
Abstract
Purpose
Females have a higher risk in terms of anterior cruciate ligament injuries during sports than males. Reasons for this fact may be different anatomy and muscle recruitment patterns leading to less protection for the cruciate- and collateral-ligaments. This in vitro study aims to evaluate gender differences in knee joint kinematics and muscle force during weight-bearing knee flexions.
Methods
Thirty-four human knee specimens (17 females/17 males) were mounted on a dynamic knee simulator. Weight-bearing single-leg knee flexions were performed with different amounts of simulated body weight (BW). Gender-specific kinematics was measured with an ultrasonic motion capture system and different loading conditions were examined.
Results
Knee joint kinematics did not show significant differences regarding anteroposterior and medial–lateral movement as well as tibial varus–valgus and internal–external rotation. This applied to all simulated amounts of BW. Simulating 100 N BW in contrast to AF50 led to a significant higher quadriceps overall force in female knees from 45° to 85° of flexion in contrast to BW 50 N. In these female specimens, the quadriceps overall force was about 20 % higher than in male knees being constant in higher flexion angles.
Conclusions
It is indicated by our results that in a squatting movement females compared with males produce higher muscle forces, suggesting an increased demand for muscular stabilization, whereas tibio-femoral kinematics was similar for both genders.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anatomic variations have been found between males and females concerning muscle thickness and strength [2], bone shape [9, 15] and passive knee joint stabillizers [1, 31] like the anterior cruciate ligament (ACL), which has an increased risk to be injured in females even in non-contact sports [11, 22]. The ACL of women was found to be smaller in diameter and more frail to rupture [4, 22, 23]. An increased Q angle and valgus motion during flexion [16] also can be of importance, because this might cause the ACL to impinge at the lateral border of the femoral notch and thus be injured [16, 39].
Hormonal and biomechanical risk factors have also been identified. Whereas fluctuation of sex hormones throughout the menstrual cycle is considered to influence higher laxity of collagen fibres including the ACL, this coherence has not been proven conclusively [5, 11, 29].
Neuromuscular factors like gender-specific muscle activation are thought to be important covariants in knee joint injury mechanism [3, 7, 10, 13, 17, 36, 39].
Since women demonstrate significant stronger quadriceps activation during eccentric contraction [7, 20] this may lead to ruptures of the ACL, which has been demonstrated by an in vitro study [8].
A consensus concerning this topic has not been reached. So far, no in vitro study has been performed to investigate gender specifics in tibio-femoral kinematics and quadriceps activation during a squatting movement, which is part of many sports activities and may be associated with ACL injuries.
Having performed two previous studies with different questions [22, 34], the purpose of the current study was to summarize additional unpublished data obtained with these studies in order to analyse whether gender has an influence on tibio-femoral kinematics under different simulated body weight utilizing a physiological load pattern. We also wanted to know whether the reported higher quadriceps activation is due to neuromuscular control or whether there can be found other reasons for this phenomenon, thus being able to help to reduce the number of ACL injuries in females. We hypothesized (a) gender neither has influence on knee joint kinematics in vitro nor (b) does it affect the total quadriceps force required to simulate a partial bodyweight during knee flexion.
Materials and methods
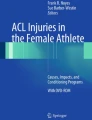
Kinematic and muscle force data of an overall number of 34 fresh frozen cadaveric knee specimens that partly have been used in other studies [24, 38] were analysed in order to compare knee kinematics and muscle load patterns of the quadriceps muscles for a knee squat. Seventeen female knees (age range 42–102 years) and 17 male knees (age range 58–91 years) could thus be compared. For technical reasons, only left knees were used. The knees were stored in airtight plastic bags at −20 °C. The femur and tibia were cut approximately 18–20 cm from the joint line, and all muscles were removed from the femoral and tibial bodies. All skin, muscle and other soft tissues were removed leaving only the intact joint capsule, quadriceps tendons, semimembranosus and biceps femoris. The proximal third of the fibula was fixed to the tibia via a bone screw. The ends of the tibia and femur were placed in an epoxy compound used for fixation to a knee simulator (Fig. 1), for technical details see Müller et al. [27].

