
Abstract
This paper develops an overlapping generations model that links a public health system to a pay-as-you-go (PAYG) pension system. It relies on two assumptions. First, the health system directly finances curative health spending on the elderly. Second, public pensions partially depend on health status by introducing a component indexed to society’s average level of old-age disability. Reducing the average disability rate in the economy then lowers pension benefits as the need to finance long-term care services also drops. We study the effects of introducing such a ‘comprehensive’ Social Security system on individual decisions, capital accumulation, and welfare. We first show that health investments can boost savings and capital accumulation under certain conditions. Second, if individuals are sufficiently concerned with their health when old, it is optimal to introduce a health-dependent pension system, as this will raise social welfare compared to a system where pensions are not tied to the society’s average level of old-age disability. Our analysis thus highlights an important policy recommendation: making PAYG pension schemes partially health-dependent can be beneficial to society.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Because of impressive health care improvements over the last fifty years, longevity has risen substantially in all developed countries. This has not come without policy challenges, however. In 2019, more than two out of five EU individuals aged 65 or older reported having some kind of functional limitation (Eurostat 2023). These can range from sensory, physical, and mental limitations to limitations in personal care and household activities, and they dramatically increase with age. In many OECD countries the importance of long-term care (LTC) has therefore grown — and will continue to grow — together with its costs (Siciliani 2013).Footnote 1
Different solutions have been discussed over the years to guarantee sufficient financial leeway for the elderly in case they become dependent. One solution would be to incentivize the purchase of private LTC insurance, but this has been shown to be relatively ineffective. Individuals often fail to insure themselves against the risk of becoming dependent at a later age, despite the substantial costs associated with the loss of autonomy.Footnote 2 A second solution would be to let the family take care of their elderly through either formal (in cash) or informal (in time) care, but this may come at the expense of a reduced labour supply of informal caregivers, higher psychological costs, and possibly lower aggregate welfare.
The last solution, which is the one we explore in this paper, is to let the government provide financial support to the elderly when they become dependent. More specifically, we propose a ‘comprehensive’ Social Security system that combines a health system and a pension system, which are closely interconnected. On the one hand, the government invests in public health to reduce the dependency rate of the elderly. On the other hand, pension benefits are partially indexed to society’s average level of old-age disability.Footnote 3 We thus extend the standard Diamond (1965) overlapping generations (OLG) model by ‘augmenting’ the universal Pay-As-You-Go (PAYG) pension benefit with a component that is health-dependent. We will call it the ‘disability-augmented’ pension benefit. This modulation of the pension system partially ties pension benefits to health status and compensates the elderly for spending more on costly LTC services in case they would grow more dependent.
We are interested in such a comprehensive Social Security system because it offers three advantages when investing in the elderly’s health. First, better health will reduce the average disability rate in the economy and hence directly increase individual welfare. Second, for a given average longevity, better health decreases financial pressure on the social security system. This is because when old-age dependency is reduced, our comprehensive system allows pension benefits to follow suit since the need to finance long-term care services decreases. Third, we show that when the level of health taxation is not too high, this process can boost saving for old age as pension contribution rates decrease. This can then spark off a general equilibrium effect that nudges up capital accumulation, growth, and wages. As a result, combining all three previous effects, we find that the introduction of a comprehensive Social Security system improves aggregate welfare when people are sufficiently concerned about their health in old age.
Importantly, since the health care pillar of our comprehensive system aims to directly reduce the dependency rate of the elderly, we focus on curative health spending to improve the quality of elderly life. A few examples are building nursing homes, promoting the education of qualified nurses, providing more day-to-day care, medications and therapies, and extending other existing medical services. In a recent report, the OECD (2021) indicates that a vast majority of public health spending is directed toward curative care rather than disease prevention and health promotion. In particular, curative and rehabilitative care services account for 60% of total health spending in OECD countries through inpatient and outpatient treatments (see Figure 7.15 in the OECD report).
