
Abstract
Purpose
Bone tunnel creation techniques influence the 3-dimensional (3D) position of bone tunnels and graft-bending angle in anterior cruciate ligament (ACL) reconstruction. This study assessed graft-bending angle and 3D characteristics of femoral bone tunnels and compared them between outside-in (OI) and transportal (TP) techniques.
Methods
Participants comprised 64 patients who underwent anatomic double-bundle ACL reconstruction, allocated to OI and TP groups (n = 32 each). The graft orientation plane exhibiting the largest graft-bending angle at the femoral tunnel aperture with the knee in extension was reconstructed from CT data using 3D imaging software. In this plane, graft-bending angle was compared between the OI and TP techniques.
Results
Although positionings of the intra-articular apertures of the femoral and tibial bone tunnels were similar, several spatial parameters of bone tunnels differed between techniques. Graft-bending angles of both anteromedial and posterolateral bundles were significantly more acute with the OI technique than with the TP technique. On coronal-plane CT, angle of the bone tunnel axis relative to the distal condylar axis correlated negatively with graft-bending angle, while in the axial plane, angle of the bone tunnel axis relative to the posterior condylar axis correlated positively with graft-bending angle. Lysholm score, pivot shift test, and anteroposterior laxity at >2.5-year follow-up demonstrated no significant differences between techniques.
Discussion
Different bone tunnel directions in OI and TP techniques substantially affected graft-bending angle , despite similar positionings of the intra-articular apertures. Graft-bending angle with the OI technique was acute, but risk of posterior blowout of the lateral femoral condyle was decreased. Surgeons should create the femoral tunnel while considering an obtuse graft-bending angle without increasing the risk of posterior blowout.
Level of evidence
III.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In anterior cruciate ligament (ACL) reconstruction, the number of publications dealing with the outside-in (OI) technique for creating femoral bone tunnels has been increasing since retractable retrograde cutting instruments became more widely available [10, 17]. Compared with the inside-out transportal (TP) technique, the OI technique appears to offer several advantages for both single- and double-bundle ACL reconstructions, such as avoidance of posterior cortex blowout [11, 17]. However, one potential concern has been raised against the OI technique: acute graft-bending angle (GBA) with the knee in full extension has been documented in recent in vivo 3-dimensional (3D) analyses [11, 17]. To date, two cadaveric studies have reported potential adverse effects of acute GBA. The degree of graft deformity within the bone tunnel increased with increasing GBA, which substantially shifted the tunnel position anteriorly, even when placing the graft in the optimal position [6]. Segawa et al. [19] demonstrated that femoral tunnels with acute GBA resulted in high contact pressure at the anterior aspect of the tunnel throughout the range of motion, explaining bone tunnel enlargement in this direction. In addition, from the clinical perspective, repetitive bending stress on the graft at the femoral tunnel aperture may increase magnetic resonance imaging (MRI) signals of the graft in this region and is considered one of the causes of graft failure after ACL reconstruction [3, 12, 20, 22].
In the present study, 3D femoral tunnel characteristics of both the AMB and PLB were examined in patients undergoing anatomic double-bundle ACL reconstruction with the OI and TP techniques. GBA was also determined in vivo using computed tomography (CT) data from the patients, and a strategy to reduce GBA was based on the data from correlation analyses between GBA and spatial parameters for bone tunnel direction. The hypothesis of this study was that GBA would be larger with the OI technique than with the TP technique and would be affected by the 3D characteristics of the bone tunnel direction.
