
Abstract
The aim of this study was to compare the alteration of patellar tracking by time, which was performed through two different approaches: midvastus and medial parapatellar. Twenty-one patients undergoing simultaneous bilateral primary total knee replacements were randomized prospectively to perform the surgery via a medial parapatellar approach on one knee and midvastus approach on the other knee. All of the patellae were resurfaced. Preoperative, early and late postoperative (mean 22 month) skyline views of the patellae were taken. We found that preoperative 2.24° lateral tilt of patella had not changed by time at the midvastus side (2.95° and 2.57°). Moreover, preoperative 0.48% lateral subluxation of the patella for midvastus approach had not changed (1.48% and 1.67%). Although 2.19° patellar lateral tilt had not significantly changed at the early postoperative period, which was performed via medial parapatellar approach, there had been a significant increase to 5.38° by time (P=0.037) compared to the preoperative radiographs. Additionally, the preoperative lateral subluxation of the patella (0.57%) at the medial parapatellar side had increased to 5.43% at the early (P=0.009) and 5.62% at the late (P=0.012) postoperative measurements. Midvastus approach is superior to medial parapatellar approach concerning the late patellar tracking.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Proper patellar tracking is crucial for a total knee arthroplasty to function well. Abnormal patellar tracking can lead to diminished range of motion, anterior knee pain, overloading the polyethylene and abnormal implant wear [12, 17]. Patellar tilt angle and displacement can worsen during the long-term postoperative period, which was made with medial parapatellar (MPP) approach [13, 16]. The midvastus (MV) approach, which was popularized by Engh for the last decade, had some potential advantages about patellar tracking and lateral retinacular release rates [6, 15, 19]. However, there is not enough data concerning the time-dependent alteration of patellar tilt and congruence with MV approach. The purpose of this prospective randomized controlled study was to document the changes in patellar tracking by time comparing the MV and MPP approaches in a series of one-stage bilateral total knee replacements.
Material and methods
From October 2001 to October 2002, 21 patients (42 knees) undergoing simultaneous bilateral cemented primary total knee replacements were prospectively randomized to perform the surgery via a MPP approach on 1 knee and MV approach on the other knee. The average age of the patients was 67 years (range 53–73). There were one male and 20 female patients. Selection criteria for this study included primary diagnosis of osteoarthritis, varus deformity, almost the same grade arthrosis and same degree preoperative range of motion for both knees of the same patient. Total knee arthroplasty system used in this study were posterior cruciate ligament (PCL)-stabilized knee design in 18 knees of nine patients and PCL-retaining design in 24 knees of twelve patients (Genesis II, Smith& Nephew, Memphis, TN, USA). The same instrumentation was used in both knees of the same patient individually. Two surgeons performed all of the surgical procedures. Both knees of the same patient were operated by the same surgeon. Femoral neutral bone cuts were made with the anterior referencing cutting guides (without externally rotating the cutting blocks). All of the patellae were resurfaced with dome shaped polyethylene patellar component. Patellae were prepared by means of a patellar clamp with a reamer guide to obtain precise reaming. Ridges were cut by an oscillating saw. Patellar thickness was measured with a caliper before resection and an effort was made to reproduce the original patellar thickness. Medially positioned onset cemented fixation of the patellar button was performed. Same size implants were used for both knees. Both knees of two patients needed lateral retinacular release.
Preoperative skyline views of the patellae were taken with the knee in approximately 30° flexion using the technique of Laurin et al. [14]. Postoperative radiographs were taken at the sixth week and finally at the mean twenty-second month of the operation (range 13–28 month).
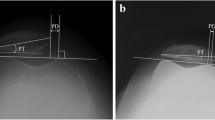
Lateral tilt of the patella was measured and patellar congruency was calculated by a blinded observer at the preoperative and early and late postoperative radiographs. The preoperative lateral tilt of the patella was defined as the angle between a line drawn from the anterior limits of the femoral condyles and a line drawn from the posterior limits of the articular surfaces of the medial and lateral facets of the patella [2]. The postoperative lateral tilt angle (Fig. 1) was defined as the angle between a line from the anterior limits of the femoral condyles and a line drawn through the patellar prosthesis-bone interface [8]. Patellar congruency (Fig. 2) was calculated as a percentage, which was a modification of the system described by Keblish et al. [11]. (The calculated value was subtracted from 100 to facilitate the statistical calculations and this final value was the percentage of subluxation). For the tilt and tracking, negative values indicated medial, positive values indicated lateral bending or subluxation of the patella.