Overall, our modelling of a comprehensive Social Security system offers a more encouraging outlook for the future of social protection in general and pension systems in particular. Indeed, in many countries facing the consequences of population ageing, public discourse often spreads the idea that health improvements are one of the reasons why PAYG pension systems are under pressure.Footnote 4 However, our results suggest that, quite logically, investing in curative health care improves the health status of the elderly and reduces the need for additional LTC spending. In turn, the introduction of health-dependent pension benefits can boost saving for old age and ultimately increase overall welfare. This paper thus aims to show how public health investments targeted toward the elderly may be useful in designing more efficient pension schemes.
More specifically, our model features a representative individual who lives two periods of fixed length with certainty. He derives his utility from consumption in both periods and from being healthier during old age. In the first period, he works and contributes to the health system, as well as to the Social Security system. He also saves for old-age consumption. In the second period, he consumes the proceeds of his savings and the pension benefit. Public intervention is twofold. First, using the health contributions, the government invests in public health by making curative expenditures. Contributions of workers in a given period are directly invested to increase the health condition of the old in the same period, and this directly increases the elderly’s utility since they value better health during old age. Second, individuals contribute to a PAYG pension system in the first period and receive a pension benefit in the second. As already mentioned, we will model an augmented version of a standard pension system by allowing the amount of the pension benefit to be tied to the average level of old-age disability in the economy. If health during old age deteriorates (equivalently, the intensity of dependency is higher in society), the elderly will receive higher pension benefits to cope with extra LTC expenditures.
Before going further, let us note that we abstract from the potential impact of health investment on increased longevity, which in turn would affect the pension budget constraint. In this way, we focus exclusively on the consequences of improved health of the elderly, regardless of lifespan changes. To our knowledge, no other study considers the effect of curative (rather than preventive) health investments on capital accumulation and welfare and models a health-dependent PAYG pension scheme. To do so, however, we had to shut down other channels. We believe that studying the effect of curative health spending together with health-dependent pensions is sufficiently novel to study it in isolation.
To analyze our comprehensive system in a context that would match reality more closely, we first run an analysis assuming that Social Security tax rates are close to those observed in OECD countries and look at how higher public health spending impacts health and capital accumulation. Second, we fix a minimum PAYG pension contribution and find the optimal levels of both the public health tax and the additional Social Security tax rate, which would finance the disability-augmented part of the pension benefit. We further study the welfare effects of introducing a disability-augmented component to the pension benefit. Importantly, we relate the optimal tax rate levels and the welfare effects to the individual preference for being healthier during old age.
Our main results are twofold. First, we show that, if the Social Security contribution rates match those observed in OECD countries, higher public health expenditures foster capital accumulation and growth as long as the contribution rate to the health system is not too large. This is the result of two opposing forces. On the one hand, increasing the health tax increases average health (i.e. decreases average disability) so it decreases pension benefits in the second period, and thus increases the willingness to save for old age to smooth consumption across periods. On the other hand, a higher health tax decreases disposable income and thus, savings. If the health tax is not too large, the first effect dominates the second: savings increase, and so do capital and output per capita.
Our second contribution concerns the welfare effects of introducing a disability-augmented pension benefit. We show that if individuals are sufficiently concerned with their health during old age, it is welfare-improving to introduce a system where pensions are tied to society’s average level of old-age disability, as compared to a standard system where this is not the case. In addition, as the individual’s preference for health increases, the welfare gains of augmenting the PAYG system become larger.
Relating these findings with what we observe in reality, it is reasonable to think that in the last decades, individuals have become more concerned with their health as a consequence of first, population ageing (and with it, an increasing probability of becoming dependent) and second, of our economies becoming richer and more informed about health issues. Our results indicate that it could indeed be welfare-improving to introduce a health-augmented pension system under these circumstances.
1.1 Related literature
By linking up the health system with the pension system, our interest in a comprehensive Social Security system also adds to the existing literature on two fronts.