Materials and methods
Sixty-four of the 101 patients who underwent ACL reconstruction between 2011 and 2012 consented to undergo postoperative CT and met the inclusion criteria for this study (Table 1). As the OI technique was first applied in September 2011, the 32 patients treated before that time were allocated to the TP group, and 32 patients after that were allocated to the OI group. Inclusion criteria were as follows: primary ACL reconstruction with an anatomic double-bundle procedure using semitendinosus (ST) tendon; unilateral ACL rupture; and a postoperative follow-up period >1.5 years. Exclusion criteria comprised previous ligament reconstruction or multiple ligament injuries, and reconstruction with other substitutes such as bone patellar tendon bone autograft. Indeed, 19 revision ACL reconstructions and 11 selective bundle reconstructions (either AMB or PLB) were excluded. By 2 months postoperatively, all patients had achieved knee extension equal to the contralateral knee, including hyperextension or 0° extension, and underwent 1-mm helical CT. Knee joint in 0° extension was routinely confirmed using a scout view of the whole leg obtained prior to the CT examinations. As GBA was affected by knee flexion angle, a special knee support was used to keep the knee joint in 0° extension throughout CT examinations.
Surgical techniques
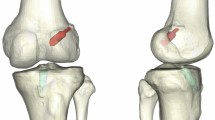
All ACL reconstructions were performed arthroscopically by a single surgeon, as reported previously [13, 14]. Briefly, ST tendon was harvested and cut into two pieces, and two double-looped ST tendons were prepared for AMB and PLB grafts. During femoral bone tunnel creation, our landmark for ideal AMB and PLB bone tunnels was the intercondylar ridge, which is reportedly identifiable in more than 97 % of human femora [4, 5]. Tunnels for the AMB and PLB were placed posterior to the ridge, and the centres of these tunnels corresponded to the centre of each anatomic footprint, including the fan-like portion [5, 8]. With the TP technique, two 2.4-mm guidewires were inserted into both the AMB and PLB attachments in an inside-out fashion through a medial accessory portal. The knee joint was flexed maximally during guidewire insertion. After 4.5-mm drilling was performed over the guidewire, a socket 15 mm in length was created by drilling with each tunnel diameter. With the OI technique, two ACL aimers were used and set for insertion angles of 100° (Arthrex, Naples, FL) or 0° (Smith & Nephew Endoscopy, Memphis, TN). The angle of the femoral tunnel in relation to the joint line was aimed at 50° for AMB and 40° for PLB in the axial plane (Fig. 1). A 3.5-mm guide pin was introduced from the lateral femoral cortex and replaced by a FlipCutter® (Arthrex), which in turn cut a socket into the femur to a depth of 15 mm. After tibial bone tunnel creation, grafts were introduced through the tibial tunnel into the femoral tunnel. Femoral fixation for the two ST tendon grafts was achieved using TightRope® (Arthrex). Tibial graft fixations were achieved using a double spike plate (Smith & Nephew Endoscopy). Both grafts for AMB and PLB were secured with 20 N each with the knee in 20° flexion using a ligament tensioner (Smith & Nephew Endoscopy).

In the OI technique, the OI-ACL aimer is set at an insertion angle of 50° for AMB and 40° for PLB in relation to the joint line with the knee in 90° of flexion
Measurement of bone tunnel position
In this study, 3D imaging software (ATHENA®; Soft Cube, Osaka, Japan) originally developed for preoperative planning of total knee arthroplasty was used to reconstruct an arbitrarily oriented imaging plane from CT data [21]. This software allows digital reconstruction of radiographs from CT data, simulating different radiographic source positions and angles. First, CT data for the entire femur and tibia were reconstructed into 3D models using the ATHENA® software. As consistent positioning of the intra-articular bone tunnel aperture was prerequisite for comparison of GBA between the OI and TP techniques, femoral and tibial bone tunnel positions were analysed. The coronal reference plane was defined as a plane including the centre of the femoral head and the tangential line connecting the most posterior points of the medial and lateral femoral condyles. The sagittal plane including the highest point of the intercondylar notch and the centre of the femoral head was made perpendicular to this coronal plane. A view of the medial wall of the lateral femoral condyle was set strictly parallel to this sagittal plane, and a rectangular measurement frame as reported by Bernard et al. [2] was applied to the image. Locations of the AMB and PLB tunnels were quantified and expressed as the percentage distance from the deepest subchondral contour and the intercondylar notch roof to the centre of each tunnel. In the analysis of tibial tunnel position, the sagittal reference plane was defined to include the following three points confirmed in the axial plane of the tibia: the talus centre; the medial one-third of the anterior spine; and the centre of the PCL footprint. Sagittal positions of each bone tunnel centre were assessed on sagittal images parallel to the reference plane and were expressed by dividing the distance from the anterior border of the tibia to the bone tunnel centre by the anteroposterior width of the tibia, in accordance with the methods described by Amis et al. [1].
