, knee stability, clinical scores, and revision rates were similar in PS and CR prostheses. According to the included studies (Table 5) for this systematic review, there was no preference in using CR or PS for TKA after HTO.
There were surgical issues in performing TKA on patients who underwent HTO. In the aspect of surgical exposure, quadriceps snip and tibial tuberosity osteotomy were performed more frequently in the lateral closing wedge HTO group. Gupta et al. [10] reported 12.1 % of quadriceps snip in their lateral closing wedge HTO case series. Erak et al. [8] reported 2.9 % of quadriceps snip in their medial opening wedge HTO case series. In the comparative study performed by Bastos et al. [3], they needed more additional procedures for the lateral closing wedge HTO group in comparison with medial opening wedge HTO group in the aspect of quadriceps snip (2.6 vs. 0 %) and tibial tuberosity osteotomy (22.2 vs. 8.3 %). The difficulty of patella eversion in TKA after lateral closing wedge HTO has also been noted in other studies. Haddad et al. [11] reported that rectus snip was necessary in 16 % of patients, and Nizard et al. [19] found that tibial tubercle osteotomy was needed in 11 % of cases. Windsor et al. [28] previously reviewed 45 patients who had been treated with TKA after tibial osteotomy. They reported technical difficulties, not only with exposure particularly, but also in relation to the loss of bone stock and to impingement of the stem of the tibial component on the lateral tibial cortex. Impingement can be avoided by implanting undersized tibial trays and leaving the lateral tibial plateau partially uncovered or by positioning the tibial tray more medially, with the risk of overhang and medial collateral ligament impingement [10, 15]. The proximal tibia is shortened and therefore must be cut as thin as possible to expose cancellous bone for cementation of the tibial component and avoidance of flexion and extension gap imbalance [18]. This is more frequent situation during TKA surgery in patients who previously had lateral closing wedge HTO. One of the theoretical advantages of TKA after opening wedge HTO is preservation of proximal tibial anatomy; therefore, technical difficulties such as the tibia stem impingement on the lateral cortex do not occur.
In the present systemic review, similar TKA clinical improvements were demonstrated in both medial opening and lateral closing wedge HTO. There was no clear clinical and/or radiologic difference between groups. However, some studies reported less satisfactory TKA outcomes, which may be due to post-HTO patients. Gupta et al. [10] reported poor results in four knees due to the presence of patella baja. They hypothesized that patella baja was due to patellar tendon shortening from 6 to 8 weeks of post-HTO cast immobilization. Among results, patella baja was more common in TKA after lateral closing wedge HTO group than that after medial opening wedge HTO group (Table 7) [3].
An increased tibial slope causes anterior tibial translation and possible instability in flexion. Likewise, a decrease in the slope leads to posterior tibial translation, posterior capsule contraction, and decrease in flexion. Maintenance of tibial slope is mandatory for satisfactory outcome after HTO. One study mentioned the issue of the posterior tibial slope. Erak et al. [8] noted that 21 % of their medial opening wedge HTO had a tibial slope of over 15° after operation. Tibial slope tends to be increased after medial opening HTO, which can lead to large anterior tibial resections and/or defects in the posterior tibia, and can also affect flexion/extension balancing.
Ligament balancing is another important outcome factor after TKA. A tibial osteotomy produces an extra-articular deformity that influences soft tissue tension. At the time of prosthesis implantation, a tibial bone cut perpendicular to the mechanical axis leads to asymmetric tibial resection. This asymmetric tibial resection produces the so-called resection laxity, which may increase the pre-existing imbalance. Erak et al. [8] found that extra medial dissection for removal of hardware on patients with previous medial opening wedge HTO can lead to medial laxity requiring lateral ligament release to balance the knee. Bastos et al. [3] suggested that higher rates of lateral release following lateral closing wedge HTO are most likely due to postosteotomy scarring that occurs on the lateral side of the knee.
Limitations of this systematic review should be noted. First, no randomized controlled trial was included. Second, there were only two studies directly reporting TKA outcomes between medial opening and lateral closing wedge HTO. Although single-arm case series were included to support the comparative studies, there are possible consequences that the pooled analyses are biased. Third, since medial opening wedge HTO procedure has recently increased in contrast to lateral closing wedge HTO which has been a much older procedure, lateral closing wedge HTO had more time to fail requiring conversion to TKA. Well-designed longer follow-up studies are further required for definitive conclusions.
Conclusion
The present systematic review suggests that TKA after medial opening and lateral closing wedge HTO showed similar performance. Clinical and radiologic outcome including revision rates did not statistically differ from included studies. However, there are more surgical technical concerns in TKA conversion from lateral closing wedge HTO than from the medial opening wedge HTO group.