First, since we investigate the effect of health investment on growth and welfare, we extend the findings of a strand of the literature that followed Chakraborty (2004).Footnote 5 He incorporates public health expenditures in an overlapping generation model (OLG) to endogenously determine longevity, finding that increased taxes for public health investments improve elderly survival chances and boost long-term capital accumulation. While the latter approach endogenises longevity through preventive health care investment, we endogenise health during old age through curative public investment. Our primary interest is therefore to determine to what extent a reduction in morbidity resulting from increased health investment can promote capital accumulation and economic growth. In this sense, our paper is the first to address the other side of the coin of health care investment. In doing so, moreover, we examine the interaction between public health programs and PAYG pension systems, demonstrating how their combined design influences capital accumulation, growth and ultimately welfare. This aspect has not been explored in the existing OLG literature.Footnote 6
Second, our proposed indexation of PAYG pension benefits to the old-age health status adds to the many studies on rising LTC ageing costs and their impact on social welfare. Most of the existing literature has concentrated on the reasons behind the LTC insurance puzzle (see footnote 2), however, and relies on partial equilibrium models.Footnote 7 Our general equilibrium analysis of LTC needs and its potential impact on saving decisions and welfare is hence fairly novel, barring the following three contributions. Marchiori and Pierrard (2022) consider the link between endogenous health investment, saving, growth, LTC and welfare. They find that there is a need for public preventive health care to internalise the negative externalities of private under-investment. Kopecky and Koreshkova (2014) calibrate a life-cycle model where individuals face a risk on earnings, survival and LTC expenses, but can partially insure through public programs such as Medicaid and Social Security. They show that a large part of wealth is devoted to planning for old-age risks of survival and of needing LTC. They further show that all young generations would benefit from making these public programs more generous. Finally, Canta et al. (2016) study the dynamics of capital accumulation when individuals face a probability of becoming dependent during old age and when the existence of family norms can influence the level of informal care provided by the family. They allow for social insurance covering LTC risk but take it as given.
Differently from these papers, we model a public pension system in which any changes in old-age disability affect the pension benefits to be distributed and we focus on curative public health investment. Furthermore, we provide a normative analysis and show that introducing a health component in the pension benefit formula is welfare-improving. As such, we propose that both public programs should not be considered in isolation, contrary to what is mostly assumed in the above-cited literature. This, in a sense, also bridges the two strands of literature we discussed here.
The paper proceeds as follows. Section 2 presents the model and establishes the equilibrium. Section 3 describes the effect of a rise in health investment on steady-state capital accumulation. Section 4 combines our findings to shed light on the potential welfare ramifications brought about by the kind of mixed pension system we propose. Section 5 concludes.
2 The model
We consider a closed economy populated by a continuum of perfectly foresighted and identical individuals whose lifespan is finite and divided into two periods: youth (the working period) and old age (the retirement period). We assume no uncertainty in lifespan, and each period duration is normalised to one.
At every date t, a mass \(N_t\) of newly born individuals (generation) overlaps with the previous one. \(N_t\) grows at an exogenous rate of \(n\in (-1;+\infty )\), so that \(N_t=(1+n)N_{t-1}\).
When young, the representative agent born at t inelastically supplies one unit of labour and earns the competitive wage rate \(w_t\). When retiring, agents consume their accumulated savings as well as the pension benefits (which we formally define below) provided by the government.
The public system consists of two separate pillars: a pension system and a health care system. These two pillars are detailed below.
2.1 Public health investment
We assume that individuals have perfect health (normalised to 1) in the first period of their life, while in the second (old age) period, their health has deteriorated. Their health status in old age, or equivalently their level of autonomy, is denoted by \(d_t\) and depends on public health investment (denoted by \(h_t\)), so that
with \(d_0 \in [0,1)\). In particular \(d_t\) is an increasing and concave function of \(h_t\) with \(d(0)={d_0}\), \(\lim \limits _{h\rightarrow \infty }d(h)=1\) and \(\lim \limits _{h\rightarrow 0} d^{'}(h)={1-d_0}\). We remain agnostic about the significance of \(d_0\), which corresponds to the minimum health status in the absence of public health expenditures. It could be a fixed health status component inherited from a younger age or any other component influencing the health status when old.
Note that since the economy is populated by a continuum of identical individuals, \(d_t\) also represents the average health status at time t in this economy.