Measurement of GBA
The graft-bending plane passing through the centres of the extra- and intra-articular apertures of the femoral tunnel and the centre of the intra-articular aperture of the tibial tunnel was made using ATHENA® (Fig. 2a). This plane included the largest GBA at the intra-articular aperture of the femoral tunnel with the knee in extension. The methodology of preparing graft-bending plane was the same as that reported by Wang et al. [23]. GBA was defined as the angle between the femoral bone tunnel axis and the line connecting each centre of the intra-articular apertures of the femoral and tibial bone tunnels (Fig. 2b), indicating the virtual ACL graft. The definition of GBA was the same as that reported by Nishimoto et al. [15]. As variables potentially affecting the GBA, bone tunnel length, angle to the PCA, angle to the distal condylar line, and angle of divergence of the AMB and PLB tunnels were determined. The 3D surface model was projected into the coronal and axial planes to measure the angle to the PCA and angle to the distal condylar line [18]. Two orthopaedic surgeons who were blinded to the tunnel drilling method measured GBA, bone tunnel length, angle to PCA, angle to distal condylar line, and angle of tunnel divergence on two separate occasions with an interval of 1 week. Intra- and inter-observer reliabilities were determined for each measurement using intra-class correlation coefficient (ICC) (Table 2).

a Graft orientation plane passing through the centres of the extra- and intra-articular apertures of the femoral tunnel and the centre of the intra-articular aperture of the tibial tunnel. b GBA is defined as the angle between the bone tunnel axis and the line connecting each centre of the intra-articular apertures of the femoral and tibial bone tunnels
All patients provided informed consent prior to enrolment, and all study protocols were approved by our institutional review board (Keio University, School of Medicine, ID #20100266).
Statistical analysis
Statistical analysis was performed using SPSS version 17.0 software (SPSS, Chicago, IL). Student’s t test was used to compare the following measurement between the two tunnel drilling techniques: patient demographics and postoperative clinical scores including age, time to operation, Tegner activity scale, Lysholm score; and bone tunnel parameters including GBA, femoral width, tunnel length, tunnel divergent angle, angle to PCA, and angle to distal condylar line. The Chi-square test was used to compare differences in sex, substitutes used, and type of combined treatment between the two tunnel drilling techniques. Pearson’s correlation coefficient test was used to determine the significance of associations among GBA and bone tunnel parameters including angle to PCA, angle to distal condylar line, and bone tunnel length. All tests were considered statistically significant for values of p < 0.05. Regarding intra-class reliability, measurement was considered reliable if the ICC was >0.80. Sample size for the current investigation was determined using the effect size of GBA of AMB obtained from the first 10 cases for each of the OI and TP groups. Twelve patients in each group were calculated to be required to demonstrate a difference with an alpha level of 0.05 and a statistical power of 80 %.
Results
No significant differences in bone tunnel positionings of the AMB or PLB were evident between the OI and TP techniques (Figs. 3, 4).

Distribution of sagittal bone tunnel positions of the femur with TP (a) and OI (b) techniques. Centres of the bone tunnel aperture are plotted and evaluated according to the quadrant technique described by Bernard et al.

Distribution of sagittal bone tunnel positions in the tibia with TP (a) and OI (b) techniques. Centres of bone tunnel apertures are plotted and evaluated based on the Amis-Jacob line
As a typical graft-bending plane in AMB demonstrates (Fig. 5), GBA was significantly larger with the OI technique than with the TP technique, representing a common trend for both AMB and PLB (p < 0.001, Table 3). Angles of bone tunnel axes in relation to the PCA for both AMB and PLB were significantly larger with the OI technique than with the TP technique. Bone tunnel length for AMB was significantly longer with the OI technique than with the TP technique.