Postoperative lateral tilt of the patella is the angle between a line from the anterior limits of the femoral condyles and a line drawn through the patellar prosthesis-bone interface [9]

Method of measuring patello-femoral congruency adapted from Keblish et al. [11]. 100 − [(B′D′/A′B′) × 100] = percentage of patellar subluxation (negative for medial and positive for lateral subluxation of the patella)
Statistical significance of the preoperative and postoperative values about the tilt degree and tracking percentage were analyzed by using Mann–Whitney U test and Wilcoxon sign test.
Results
The preoperative patellar tilt and congruency of right/left knees and MPP/MV sides had no significant differences (P>0.05) as shown in Table 1.
Radiographic measurements for the two groups were summarized in Table 2 and Figs. 3 and 4. The tilt angles at the early postoperative period for the two approaches were not significantly different (P=0.899). However, at the late postoperative period, lateral tilting of the patella was significantly higher for MPP group compared with the MV group (P=0.038). Nevertheless, the patellae showed a significant lateral subluxation for MPP group both at the early (P=0.024) and late postoperative periods (P=0.029) compared with the MV group.

Time dependent changes of patellar lateral tilt with two different approaches. Lateral tilt of the patella had significantly increased at the medial parapatellar approach side

Changes at the patello-femoral congruency. Medial parapatellar approach group had significant postoperative lateral subluxation
Furthermore, the preoperative tilt of the patella was compared with early and late postoperative values within the groups. Tilting of the patella was not significantly different for MPP group at the early postoperative measurements compared to the preoperative values (P=0.418). On the other hand, this value significantly deteriorated at the late postoperative period (P=0.037). Lateral tilting of the patella for MV group did not significantly alter at the early (P=0.359) and late postoperative periods (P=0.672) compared to the preoperative values.
The preoperative congruence of the patella was also compared with early and late postoperative values. The patellae significantly shifted laterally for MPP group at the early (P=0.009) and late postoperative measurements (P=0.012) compared to the preoperative values. On the other hand, there was not a significant difference at the congruence of the patella for MV group at the early (P=0.646) and late postoperative period (P=0.484) compared to the preoperative values.
Discussion
Proper patellar tracking and alignment is a major constituent of a well-functioning total knee replacement. To centralize the patella in the trochlear groove, a parapatellar release might be required [12]. On the other hand, this procedure may interrupt patellar blood supply and may cause many patellar complications secondary to avascularity like stress fracture [1, 9, 18]. MV approach offers some distinct benefits over the MPP approach. The most accepted advantage of this approach is preservation of the majority of the extensor mechanism. As a result, MV approach improves patellar tracking [4], and decreases the need for lateral retinacular release [5, 6, 15, 19].
It was reported that postoperative tilt angle and displacement of the patella had not remained at the same position. Lateral tilt of the patella can increase and displacement can worsen during the long-term postoperative period [13, 16]. Although there are some reports about the patellar tracking comparing the MPP and MV approaches, we are unaware of any report on the patellar tracking changes by time, which was performed with MV approach.
In this study, the tilt angles at the early postoperative period, for the two approaches, were not different. The real advantage of MV approach on patello-femoral tilt angle was obvious at the late postoperative period. Lateral tilt of the patella, which was performed with MPP approach, was increasing by time. It was shown in an experimental model of flexor tendon repair that in the rehabilitation period, there may be a gap formation and elongation in the repair side of the tendon [7]. We think that this increase in the MPP approach knees may be explained by the loosening of the repaired medial quadriceps tendon during rehabilitation. On the other hand, as the quadriceps tendon was not damaged during the surgery with MV approach, we could not observe any time dependent change in the patellar tilt. However, there was not any significant change on patellar tilt angle by time, which was made with MV approach.
Similarly, MV approach was also advantageous on patellar subluxation both in the early and late postoperative periods. Patella was tended to preserve its preoperative position. However, there was an obvious lateral displacement of the patella, which was made with MPP approach.
In this study, we used two type of prosthesis: PCL-stabilized and PCL-retaining design. As the selection criteria was almost the same grade arthrosis and same degree preoperative range of motion for both knees of the same patient, same type of implantation was performed for both knees in an individual patient. In the literature, it was shown that patellofemoral loading characteristics were not statistically different for PCL-stabilized and PCL-retaining design prostheses until 60°, it was expected that these variables will not change our results [3]. Since the femoral component design of the prosthesis used, in this study (Genesis II), had an anatomic lateralized trochlear groove design, the results obtained in this study may not be generalized for all type of arthroplasties. This study design was constructed on the fact of abnormal patellar tracking may lead to overloading the polyethylene and abnormal implant wear. Because of that we only included the patients whose patellae were replaced. It is also impossible to generalize the results to the patients whose patella was not replaced. We used Laurin’s technique to have the skyline views of the patella to measure the patellar tilt and congruency. However, it was reported that patellar subluxation can be detected more accurately by using computed tomography with the knee in full extension than by using conventional axial roentgenograms [10]. This was also the weakness of this study.