Quite importantly, observe that the time index of \(h_t\) in Eq. 1 is the same as the time index of \(d_t\) so that health expenditures are made in the same period as the benefits on health are experienced.Footnote 8 This happens because the objective of our article is to consider curative rather than preventive health expenditures, as is the case for public health investment in quality of life during old age. As already discussed in the introduction, such investments range from building nursing homes to providing day-to-day care, medications and therapies, or quite simply extending existing medical services,Footnote 9
In order to finance public investments in the health of the elderly generation \(h_t\), we assume that the government levies a health tax \(\tau _h\in [0,1]\) on the labour income of the current working generation. For the sake of simplicity, we set the proportional tax on gross wages to be constant over time and, assuming that at each period the health care budget needs to be balanced, we have
Finally, since the objective of this paper is to understand the effect of public health investments in the health of the elderly on capital accumulation and welfare, we voluntarily abstract from modelling private investments in health,Footnote 10
2.2 Health-dependent pensions
We assume a PAYG pension system where young adults pay at period t for the pension benefits received by retirees in the same period. To finance the pension system, the workers pay a proportional contribution rate \(\tau _{p,t}\in [0,1]\), so that
where \(\tau _0,\, \tau _1\in (0,1)\) are contribution rates. The contribution rate paid by workers is constituted of two parts. The first part \(\tau _0\) does not depend on the current health status in society; the second one, \(\tau _1(1-d_t)\) does. This second (health-related) contribution part constitutes the main difference with respect to existing models of pensions and LTC, which always consider pensions and LTC systems as two separate systems and never condition the taxes to be paid on the current average level of old-age disability in society. The idea here is to make workers pay more whenever the health status of the old in the society deteriorates (i.e. \(d_t\) is smaller).Footnote 11 For that reason, the contribution rate to the pension system depends on time t, through \(d_t\) (or equivalently, \(h_t\)).
Assuming that the pension system is balanced at each time period t, each retiree will receive a pension benefit \(p_t\) of the following form:
where the left-hand side accounts for all pension benefits given to retirees and the right-hand side accounts for total contributions to the pension system.
The first part of the above equation, that is, \((1+n)\tau _0w_t\), denotes the traditional contribution part of the PAYG pension benefit. The second part, i.e. \((1+n) \tau _1(1-d_t)w_t\), constitutes the novelty of our approach with respect to standard retirement models: it is the ‘disability-augmented’ part of the pension benefit. If health were perfect (i.e. individuals remained fully autonomous in old age), \(d_t=1\) the second part would vanish. In that case, retirees would obtain a lump sum benefit, \(p_t=\tau _0(1+n)w_t\), independent from the health status in society. Inversely, whenever health is imperfect, that is, \(d_t<1\), workers face an additional tax contribution which is redistributed to retirees. The better (resp. the worse) the health condition in old age in society (through higher -resp. lower- public investment in health), the lower (resp. the higher) would be the tax rate and thus the pension benefits to be served. This additional benefit, indexed to the average level of disability in society, can then be used to finance the additional LTC expenditures caused by a lower level of autonomy during old age.Footnote 12
Note finally that we assume here that the financing of the pension system and of the health system are separated so that no cross-subsidisation is possible between the two systems. We do so for several reasons. First, it is quite realistic to assume two separate public systems financed through different contributions. Second, allowing for cross-subsidisation would complicate the model substantially, and we may not be able to have an explicit relationship between the health status and the pension benefit (as in Eq. 4). Finally, allowing for cross-subsidisation is not necessary to establish the impacts of linking pension benefits to health status on capital accumulation and on welfare.
