
Abstract
Background
Whether a previous high tibial osteotomy (HTO) influences the long-term function or survival of a total knee arthroplasty (TKA) is controversial.
Questions/purposes
We compared long-term functional scores and survival of bilateral TKAs in patients who had a previous HTO in one of the knees.
Patients and Methods
From 1980 to 1995, we performed 5043 primary TKAs; 39 of these patients had bilateral TKAs at an average of 8.7 years after unilateral HTO. Surgery was simultaneous in 32 patients and staged in seven. There were 12 women and 27 men with an average age of 66.9 years at the time of surgery. At last followup, 19 of the 39 patients were living and had been reevaluated since our previous study. We determined function with Knee Society scores. The length of followup for patients who had HTOs averaged 14 years (range, 3–21 years); for patients without HTOs, the average followup was 13.9 years (range, 3–22 years).
Results
We observed no differences in Knee Society function and radiographic and pain scores between the knees without and with previous HTO. Terminal extension and flexion, arc of motion, and knee alignment were similar between the knees. There were no femorotibial revisions in either group of knees. Survival at 15 years was 100% for knees without previous HTO and 97% for knees with previous HTO.
Conclusions
Our observations suggest a previous high tibial osteotomy does not influence the function or survival of a knee long term.
Level of Evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Controversy exists regarding the success of a TKA after a prior HTO [2–4, 6–13]. One might question whether failures would be greater in the long term as the HTO shortens the proximal tibia, the ligaments become lax and the proximal bone is more sclerotic. We previously reported 39 patients with bilateral TKAs who had one prosthesis implanted in a knee with a previous HTO [8]. At an average of 7 years after surgery, they were clinically and radiographically similar.
We have followed these patients an additional 7 years and again asked if the prior HTO makes a difference in the function after a TKA, and if there is a difference in prosthetic survivorship between these knees?
Patients and Methods
From 1980 to 1995, 5043 primary TKAs were performed at our institution. Of this group, 39 patients with previous unilateral closing wedge HTOs had bilateral, cemented TKAs. The osteotomies had been performed an average of 8.7 years (range, 2.0–15.4 years) before TKA. The original osteotomy failed in 28 of the 39 patients (72%) owing to recurrence of deformity; in the remaining 11 patients, the failure related to progressive osteoarthritis of the lateral compartment. There were 12 women and 27 men with an average age of 66.9 years at time of surgery. No patient was lost to followup. Twenty patients died, three in the first 7 years at the time of the first review [8] and 13 in the past 7 years. Thus, 19 of the 39 patients (49%) were alive. All had followups since the previous study. The followups for patients with HTOs averaged 14 years, (range, 3–21 years) and for patients without HTOs, 13.9 years (range, 3–22 years). No patients were recalled specifically for this study; all data were obtained from medical records and radiographs. This project (MV 102) was approved by our Institutional Review Board.
Both knees had the same posterior cruciate-retaining prosthesis implanted with the same surgical technique [8]. There were two important surgical concerns for the knee with a previous HTO. First, the patellar tendon may be fixed to the proximal tibia and theoretically is shorter. Great care must be taken to free it up to its original insertion and then protect it from being avulsed. Second, the proximal tibia has been shortened and therefore must be cut as thin as possible to expose cancellous bone for cementation of the tibial component and avoid a flexion and extension gap imbalance. Other important specific difficulties include the metadiaphyseal mismatch, ligament balancing in an original varus knee corrected to valgus, medial and lateral joint line level, and inverted tibial slope. Surgery was simultaneous in 32 patients and staged in seven at an average interval of 60 months (range, 10–97 months). Thirty-eight patients had an Anatomic Graduated Component (AGC; Biomet, Inc, Warsaw, IN, USA) implanted, and one had a posterior cruciate-retaining Posterior Cruciate Condylar Prosthesis (Howmedica; East Rutherford, NJ, USA). The data were collected prospectively and analyzed retrospectively.
Patients were followed at 2, 6, and 12 months and then every 2 years thereafter with clinical evaluations (ROM, extensor lag, and medial, lateral, and AP laxity) using the Knee Society clinical and radiographic scoring systems (standing AP and recumbent lateral and patellar views) preoperatively and postoperatively [1, 5].
Data were analyzed using the Wilcoxon signed-rank test (nonparametric paired test) and the paired t-test. The F-test was used to detect any differences in variance between knees that had HTOs and TKRs for equality of variance. Spearman and Pearson correlation coefficients were reported to evaluate the degree of correlation between paired knees. Survival analysis was performed using Kaplan-Meier survival analysis with failure defined as reoperation for any reason of the tibia or femur and excluding metallosis secondary to a metal-backed patella. Patients who died were censored at their death date. Statistical analysis was performed using SAS software program (SAS Institute, Cary, NC, USA).
Results
At latest followup, we observed no differences in the Knee Society scores for the knees without and with previous HTOs (Table 1). The pain scores were similar (p = 0.1252) between knees.
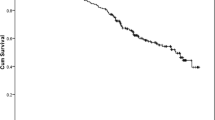
Kaplan–Meier survival at 15 years was 100% for knees without a previous HTO, and 97% for knees with a previous HTO. There were no new revisions attributable to failure as defined by loosening or wear since the last study. There was one new revision attributable to metallosis secondary to patella disassociation in a knee having a previous HTO. We have had no revisions of the femoral or tibial components.
Discussion
Concern remains regarding the results of a TKR after an HTO. Because of the difficulties doing a TKA after an HTO, we determined the function and survival of TKA in knees without and with previous HTOs.