Experimental set-up of the knee simulator. The coordinate systems for both tibia (solid) and femur (dashed) are shown. The ultrasonic motion capturing triad of the tibia segment is marked by an arrow as well as the tibia base, including the load cell for the vertical ankle force
Custom-designed stainless steel clamps were used to attach the quadriceps tendons (rectus femoris, vastus lateralis and vastus medialis), semimembranosus and biceps femoris to their respective motors for application of the dynamic quadriceps muscle forces and the static hamstrings forces. Knee flexions were performed driving the knee specimens in a force-controlled manner from nearly full extension to about 90° of flexion in vertical direction with a speed of 1°/s. In order to simulate a prescribed amount of body weight, the quadriceps and hamstrings muscle forces were generated by their respective motors to maintain a constant vertical ankle force, AF, measured by a load cell at the base of the tibia. The nominal static hamstrings force was 10 N. Since the real kinematic values of the knee movement has been determined after the flexion movement has finished as describe below, starting and finishing positions of the knee movement have been prescribed by default starting positions of the apparatus. In order not to hyperextend the cadaver knees while starting and not to overload in high flexion, the movement of every knee specimen was performed between 20° and 90° of flexion, taking into account that some of the specimens did not reach this end point because of size restrictions of the specimens.
The knee flexion kinematics was recorded by an ultrasonic motion capture system (ZEBRIS, Isny, Germany) with a sample rate of 1 Hz. Knee rotations and translations were defined by the paradigm of Grood and Suntay [12]. Motions were described by the orientation of the tibia coordinate system relative to the femur coordinate system. We adopted an Euler angle system (z–y–x sequence) to describe the orientation of the tibia relative to the femur. The knee coordinate system centres were placed at the mid-point between medial and lateral prominences of the tibial plateau. Both coordinate systems were defined to coincide at 0° flexion. The mediolateral (ML) axis was defined along a line connecting the medial and lateral prominences of the tibial plateau. The anteroposterior (AP) axis was defined as a line normal to a plane created by the flexion axis and a point along the length of each bone. The internal–external (IE) axis was then defined as a line normal to both ML and AP axes.
In all studies, each specimen was first flexed in an unloaded manner (i.e. without any muscle loads: AF0) and muscle-loaded knee movements were subsequently performed simulating knee flexion with 50 N (AF50) or 100 N (AF100) of ankle force, depending on the further measuring program of the respective study design. Some of the specimens were damaged by the high quadriceps loads due to the simulated ankle forces leading to a diminished number of specimens available for different parts of the studies. The number [n] of the utilized cadavers is indicated in each figure (Figs. 2, 3, 4, 5). As in recent studies, we performed every run with one repetition. Test–retest repeatability of the kinematic variables have shown to be 0.5° and 1 mm for rotation and translation, respectively [27, 37]. For quadriceps forces, we obtained test–retest repeatability of 5 N.

Flexion dependencies of the kinematic variables a femur anteroposterior movement, b femur medial–lateral movement, c tibia internal–external rotation and d tibia varus–valgus rotation for the two different gender groups as mean values + confidence intervals. Simulated ankle force 0 N

Flexion dependencies of the kinematic variables a femur anteroposterior movement, b femur medial–lateral movement, c tibia internal–external rotation and d tibia varus–valgus rotation for the two different gender groups as mean values + confidence intervals. Simulated ankle force 100 N. Asterisk indicates a p value ≤0.05

Summed quadriceps force and flexion angles for 50-N simulated ankle force (mean values + confidence intervals)

Summed quadriceps force and flexion angles for 100 N simulated ankle force (mean values + confidence intervals. Asterisk indicates a p value ≤0.05). The difference between the two curves between 45° and 80° is roughly 20 %
A custom-written program in MatLab (The MathWorks, Natick, MA, USA) processed the raw coordinate data of the capturing system in order to receive six measurement values, which describe the kinematics of the knee movement: knee flexion, varus–valgus rotation of the tibia, tibial internal rotation, femoral AP movement, ML movement and cranio-caudal movement. Each run was conducted twice. An interpolation routine made the measuring values equidistant in steps of 1° and averaged both runs. For reason of clarity, we present the results later on in diagrams with a spacing of 5°.