2.3 Individuals
The lifetime welfare of the representative individual of generation t is modelled through a homothetic and separable utility function \(U_t\), defined over consumption of a private good in young and old ages, and over the health status in old age:
with \(c_{1,t}\) and \(c_{2,t+1}\), denoting private consumption respectively when young and when old (i.e. retired), and \(d_{t+1}\) is the health status in old age which, as we detailed in Section 2.1, depends on public health investment. The parameter \(0<\beta \le 1\) accounts for time preferences, while \(\gamma >0\) is an individual parameter for health preference. A higher \(\gamma \) corresponds to a higher weight attributed to health in old age, and, as we show below, it will motivate higher public investment in health and higher health-related tax rates. As a preference for the desired health status during old age, this parameter can also be thought of as a health-oriented expression of ‘future orientation’.Footnote 13 When \(\gamma =1\), this formulation of the individual’s utility is similar to Marchiori and Pierrard (2022).
Assuming separability is standard in the OLG and the health economics literature. Indeed, we implicitly assume here that there is no complementarity or substitutability between health (or disability) and consumption in old age, or equivalently that the marginal utility of old-age consumption does not depend on the health status (i.e. cross derivatives between consumptions and health are null). As argued by Hall and Jones (2007) and De Donder and Leroux (2021), whether substitutability and complementarity should be assumed is an empirical (and debatable) question. It crucially depends on the type of consumption goods considered, whether it includes traveling, food, restaurants or, conversely, medical expenditures and the adaptation of the house to limitations in daily-life activities. In the former case, consumption and good health are likely to be complements; in the latter case, they are likely to be substitutes. To keep our analysis tractable, we decided to abstract from these considerations.
At time t, young individuals join the workforce and offer one unit of labour to firms, and receive the competitive wage \(w_t\). This salary is taxed to finance both public health investment and the pension system. Therefore, the budget constraint of the young agent at time t is given by
where \(s_t\) are the individual’s savings. Savings are deposited in a mutual fund accruing at a gross return of \(r_{t+1}\). Note that in the following, we ensure that the overall tax rate is below unity: \((\tau _{p,t}+\tau _h)\in (0,1]\).
During old age, consumption \(c_2\) is financed by savings and pension benefits. The budget constraint of an old agent born at time t then writes as
with \(p_{t+1}\) the pension benefit as defined by Eq. 4. Substituting Eqs. 4, 6 and 7 into Eq. 5 and maximising the individual’s utility function \(U_t\) w.r.t. savings, it can be shown that the optimal saving decision \(s_t\) of an individual born in period t is equal to
The second term in the numerator corresponds to the pension benefit, \(p_{t+1}\) the individual expects to receive at the old age. The higher the pension benefit, the smaller the amount of savings, \(s_t\). Hence, if the government increases public health spending \(h_{t+1}\), this will improve the health status at the old age (\(d_{t+1}\)), but at the same time it will decrease the amount of pension received. In turn, the individual will choose to save more.
2.4 Firms
At every period t, firms produce a final good whose price is normalised to unity, for an amount \(Y_t=Y(K_t,L_t)\), which can be consumed, saved or invested in public health. Since in our model, every young agent works, \(L_t=N_t\) and assuming a standard Cobb Douglas production function, we have
with \(\alpha \in (0,1)\) and where \(A>0\) accounts for the exogenous technology productivity or, equivalently, total factor productivity.
We define the production function in per capita terms:
with \(k_t\) is capital per unit of labor.
Perfect competition in the goods market implies that both capital and labour are paid at their respective marginal productivity, so the wage is \(w_t=\frac{\partial Y(K_t, N_t)}{\partial N_t}\) and the rental rate of capital is \(R_t=\frac{\partial Y(K_t, N_t)}{\partial K_t}\). Assuming (in the latter) full depreciation of capital, we get
Again, in the situation of complete depreciation of the capital at each period, we obtain the following relationship between capital and savings:
2.5 Equilibrium
Given the initial level of capital stock \(k_0\), the competitive equilibria are characterised by a sequence of {\(k_t\)} that jointly satisfy the savings condition defined in Eq. 8, the full depreciation capital Eq. 11, the prices Eq. 10 and, the health status and health expenditures Eqs. 1 and 2 respectively. A steady-state equilibrium is an equilibrium in which \(k_t\) (and thus, all other variables) is constant over time. The following proposition provides an existence and a uniqueness result for the steady-state equilibria in the case where \(\alpha \in (0,\frac{1}{2}]\),Footnote 14
Proposition 1
Suppose that \(\tau _h + \tau _0 + \tau _1 (1-d_0)<1\) and \(\alpha \in (0,\frac{1}{2}]\). Then, for a given initial level of capital \(k_0>0\), the dynamics \(\{k_t\}\) of the per capita stocks of capital over time is well defined. The system admits two steady states: the trivial steady state where \(k^*=0\) which is unstable and a positive asymptotically stable steady state \(k^*>0\).