Typical graft-bending plane of AMB created with TP (a) and OI (b) techniques. Larger GBA and longer bone tunnel are observed with the OI technique rather than with the TP technique
In correlation analyses of spatial parameters, angle of the bone tunnel axis relative to the distal condylar axis correlated negatively with GBA in the coronal plane for both techniques (Table 4). In the axial plane, the angle of the bone tunnel axis relative to the PCA showed a positive correlation with GBA, but this was only a trend with the TP technique. In terms of bone tunnel length, angle to the PCA in the axial plane correlated positively with the bone tunnel length for both AMB and PLB.
When assessing the clinical effects of bone tunnel creation technique and subsequent GBA, Lysholm score, rate of pivot shift test ≥glide, and anteroposterior laxity measured with KT-1000 demonstrated no significant difference between the two techniques (Table 5).
Discussion
The most important finding in this study was that GBAs for both AMB and PLB at the femoral tunnel aperture were significantly more acute in the OI technique than in the TP technique. Even though the positions of intra-articular aperture of the femoral and tibial bone tunnels were similar between OI and TP techniques, we noticed that the 3D characteristics of bone tunnels differed markedly between techniques, contributing to significant differences of GBA between techniques.
In ACL reconstruction, surgeons have increasingly been focusing on GBA, as 3D imaging modalities for bone tunnels have developed. Actually, in PCL reconstruction, concerns about acute GBA and bone tunnel enlargement have been raised, particularly for ‘killer turn’ and ‘critical corner’ at the tibial and femoral intra-articular bone tunnel apertures, respectively [7, 9]. Similarly in ACL reconstruction, impaired graft maturation or subsequent graft damage have been confirmed around the femoral tunnel aperture based on MRI and second-look arthroscopy [12, 16]. Based on our in vivo analysis, GBAs for both AMB and PLB were significantly larger with the OI technique than with the TP technique. A large GBA indicates that the graft is acutely bent and stretched at the femoral bone tunnel aperture. To date, several advantages to the OI technique have been put forward, such as a low incidence of posterior wall blowout of the lateral femoral condyle, a lack of cartilage damage at the medial femoral condyle during drilling, and easy handling of cases with a narrow notch [11]. However, whether acute GBA in the OI technique actually impairs graft-healing and, if so, what the safe range is, remain unclear.
Arbitrary positioning of the extra-articular tunnel aperture and bone tunnel direction might be a strong technical advantage of the OI technique. Based on the correlation analysis of GBA with several bone tunnel parameters, strategies to control GBA may emerge. In terms of preventing blowout of the posterior condyle, maintaining a large angle of the bone tunnel axis relative to the PCA might be beneficial. In practice, we aimed to set this angle as 40° for PLB and 50° for AMB, relative to the joint line (Fig. 1). However, in the present cases, a weak positive correlation between angle to the PCA and angle to the distal condylar line was found, which might be attributable to the preferences of the surgeon. If the angle to the PCA exceeds 50° in the OI technique, the shape of the bone tunnel becomes elliptical, such that surgeons tended to fit the elliptically shaped tunnel to the ACL footprint by increasing the angle to the distal condylar line.
Compared to the OI technique, controlling bone tunnel direction and subsequent GBA is somewhat difficult in the TP technique. The tunnel direction can only be changed to some extent by controlling knee flexion angle during drilling of bone tunnel, but potential risks of posterior wall blowout at the lateral femoral condyle and cartilage damage at the medial femoral condyle may restrict tunnel direction. Nishimoto et al. [15] reported that knee flexion to 110° at the time of drilling with the TP technique minimized GBA, significantly smaller than that in the transtibial technique; but with such a flexion angle, posterior wall blowout may occur if the angle to the distal condylar line is intentionally increased to reduce GBA.