Statistical analysis
In order to compare kinematics of male and female knees, we present the flexion dependencies of the kinematic variables for the two different gender groups as mean values plus confidence intervals at each flexion value separately. A two-tailed t test revealed the hypothesized differences between the groups at every flexion step, which is highlighted by an asterisk for a p value ≤0.05.
Originating from two previous experiments the amount of specimens was not identical for all different measuring values we present in this study. All 34 specimens have been measured with the unloaded condition AF0. For the loaded conditions AF50 and AF100, not all specimens endured both measuring conditions. Thus, the number of specimens for the different measuring values is as follows:
-
Kinematics:
-
AF0: 17 male, 17 female
-
AF100: 6 male, 11 female
-
Muscle force:
-
AF50: 11 male, 8 female
-
AF100: 6 male, 11 female
As mentioned above, not all of the specimens reached the end positions of the whole flexion range (i.e. 20°–90°). Therefore, especially at these flexion angles, not all of the specimens could be used for statistics.
The research presented in this work conforms to the Helsinki Declaration and to local legislation. It has been approved by the Ethical Committee of the medical faculty of the University of Tübingen.
Results
Tibio-femoral kinematics
Tibio-femoral kinematics did not show significant differences regarding anteroposterior and medial–lateral movement as well as varus–valgus and tibial IE rotation. This applied to all simulated ankle force conditions (AF0, 50, 100). Solely at 70° of flexion, femur medial–lateral movement was significantly different in females compared with males (AF 100). Figure 2a–d presents the results of 17 male and 17 female specimens for AF0 showing almost identical curve progressions. Although not significant, for AF100, Fig. 3a–d illustrates that in male knee joints the femur moves more lateral, and tibial internal rotation is higher throughout the whole flexion range as well as the femur moves further posterior starting at 35° flexion angle. Females have a minimally elevated valgus rotation from 20° to 85° of flexion.
Quadriceps muscle force
During flexion, the quadriceps force to simulate a certain ankle force was rising in both male and female knee joints. AF100 in contrast to AF50 led to a significant higher quadriceps overall force in female knees from 45° to 85° of flexion (Figs. 4, 5). In this trial, the quadriceps overall force in female knees was about 20 % higher than in male knees with this relative surplus being constant in higher flexion angles (Table 1).
Discussion
The most important finding of the present study was that in a squatting movement females compared with males produce higher muscle forces, whereas tibio-femoral kinematics was similar for both genders. These findings are fortified by the large number of available specimen for data analysis, which is higher as is common practice for in vitro studies [6, 30, 35, 37, 40]. Zeller et al. [39] analysed the differences in kinematics between men and women during a single-legged squat, a movement similar to that in our set-up. They found a decreased ability of females to maintain a varus position during the squat as compared with the men. Varadarajan identified gender-specific rotational kinematics [32], Leszko et al. [21] found differences between Caucasian males and females concerning medial condyle translation and Biscevic et al. as well as Hollmann et al. [1, 14] identified a higher proportion of joint surface gliding in females during extension.
One other study confirms our findings. Johal et al. [19] performed a weight-bearing interventional MRI study and found the relative motion of tibia and femur during squatting to be independent of gender.
Since in cadaver studies neuromuscular regulations [13, 20, 28, 39] of kinematics are impossible, the different anatomy of males and females might explain our results, although anatomic variations of the specimens was not specifically investigated in the current study. Focusing specifically at the femur and tibia, only borderline sex-specific anatomic discrepancies were found [26]. Unequal anterior distal femur condyles were described by Fehring et al. [9], and since these are part of the patellofemoral joint, differences in patella tracking might occur.