Proof
See Appendix A.1.
For further use, we denote the steady-state values of consumption in both periods, public health expenditures as well as the health status associated to \(k^*>0\), by \(c_{1}^*\), \(c_{2}^*\), \(h^*\) and \(d^*\).
3 Public health investment and capital accumulation
Having established the equilibrium, we now focus on the long-term welfare effects of public health investment when the pension system is made conditional on the old-age level of disability in society (that is, \(p_t\) depends on \(d_t\)). We first analyse the effect of the health tax \(\tau _h\) on capital accumulation. This is crucial since the level of capital determines long-term outcomes such as wages, interest rates, and ultimately welfare (see Section 4).
Whether \(k^*\) increases or decreases in \(\tau _h\) depends on two forces going in opposite directions. On the one hand, a higher health tax reduces disposable income, in turn discouraging savings and eroding capital stock. On the other hand, a higher health tax increases health in old age (through higher public health investments) so that the contribution rate to finance pensions decreases, which increases disposable income, increases the willingness to save and fosters capital accumulation. Nevertheless, depending on parameter values, the latter effect may dominate and we may obtain that as \(\tau _h\) increases, the steady-state level of capital, \(k^*\), increases. Proposition 2 below gives an explicit condition that ensures that this is the case.
Proposition 2
Suppose that the assumptions in Proposition 1 are verified. Consider an economy where \(\tau _h\) is initially equal to 0. The steady-state stock of capital, \(k^{*}\) increases with a small positive \(\tau _h\) as long as the following condition is satisfied:
where \(k_h\) is the steady-state level of capital when \(\tau _h=0\) and is equal to
Proof
See Appendix A.1.
Note that the expression on the left-hand side of condition Eq. 12 is increasing in the level of capital per capita \(k_h\) so that this condition is more likely to be verified in developed economies with an ageing population. That being said, \(k_h\) is not exogenous in our model but depends on specific values of the parameters as shown in the formula Eq. 13. In the next proposition, we derive some comparative statics and see how \(\Gamma \) varies with A, \(\tau _0\), \(\tau _1\) and \(d_0\).
Proposition 3
Suppose that the assumptions of Proposition 1 are verified. The function \(\Gamma \) in Eq. 12 increases in A, decreases in \(\tau _0\), but is ambiguous in \(\tau _1\) and \(d_0\).
Proof
See Appendix A.1.
The above proposition shows that for higher levels of the technological parameter A, condition Eq. 12 is more likely to be verified. Hence, the introduction of a health tax is more likely to foster capital accumulation when A is high. This is then more likely to be the case in developed economies. Conversely, the effect of \(\tau _0\) on \(\Gamma \) is driven by the negative effect of \(\tau _0\) on capital accumulation. Reducing the individual’s disposable income reduces their saving capacity, which in turn decreases capital accumulation, and decreases the likelihood that the threshold condition is satisfied. Hence, a higher level of \(\tau _0\) is more likely to make condition Eq. 13 not be satisfied and lead to a lower level of \(k^*\) when \(\tau _h\) increases. When \(\tau _1\) increases, the same effect on \(\Gamma \) is at play: a higher \(\tau _1\) decreases disposable income and leads to lower savings and a lower level of \(k^*\). Yet, there is now an additional competing effect. Increasing \(\tau _1\) amplifies the marginal impact of \(\tau _h\) (through \(d_t\)) on the contribution rate. Indeed, the degree to which increasing \(\tau _h\) also increases \(d_t\) and hence, reduces the contribution rate will be higher for higher levels of \(\tau _1\), leading to a higher willingness to save. This, in turn, increases disposable income, savings and capital accumulation. This is why the overall impact of \(\tau _1\) on \(\Gamma \) is ambiguous. The effect of \(d_0\) on \(\Gamma \) is symmetric to the