References
Akasaki Y, Matsuda S, Miura H, Okazaki K, Moro-oka TA, Mizu-uchi H, Iwamoto Y (2009) Total knee arthroplasty following failed high tibial osteotomy: mid-term comparison of posterior cruciate-retaining versus posterior stabilized prosthesis. Knee Surg Sports Traumatol Arthrosc 17:795–799
Bae DK, Song SJ, Yoon KH (2010) Total knee arthroplasty following closed wedge high tibial osteotomy. Int Orthop 34:283–287
Bastos Filho R, Magnussen RA, Duthon V, Demey G, Servien E, Granjeiro JM, Neyret P (2013) Total knee arthroplasty after high tibial osteotomy: a comparison of opening and closing wedge osteotomy. Int Orthop 37:427–431
Bergenudd H, Sahlstrom A, Sanzen L (1997) Total knee arthroplasty after failed proximal tibial valgus osteotomy. J Arthroplasty 12:635–638
Cerciello S, Vasso M, Maffulli N, Neyret P, Corona K, Panni AS (2014) Total knee arthroplasty after high tibial osteotomy. Orthopedics 37:191–198
Chen JY, Lo NN, Chong HC, Pang HN, Tay DK, Chin PL, Chia SL, Yeo SJ (2014) Cruciate retaining versus posterior stabilized total knee arthroplasty after previous high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3259-z
Coventry MB (1965) Osteotomy of the upper portion of the tibia for degenerative arthritis of the knee. A preliminary report. J Bone Joint Surg Am 47:984–990
Erak S, Naudie D, MacDonald SJ, McCalden RW, Rorabeck CH, Bourne RB (2011) Total knee arthroplasty following medial opening wedge tibial osteotomy: technical issues early clinical radiological results. Knee 18:499–504
Farfalli LA, Farfalli GL, Aponte-Tinao LA (2012) Complications in total knee arthroplasty after high tibial osteotomy. Orthopedics 35:e464–e468
Gupta H, Dahiya V, Vasdev A, Rajgopal A (2013) Outcomes of total knee arthroplasty following high tibial osteotomy. Indian J Orthop 47:469–473
Haddad FS, Bentley G (2000) Total knee arthroplasty after high tibial osteotomy: a medium-term review. J Arthroplasty 15:597–603
Hooper G, Leslie H, Burn J, Schouten R, Beci I (2005) Oblique upper tibial opening wedge osteotomy for genu varum. Oper Orthop Traumatol 17:662–673
Insall JN, Joseph DM, Msika C (1984) High tibial osteotomy for varus gonarthrosis. A long-term follow-up study. J Bone Joint Surg Am 66:1040–1048
Kawano T, Miura H, Nagamine R, Urabe K, Matsuda S, Mawatari T, Moro-Oka T, Iwamoto Y (2003) Alignment in total knee arthroplasty following failed high tibial osteotomy. J Knee Surg 16:168–172
Kazakos KJ, Chatzipapas C, Verettas D, Galanis V, Xarchas KC, Psillakis I (2008) Mid-term results of total knee arthroplasty after high tibial osteotomy. Arch Orthop Trauma Surg 128:167–173
Mason JB, Fehring TK, Estok R, Banel D, Fahrbach K (2007) Meta-analysis of alignment outcomes in computer-assisted total knee arthroplasty surgery. J Arthroplasty 22:1097–1106
McNamara I, Birmingham TB, Fowler PJ, Giffin JR (2013) High tibial osteotomy: evolution of research and clinical applications–a Canadian experience. Knee Surg Sports Traumatol Arthrosc 21:23–31
Meding JB, Wing JT, Ritter MA (2011) Does high tibial osteotomy affect the success or survival of a total knee replacement? Clin Orthop Relat Res 469:1991–1994
Nizard RS, Cardinne L, Bizot P, Witvoet J (1998) Total knee replacement after failed tibial osteotomy: results of a matched-pair study. J Arthroplasty 13:847–853
Orban H, Mares E, Dragusanu M, Stan G (2011) Total knee arthroplasty following high tibial osteotomy—a radiological evaluation. Maedica (Buchar) 6:23–27
Parvizi J, Hanssen AD, Spangehl MJ (2004) Total knee arthroplasty following proximal tibial osteotomy: risk factors for failure. J Bone Joint Surg Am 86-A:474–479
Preston S, Howard J, Naudie D, Somerville L, McAuley J (2014) Total knee arthroplasty after high tibial osteotomy: no differences between medial and lateral osteotomy approaches. Clin Orthop Relat Res 472:105–110
Ramappa M, Anand S, Jennings A (2013) Total knee replacement following high tibial osteotomy versus total knee replacement without high tibial osteotomy: a systematic review and meta analysis. Arch Orthop Trauma Surg 133:1587–1593
Treuter S, Schuh A, Honle W, Ismail MS, Chirag TN, Fujak A (2012) Long-term results of total knee arthroplasty following high tibial osteotomy according to Wagner. Int Orthop 36:761–764
van Raaij TM, Reijman M, Furlan AD, Verhaar JA (2009) Total knee arthroplasty after high tibial osteotomy. A systematic review. BMC Musculoskelet Disord 10:88
Walther M, Konig A, Kirschner S, Gohlke F (2000) Results of posterior cruciate-retaining unconstrained total knee arthroplasty after proximal tibial osteotomy for osteoarthritis. A prospective cohort study. Arch Orthop Trauma Surg 120:166–170
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M et al (1999) The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Ottawa, ON, Ottawa Health Research Institute
Windsor RE, Insall JN, Vince KG (1988) Technical considerations of total knee arthroplasty after proximal tibial osteotomy. J Bone Joint Surg Am 70:547–555
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
Additional information
Jae Hwi Han and Jae-Hyuk Yang contributed equally to this work as co-first authors.
Rights and permissions
About this article

Cite this article
Han, J.H., Yang, JH., Bhandare, N.N. et al. Total knee arthroplasty after failed high tibial osteotomy: a systematic review of open versus closed wedge osteotomy. Knee Surg Sports Traumatol Arthrosc 24, 2567–2577 (2016). https://doi.org/10.1007/s00167-015-3807-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3807-1