In terms of clinical outcome for the present ACL reconstruction series, the OI technique was comparable to the TP technique. The OI technique is likely to grow in popularity with the development of retrograde cutting instruments, but surgeons should be aware of the increased GBA in the OI technique and understand how to control GBA intra-operatively. One potential concern that has been raised is that if attempts are made to reduce GBA, the intra-articular aperture of the femoral bone tunnel takes a more elliptical shape. An elliptical shape of the tunnel easily causes bone tunnel coalition between the AMB and PLB in double-bundle ACL reconstruction, but is likely to cover the anatomic footprint of the ACL even with the single-bundle procedure.
Finally, some limitations must be taken into consideration when interpreting the present results. This study clarified the relationship between bone tunnel direction and GBA; however, whether and how much GBA reduction is needed for good postoperative outcome remains unknown. One can easily imagine that an acute GBA would concentrate stress at the edge of the tunnel aperture, resulting in tunnel enlargement and graft rupture according to the past in vitro studies [6, 19]. In contrast, obtuse GBA might impair graft-to-bone incorporation due to the so-called bungee effect. For the time being, no studies have demonstrated an effect of GBA on clinical outcomes. Although this study found comparable clinical outcomes in the two techniques with different GBAs, well-designed studies focusing on the effects of GBA on long-term clinical outcomes are warranted to precisely clarify the safe range for GBA.
In terms of the clinical relevance, the present study suggested that surgeons should create the femoral tunnel considering not only the anatomic positioning of the bone tunnel aperture, but also the bone tunnel direction and subsequent GBA, particularly in the OI technique.
Conclusion
Different bone tunnel directions in OI and TP techniques substantially affected GBA, despite similar positionings of the bone tunnel apertures. GBAs for both AMB and PLB were significantly more acute with the OI technique than with the TP technique.
References
Amis AA, Jakob RP (1998) Anterior cruciate ligament graft positioning, tensioning and twisting. Knee Surg Sports Traumatol Arthrosc 6:S2–12
Bernard M, Hertel P, Hornung H, Cierpinski T (1997) Femoral insertion of the ACL: radiographic quadrant method. Am J Knee Surg 10:14–21
Chhabra A, Kline AJ, Nilles KM, Harner CD (2006) Tunnel expansion after anterior cruciate ligament reconstruction with autogenous hamstrings: a comparison of the medial portal and transtibial techniques. Arthroscopy 22:1107–1112
Farrow LD, Chen MR, Cooperman DR, Victoroff BN, Goodfellow DB (2007) Morphology of the femoral intercondylar notch. J Bone Joint Surg Am 89:2150–2155
Ferretti M, Ekdahl M, Shen W, Fu FH (2007) Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthroscopy 23:1218–1225
Fujii M, Sasaki Y, Araki D, Furumatsu T, Miyazawa S, Ozaki T, Linde-Rosen M, Smolinski P, Fu FH (2014) Evaluation of the semitendinosus tendon graft shift in the bone tunnel: an experimental study. DOI, Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3461-z
Handy MH, Blessey PB, Kline AJ, Miller MD (2005) The graft/tunnel angles in posterior cruciate ligament reconstruction: a cadaveric comparison of two techniques for femoral tunnel placement. Arthroscopy 21:711–714
Hara K, Mochizuki T, Sekiya I, Yamaguchi K, Akita K, Muneta T (2009) Anatomy of normal human anterior cruciate ligament attachments evaluated by divided small bundles. Am J Sports Med 37:2386–2391
Huang TW, Wang CJ, Weng LH, Chan YS (2003) Reducing the “killer turn” in posterior cruciate ligament reconstruction. Arthroscopy 19:712–716