The results of the current study suggested that patellar lateral tilt increased by time, which was performed by MPP approach, while tilt of patella was not changed by time in the MV side. Patelo-femoral congruency did not change with MV approach even at the late postoperative period. However, the patella tended to subluxate laterally at the MPP side both at the early and late postoperative measurements.
References
Cameron HU, Huffer B (1985) Avascular necrosis of the patella following total knee replacement. Acta Orthop Belg 51:805–810
Chan KC, Gill GS (1999) Postoperative patellar tilt in total knee arthroplasty. J Arthroplasty 14:300–304
Churchill DL, Incavo SJ, Johnson CC, Beynnon BD (2001) The influence of femoral rollback on patellofemoral contact loads in total knee arthroplasty. J Arthroplasty 16:909–918
Cooper RE Jr, Trinidad G, Buck WR (1999) Midvastus approach in total knee arthroplasty: a description and a cadaveric study determining the distance of the popliteal artery from the patellar margin of the incision. J Arthroplasty 14:505–508
Dalury DF, Jiranek WA (1999) A comparison of the midvastus and paramedian approaches for total knee arthroplasty. J Arthroplasty 14:33–37
Engh GA, Parks NL, Ammeen DJ (1996) Influence of surgical approach on lateral retinacular releases in total knee arthroplasty. Clin Orthop 331:56–63
Gelberman RH, Boyer MI, Brodt MD, Winters SC, Silva MJ (1999) The effect of gap formation at the repair site on the strength and excursion of intrasynovial flexor tendons. An experimental study on the early stages of tendon-healing in dogs. J Bone Joint Surg Am 81:975–982
Gomes LS, Bechtold JE, Gustilo RB (1988) Patellar prosthesis positioning in total knee arthroplasty. A roentgenographic study. Clin Orthop Nov (236):72–81
Holtby RM, Grosso P (1996) Osteonecrosis and resorption of the patella after total knee replacement: a case report. Clin Orthop 328:155–158
B: Inoue M, Shino K, Hirose H, Horibe S, Ono K (1998) Subluxation of the patella. Computed tomography analysis of patellofemoral congruence. J Bone Joint Surg Am 70:1331–1337
Keblish PA, Varma AK, Greenwald AS (1994) Patellar resurfacing or retention in total knee arthroplasty. A prospective study of patients with bilateral replacements. J Bone Joint Surg Br 76:930–937
Laskin RS (2001) Lateral release rates after total knee arthroplasty. Clin Orthop 88–93
Laughlin RT, Werries BA, Verhulst SJ, Hayes JM (1996) Patellar tilt in total knee arthroplasty. Am J Orthop 25:300–304
Laurin CA, Levesque HP, Dussault R, Labelle H, Peides JP (1978) The abnormal lateral patellofemoral angle: a diagnostic roentgenographic sign of recurrent patellar subluxation. J Bone Joint Surg Am 60:55–60
Maestro A, Suarez MA, Rodriguez L, Guerra C, Murcia A (2000) The midvastus surgical approach in total knee arthroplasty. Int Orthop 24:104–107
Miyagi T, Matsuda S, Miura H, Nagamine R, Urabe K, Inoue S, Iwamoto Y (2002) Changes in patellar tracking after total knee arthroplasty: 10-year follow-up of Miller–Galante I knees. Orthopedics 25:811–813
Rader CP, Lohr J, Wittmann R, Eulert J (1996) Results of total knee arthroplasty with a metal-backed patellar component. A 6-year follow-up study. J Arthroplasty 11:923–930
Wetzner SM, Bezreh JS, Scott RD, Bierbaum BE, Newberg AH (1985) Bone scanning in the assessment of patellar viability following knee replacement. Clin Orthop 199:215–219
White RE Jr, Allman JK, Trauger JA, Dales BH (1999) Clinical comparison of the midvastus and medial parapatellar surgical approaches. Clin Orthop 367:117–122
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ozkoc, G., Hersekli, M.A., Akpinar, S. et al. Time dependent changes in patellar tracking with medial parapatellar and midvastus approaches. Knee Surg Sports Traumatol Arthrosc 13, 654–657 (2005). https://doi.org/10.1007/s00167-004-0605-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-004-0605-6