Our study has some limitations. First is the sample size. As we had only 19 surviving patients, we found no difference in survival rates between the knees without and with previous HTOs. Given the limited power there is a possibility of a Type II error. However, as patients had one knee without and one with an osteotomy, the knee without the osteotomy served as an internal control, avoiding the variability that would occur if the knees without and with HTOs were in different patients. Second, some elements (eg, walking distance) of the Knee Society score are not independent variables [1, 5]. That is, they cannot be segregated for an individual knee, affect the function of both knees simultaneously, and cannot be distinguished in a statistical analysis. Other elements (eg, ROM) are independent but we did not separately analyze them in knees without and with previous HTOs. Third, owing to the retrospective nature of this investigation, we did not have a true control group, which would have been the group of patients electing to proceed with primary TKR despite being a candidate for tibial osteotomy. A true control group would have eliminated the high correlation between patients’ left and right knees in the statistical testing.
Our data suggest there is no difference in the function after a TKA, for patients with or without a prior HTO. Since our previous study [8] in 2000, numerous studies have reported on TKAs after HTOs with and without patient-matched comparisons [2–4, 6, 7, 9, 10, 12, 13]. Three studies without patient-matched comparisons concluded the outcome of TKAs after HTOs is inferior to that of TKAs without previous HTOs [7, 9, 10]. They all note the technically demanding nature of the procedure as the cause for the inferior results. Several patient-matched studies arrive at opposing conclusions from those of the aforementioned studies. Walther et al. [13], in a study of 35 patients, noted similar complications in both knees. They found extended hematomas more frequent in patients with previous HTOs. Postoperative knee scores were lower for patients with previous HTOs, but they observed no difference in function scores, ROM, or alignment. The study by Haddad and Bentley [3] included 50 knees in 42 patients with an average followup of 6.2 years. They found overall outcomes “good to excellent” for most patients with subtle clinical differences in their patient-matched comparison. Similarly, Huang et al. [4] concluded a previous HTO does not negatively affect the outcome of a TKA. The 17 knees followed at an average of 59.4 months had outcomes of 94% with excellent or good results and no differences in knee score, function score, or ROM [4]. van Raaij et al. [12] reported no differences between the knees in their patient-matched comparison with an average followup of 3.7 years. The final patient-matched studies also found HTOs do not have a negative effect on later TKAs [6].
As there were no femorotibial revisions, there seemed to be no major differences in the survivorship of a TKA in either group of knees. However, we reiterate we had limited power, so the finding should not be considered definitive.
In our previous study [8], we found the knee scores and survival for TKAs were similar for patients having a previous HTO and patients without a previous HTO. After analysis of the updated data, which included longer followup (with HTO, 14 years; without HTO, 13.9 years), we reached similar conclusions. Clinical scores were similar between knees, and survivorship for a TKA with previous HTO appears similar to that for patients having a TKA without previous HTO. Ranges of motion were similar for the two knees. Our observations suggest the concerns of diminished ROM and residual instability are not warranted. A TKA for patients having had an HTO appears to continue to provide the same outcomes as those for patients without a previous HTO.
References
Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989;248:9–12.
Gandhi R, Alomran A, Mahomed N. Bilateral non-union of high tibial osteotomies treated by total knee arthroplasty: a case report. Knee. 2008;15:242–245.
Haddad FS, Bentley G. Total knee arthroplasty after high tibial osteotomy: a medium-term review. J Arthroplasty. 2000;15:597–603.
Huang HT, Su JY, Su KN, Tien YC. Total knee arthroplasty after failed dome osteotomy. Kaohsiung J Med Sci. 2002;18:485–491.
Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989;248:13–14.
Kazakos KJ, Chatzipapas C, Verettas D, Galanis V, Xarchas KC, Psillakis I. Mid-term results of total knee arthroplasty after high tibial osteotomy. Arch Orthop Trauma Surg. 2008;128:167–173.
Madan S, Ranjith RK, Fiddian NJ. Total knee replacement following high tibial osteotomy. Bull Hosp Jt Dis. 2002–2003;61:5–10.
Meding JB, Keating EM, Ritter MA, Faris PM. Total knee arthroplasty after high tibial osteotomy: a comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am. 2000;82:1252–1259.
Noda T, Yasuda S, Nagano K, Takahara Y, Namba Y, Inoue H. Clinico-radiological study of total knee arthroplasty after high tibial osteotomy. J Orthop Sci. 2000;5:25–36.
Parvizi J, Hanssen AD, Spangehl MJ. Total knee arthroplasty following proximal tibial osteotomy: risk factors for failure. J Bone Joint Surg Am. 2004;86:474–479.
Ritter MA, Herbst SA, Keating EM, Faris PM, Meding JB. Patellofemoral complications following total knee arthroplasty: effect of a lateral release and sacrifice of the superior lateral geniculate artery. J Arthroplasty. 1996;11:368–372.
van Raaij TM, Bakker W, Reijman M, Verhaar JA. The effect of high tibial osteotomy on the results of total knee arthroplasty: a matched case control study. BMC Musculoskelet Disord. 2007;8:74.
Walther M, König A, Kirschner S, Gohlke F. Results of posterior cruciate-retaining unconstrained total knee arthroplasty after proximal tibial osteotomy for osteoarthritis: a prospective cohort study. Arch Orthop Trauma Surg. 2000;120:166–170.
Acknowledgments
We thank Drs. EM Keating, PM Faris, ME Berend, and RA Malinzak for their contributions to the patient surgery count of this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she has no commercial associations that poses a conflict of interest in connection with the submitted article.”
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Meding, J.B., Wing, J.T. & Ritter, M.A. Does High Tibial Osteotomy Affect the Success or Survival of a Total Knee Replacement?. Clin Orthop Relat Res 469, 1991–1994 (2011). https://doi.org/10.1007/s11999-011-1810-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-1810-5