From this perspective, we confirmed our first hypothesis. In the authors’ opinion and judging from the available literature, neuromuscular distinctions of movement control between genders as well as differences in ligamentous stabilizers of the knee joint are the main reasons for different knee joint kinematics in vivo.
With regard to muscle forces, our data indicate that with rising simulated body weight, there are significant gender differences. Many in vivo studies found higher quadriceps activation in females making the knee joint more vulnerable especially in low flexion angles where the ACL has its maximum tension and force absorption [25]. Since in our study there is no neuromuscular feedback possible and the anatomy of the distal femur and tibia are quite alike, our results have to be contributed to other factors.
One reason might be different anatomy of the quadriceps muscle and by these different attachment angles of the motor actuators. Not only the direct locus of clamp attachment but the whole extensor apparatus including patella, patellafemoral joint, the patellar-tendon and its origin at the tuberositas tibiae [33] can influence the necessary force to simulate a certain body weight. Higher patellofemoral forces induced by higher quadriceps load may be associated with the increased involvement of the female population in osteoarthritis of the knee joint [18].
Several limitations exist in the current study. First of all, we simulated only a partial body weight. This was because the quadriceps tendons in some of the specimens could not sustain the corresponding muscle forces resulting from higher body weight simulation. In order to avoid the risks of tendon rupture under high simulated muscle loading, we compromised to simulate only a portion of the body weight [34]. Moreover, previous investigation has shown that the change in the knee kinematics profile is not sensitive to the increasing simulated body weight [27]. Therefore, we believe that qualitative clinical insights can still be elucidated with the partially loaded knee. However, the results cannot definitely be extrapolated to predict the knee kinematics under full body weight. A second limitation in this study is that the knee flexion only started from 20°, because the joint could not be flexed from fully extended position by only applying a partial body weight and quadriceps force. This is due to the set-up of the knee kinemator control: since we drive the kinemator fully force controlled, the specimen might hyperextend and thus be destroyed if the extension angles reach below 20°. The information within first 15° of flexion is thus missing. A third limitation is the hamstring forces were kept constant during the simulated flexion. This is mainly because the multiple agonist and antagonist muscle forces composed a mechanically indeterminant system, and it is not likely to determine their individual contributions. We therefore believe the use of constant hamstring forces can isolate the effects of other factors without sacrificing the fidelity of the model.
The clinical relevance of this study is that female athletes might profit from special exercise to protect their knee joints during sports due to functional differences and higher need of active stabilization.
Conclusion
In conclusion, it is indicated by our results that in a squatting movement females compared with males produce higher muscle forces, suggesting an increased demand for muscular stabilization, whereas kinematics concerning anteroposterior and medial–lateral as well as IE and varus–valgus rotation was similar for both genders.