effect of \(\tau _1\) on \(\Gamma \) since the health-related contribution part of the pension benefit is modelled by \(\tau _1(1-d_t)\) where \(d_t\) increases linearly in \(d_0\). Two opposite mechanisms are at work. On the one hand, when \(d_0\) increases (for a given level of \(\tau _h\)), \(d^*\) increases, decreasing contributions and thus increasing savings and the level of \(k^*\) so condition Eq. 12 becomes easier to satisfy. On the other hand, when \(d_0\) increases, the marginal effect of public health investment (equivalently, of increasing \(\tau _h\)) on the health status \(d^*\) becomes smaller,Footnote 15 Higher levels of \(d_0\) leads to smaller marginal effects of increasing \(\tau _h\) on \(d_t\) and thus, to a lower decrease of contributions. Hence, the extent to which \(d_0\) increases savings is higher for smaller levels of \(\tau _h\), which makes condition Eq. 12 more difficult to satisfy for higher levels of \(d_0\). The combination of these two effects explains why the variation of \(\Gamma \) with \(d_0\) is ambiguous.
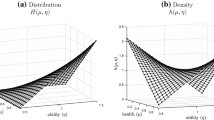
To illustrate how the steady-state level of capital responds to an increase of the health tax, we perform a simple numerical analysis in Fig. 1. To this end, we set the parameter values at the following levels. First, we assume that each representative young adult individual (whose life starts at 20 years old) lives two periods of 40 years each. Assuming an annual discount rate equal to \(1.25\%\), we find that \(\beta =0.6\), which is similar to the value of \(\beta \) in Žamac (2007).
We use a capital-output elasticity of \(\alpha =0.33\) as in de la Croix and Michel (2002). We then set the contribution rate at \(\tau _{0}=8\%\) and \(\tau _{1}=7.5\%\), because a majority of the OECD countries have rates within this range.Footnote 16 Following de la Croix and Michel (2002), we choose the replacement rate in a single-parent model over a period of 40 years, so as to match the annual growth rate of total output, set to \(2\%\). This yields \((1+0.02)^{40}=1+n\), and an exogenous population growth rate of \(n=1.2\). Finally, we set the scale parameter A equal to 50,Footnote 17 The minimum health level \(d_0\) is set to 0.25.Footnote 18 We then perform a numerical exercise considering a range of health tax rate \(\tau _h\) between \(0\%\) to \(7\%\).Footnote 19

Numerical analysis: the effect of \(\tau _h\) on \(k^*\) and on \(h^*\)
The behaviour of \(\tau _h\) in Fig. 1 (and which is robust to the different simulations we have performed) highlights the existence of a threshold \(\bar{\tau }_h\). When \(\tau _h\) is set to zero, the corresponding steady-state level of capital is equal to \(k^{*}=8.55\). Increasing the health tax, we find that the steady-state level of capital increases up to 9.2 when \(\tau _h=\bar{\tau }_h\simeq 2.2\%\), we find that increasing public health taxation further would reduce capital accumulation.
When health taxation is low, that is, \(\tau _h<\bar{\tau }_h\), we find that the steady-state level of capital increases following an increase in \(\tau _h\). In that situation, the increase in the health tax decreases the pension contribution rate (this corresponds to the second part in Eq. 3) which in turn increases disposable income and the willingness to save for old age. This effect is found to dominate the direct negative impact of a higher \(\tau _h\) on the disposable income of the young. The overall effect is an increase in savings and therefore in capital accumulation \(k^*\). This, in turn, results in higher wages, and in higher health investment and in a better health condition of the elderly. This sparks off an indirect general equilibrium feedback effect which further encourages saving, and fosters capital accumulation. As a result, the steady-state output per worker also increases.Footnote 20
However, this multiplier effect is only triggered for small values of \(\tau _h\). For higher tax levels, the direct negative effect on savings of higher taxation outmatches the positive effect of reduced health-dependent pensions as a result of the improvement of elderly health.