Kim JG, Wang JH, Ahn JH, Kim HJ, Lim HC (2013) Comparison of femoral tunnel length between transportal and retrograde reaming outside-in techniques in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 21:830–838
Kim JG, Wang JH, Lim HC, Ahn JH (2012) Femoral graft bending angle and femoral tunnel geometry of transportal and outside-in techniques in anterior cruciate ligament reconstruction: an in vivo 3-dimensional computed tomography analysis. Arthroscopy 28:1682–1694
Natsu-ume T, Shino K, Nakata K, Nakamura N, Toritsuka Y, Mae T (2001) Endoscopic reconstruction of the anterior cruciate ligament with quadrupled hamstring tendons. A correlation between MRI changes and restored stability of the knee. J Bone Joint Surg Br 83:834–837
Niki Y, Hakozaki A, Iwamoto W, Kanagawa H, Matsumoto H, Toyama Y, Suda Y (2012) Factors affecting anterior knee pain following anatomic double-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 20:1543–1549
Niki Y, Matsumoto H, Hakozaki A, Kanagawa H, Toyama Y, Suda Y (2011) Anatomic double-bundle anterior cruciate ligament reconstruction using bone-patellar tendon-bone and gracilis tendon graft: a comparative study with 2-year follow-up results of semitendinosus tendon grafts alone or semitendinosus-gracilis tendon grafts. Arthroscopy 27:1242–1251
Nishimoto K, Kuroda R, Mizuno K, Hoshino Y, Nagamune K, Kubo S, Yagi M, Yamaguchi M, Yoshiya S, Kurosaka M (2009) Analysis of the graft bending angle at the femoral tunnel aperture in anatomic double bundle anterior cruciate ligament reconstruction: a comparison of the transtibial and the far anteromedial portal technique. Knee Surg Sports Traumatol Arthrosc 17:270–276
Otsubo H, Shino K, Nakamura N, Nakata K, Nakagawa S, Koyanagi M (2007) Arthroscopic evaluation of ACL grafts reconstructed with the anatomical two-bundle technique using hamstring tendon autograft. Knee Surg Sports Traumatol Arthrosc 15:720–728
Park JS, Park JH, Wang JH, Oh CH, Hwang MH, Lee SH, Kim JG (2015) Comparison of femoral tunnel geometry, using in vivo 3-dimensional computed tomography, during transportal and outside-in single-bundle anterior cruciate ligament reconstruction techniques. Arthroscopy 31:83–91
Park SH, Moon SW, Lee BH, Chae SH, Ahn JH, Chang M, Wang JH (2015) The sagittal plane angle and tunnel-related complications in double-bundle anterior cruciate ligament reconstruction using the transportal technique: an in vivo imaging study. Arthroscopy 31:283–292
Segawa H, Koga Y, Omori G, Sakamoto M, Hara T (2003) Influence of the femoral tunnel location and angle on the contact pressure in the femoral tunnel in anterior cruciate ligament reconstruction. Am J Sports Med 31:444–448
Segawa H, Omori G, Tomita S, Koga Y (2001) Bone tunnel enlargement after anterior cruciate ligament reconstruction using hamstring tendons. Knee Surg Sports Traumatol Arthrosc 9:206–210
Tei K, Ishida K, Matsumoto T, Kubo S, Sasaki H, Shibanuma N, Akisue T, Nishida K, Kurosaka M, Kuroda R (2012) Novel image-matching software for postoperative evaluation after TKA. Orthopedics 35:e1711–e1715
Toritsuka Y, Shino K, Horibe S, Mitsuoka T, Hamada M, Nakata K, Nakamura N, Yoshikawa H (2004) Second-look arthroscopy of anterior cruciate ligament grafts with multistranded hamstring tendons. Arthroscopy 20:287–293
Wang JH, Kim JG, Lee DK, Lim HC, Ahn JH (2012) Comparison of femoral graft bending angle and tunnel length between transtibial technique and transportal technique in anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 20(8):1584–1593
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Niki, Y., Nagai, K., Harato, K. et al. Effects of femoral bone tunnel characteristics on graft-bending angle in double-bundle anterior cruciate ligament reconstruction: a comparison of the outside-in and transportal techniques. Knee Surg Sports Traumatol Arthrosc 25, 1191–1198 (2017). https://doi.org/10.1007/s00167-015-3761-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3761-y