References
Biscevic M, Tomic D, Starc V, Smrke D (2005) Gender differences in knee kinematics and its possible consequences. Croat Med J 46:253–260
Blazevich AJ, Gill ND, Zhou S (2006) Intra- and inter-muscular variation in human quadriceps femoris architecture assessed in vivo. J Anat 209:289–310
Cammarata ML, Dhaher YY (2010) Evidence of gender-specific motor templates to resist valgus loading at the knee. Muscle Nerve 41:614–623
Chandrashekar N, Mansouri H, Slauterbeck J, Hashemi J (2006) Sex-based differences in the tensile properties of the human anterior cruciate ligament. J Biomech 39:2943–2950
Chaudhari AM, Lindenfeld TN, Andriacchi TP, Hewett TE, Riccobene J, Myer GD, Noyes FR (2007) Knee and hip loading patterns at different phases in the menstrual cycle: implications for the gender difference in anterior cruciate ligament injury rates. Am J Sports Med 35:793–800
Coobs BR, Wijdicks CA, Armitage BM, Spiridonov SI, Westerhaus BD, Johansen S, Engebretsen L, Laprade RF (2010) An in vitro analysis of an anatomical medial knee reconstruction. Am J Sports Med 38:339–347
Decker MJ, Torry MR, Wyland DJ, Sterett WI, Richard SJ (2003) Gender differences in lower extremity kinematics, kinetics and energy absorption during landing. Clin Biomech (Bristol, Avon) 18:662–669
DeMorat G, Weinhold P, Blackburn T, Chudik S, Garrett W (2004) Aggressive quadriceps loading can induce noncontact anterior cruciate ligament injury. Am J Sports Med 32:477–483
Fehring TK, Odum SM, Hughes J, Springer BD, Beaver WB Jr (2009) Differences between the sexes in the anatomy of the anterior condyle of the knee. J Bone Jt Surg Am 91:2335–2341
Gehring D, Melnyk M, Gollhofer A (2009) Gender and fatigue have influence on knee joint control strategies during landing. Clin Biomech (Bristol, Avon) 24:82–87
Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M, Dick RW, Engebretsen L, Garrett WE Jr, Hannafin JA, Hewett TE, Huston LJ, Ireland ML, Johnson RJ, Lephart S, Mandelbaum BR, Mann BJ, Marks PH, Marshall SW, Myklebust G, Noyes FR, Powers C, Shields C Jr, Shultz SJ, Silvers H, Slauterbeck J, Taylor DC, Teitz CC, Wojtys EM, Yu B (2006) Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med 34:1512–1532
Grood ES, Suntay WJ, Noyes FR, Butler DL (1984) Biomechanics of the knee-extension exercise. Effect of cutting the anterior cruciate ligament. J Bone Jt Surg Am 66:725–734
Hewett TE, Myer GD, Ford KR (2004) Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Jt Surg Am 86-A:1601–1608
Hollman JH, Deusinger RH, Van Dillen LR, Matava MJ (2003) Gender differences in surface rolling and gliding kinematics of the knee. Clin Orthop Relat Res 413:208–221
Hoshino Y, Wang J, Lorenz S, Fu FH, Tashman S (2011) Gender difference of the femoral kinematics axis location and its relation to anterior cruciate ligament injury: a 3D–CT study. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-011-1738-z
Hughes G, Watkins J, Owen N (2008) Gender differences in lower limb frontal plane kinematics during landing. Sports Biomech 7:333–341
Hurd WJ, Chmielewski TL, Axe MJ, Davis I, Snyder-Mackler L (2004) Differences in normal and perturbed walking kinematics between male and female athletes. Clin Biomech (Bristol, Avon) 19:465–472
Iriuchishima T, Ryu K, Aizawa S, Yorifuji H, Shirakura K (2012) Evaluation of the prevalence, lesion, and depth of osteoarthritic changes in the patella. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-012-1894-9
Johal P, Williams A, Wragg P, Hunt D, Gedroyc W (2005) Tibio-femoral movement in the living knee. A study of weight bearing and non-weight bearing knee kinematics using ‘interventional’ MRI. J Biomech 38:269–276
Landry SC, McKean KA, Hubley-Kozey CL, Stanish WD, Deluzio KJ (2007) Neuromuscular and lower limb biomechanical differences exist between male and female elite adolescent soccer players during an unanticipated side-cut maneuver. Am J Sports Med 35:1888–1900
Leszko F, Hovinga KR, Lerner AL, Komistek RD, Mahfouz MR (2010) In vivo normal knee kinematics: is ethnicity or gender an influencing factor? Clin Orthop Relat Res 469:95–106
Lin CF, Gross M, Ji C, Padua D, Weinhold P, Garrett WE, Yu B (2009) A stochastic biomechanical model for risk and risk factors of non-contact anterior cruciate ligament injuries. J Biomech 42:418–423
Lipps DB, Oh YK, Ashton-Miller JA, Wojtys EM (2012) Morphologic characteristics help explain the gender difference in peak anterior cruciate ligament strain during a simulated pivot landing. Am J Sports Med 40:32–40
Lo J, Müller O, Dilger T, Wülker N, Wünschel M (2011) Translational and rotational knee joint stability in anterior and posterior cruciate-retaining knee arthroplasty. Knee 18:491–495
Lo J, Müller O, Wünschel M, Bauer S, Wülker N (2008) Forces in anterior cruciate ligament during simulated weight-bearing flexion with anterior and internal rotational tibial load. J Biomech 41:1855–1861
Malek IA, Moorehead JD, Abiddin Z, Montgomery SC (2009) The correlation between femoral condyle radii and subject height. Clin Anat 22:517–522
Müller O, Lo J, Wünschel M, Obloh C, Wülker N (2009) Simulation of force loaded knee movement in a newly developed in vitro knee simulator. Biomed Tech (Berl) 54:142–149
Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J (2005) The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med 33:197–207
Park HS, Wilson NA, Zhang LQ (2008) Gender differences in passive knee biomechanical properties in tibial rotation. J Orthop Res 26:937–944
Philippot R, Chouteau J, Testa R, Moyen B (2010) In vitro analysis of patellar kinematics: validation of an opto-electronic cinematic analysis protocol. Knee Surg Sports Traumatol Arthrosc 18:161–166
Rozzi SL, Lephart SM, Gear WS, Fu FH (1999) Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med 27:312–319
Varadarajan KM, Gill TJ, Freiberg AA, Rubash HE, Li G (2009) Gender differences in trochlear groove orientation and rotational kinematics of human knees. J Orthop Res 27:871–878
Varadarajan KM, Gill TJ, Freiberg AA, Rubash HE, Li G (2010) Patellar tendon orientation and patellar tracking in male and female knees. J Orthop Res 28:322–328
Varadarajan KM, Harry RE, Johnson T, Li G (2009) Can in vitro systems capture the characteristic differences between the flexion-extension kinematics of the healthy and TKA knee? Med Eng Phys 31:899–906
Victor J, Labey L, Wong P, Innocenti B, Bellemans J (2010) The influence of muscle load on tibiofemoral knee kinematics. J Orthop Res 28:419–428
Wojtys EM, Huston LJ, Schock HJ, Boylan JP, Ashton-Miller JA (2003) Gender differences in muscular protection of the knee in torsion in size-matched athletes. J Bone Jt Surg Am 85:782–789
Wünschel M, Leichtle U, Obloh C, Wülker N, Müller O (2011) The effect of different quadriceps loading patterns on tibiofemoral joint kinematics and patellofemoral contact pressure during simulated partial weight-bearing knee flexion. Knee Surg Sports Traumatol Arthrosc 19:1099–1106
Wünschel M, Müller O, Lo J, Obloh C, Wülker N (2010) The anterior cruciate ligament provides resistance to externally applied anterior tibial force but not to internal rotational torque during simulated weight-bearing flexion. Arthroscopy 26:1520–1527
Zeller BL, McCrory JL, Kibler WB, Uhl TL (2003) Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Am J Sports Med 31:449–456
Zhu Z, Ding H, Dang X, Tang J, Zhou Y, Wang G (2010) In vitro kinematic measurements of the patellar tendon in two different types of posterior-stabilized total knee arthroplasties. Conf Proc IEEE Eng Med Biol Soc 1:3938–3941
Acknowledgments
We thank Smith and Nephew for the financial support.
Conflict of interest
The presented study was partly funded by Smith and Nephew.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wünschel, M., Wülker, N. & Müller, O. Gender differences in tibio-femoral kinematics and quadriceps muscle force during weight-bearing knee flexion in vitro. Knee Surg Sports Traumatol Arthrosc 21, 2557–2563 (2013). https://doi.org/10.1007/s00167-012-2082-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2082-7