All in all, this section shows that the observed positive relationship between increased public health expenditures and capital accumulation (when \(\tau _h\) is not too high) is driven by the young individuals anticipating a better health status in old age and thus, lower public pension contributions and benefits. Obviously, this would not occur under a standard (non-augmented) PAYG pension system. When \(\tau _1\rightarrow 0\), there is no effect of increasing health expenditures on pension benefits, and increasing public health taxation always reduces capital accumulation (through lower savings).
Finally, we find that the effect of \(\tau _1\) on the steady-state level of capital is monotonic: increasing \(\tau _1\) always decreases capital accumulation \(k^*\) at the steady state.Footnote 21 Indeed, it is sufficient to note that savings and pension benefits are substitutes in the transfer of resources from young age to the old-age period. Increasing \(\tau _1\) (or equivalently \(\tau _0\)) would unambiguously increase \(p_t\) which, in turn, would decrease the willingness to save for old age. In addition, higher first-period taxation would decrease disposable income and, as such the saving capacity. These two effects go in the same direction with respect to decreasing savings and thus, to decreasing capital accumulation in equilibrium.
4 Welfare
In this section, we first derive the optimal tax rates \(\tau _1\) and \(\tau _h\), taking \(\tau _0\) as given. We start by modelling an exogenous universal PAYG pension system, by fixing \(\tau _0>0\) and assuming that this tax rate can take different exogenous values (see below). Indeed, in reality, and for different political, historical and economic reasons (e.g. insurance motive, myopia), which we do not model here, public pension systems do exist. We then explore the implications of adding a health-dependent pension component to this existing pension system. Therefore, we consider a second-best problem and show first to what extent the pension scheme should be increased. Second, we quantify the increase in welfare associated with augmenting the standard pension system by the health-dependent component.
4.1 Optimal taxation
In this section, we derive the second-best tax rate levels, \(\tau _1^*\) and \(\tau _h^*\), postulating the existence of a pension system that provides benefits in old age to the individual (as is the case in most developed countries). To do so, we exogenously fix \(\tau _0\ge 0\) and find the values of \(\tau _1\) and \(\tau _h\) that maximise the utility of the representative agent at the steady state when varying the parameter of health preference \(\gamma \). More precisely, we study the impact of varying \(\gamma \) on the (non-trivial) steady-state equilibrium characterised in Proposition 1.
In our general equilibrium framework, choosing the optimal values for \(\tau _1\) and \(\tau _h\) consists in maximising the utility of the representative agent, Eq. 5, taking into account that \(c_1^*\), \(c_2^*\) and \(d^*\) (or \(h^*\)) depend both directly on these tax rates as well as indirectly on them (through \(k^*\) in the pension benefits, wages and interest rates). Table 1 reports the optimal values of the tax rates as a function of the preference parameter \(\gamma \).Footnote 22 In this table, we consider different possible values of \(\tau _0\) ranging from \(0\%\) to \(15\%\). The assumed values for the \(\tau _0\) rates correspond to a range of what is usually observed in OECD countries (see footnote 16).Footnote 23
First note that the level of the contribution to the health system, \(\tau ^*_h\), is always strictly positive, whatever the levels of \(\tau _0\) and \(\tau ^*_1\). This is directly related to the fact that individuals value health in their utility function so that \(h^*>0\) is always optimal. On the contrary, \(\tau ^*_1\) becomes positive only above some \(\gamma \)-threshold whose level increases with the value of \(\tau _0\). This is due to the fact that both \(\tau _0\) and \(\tau _1\) put pressure on financial resources available to the individual in the first period so that when \(\tau _0\) increases, the minimum \(\gamma \) level for which \(\tau ^*_1\) becomes positive must also increase.
Let us now concentrate on the role of \(\gamma >0\) on the optimal pension design. An increase in the health-preference parameter always increases the optimal levels of the tax rates \(\tau _1\) and \(\tau _h\), for any given level of \(\tau _0\).Footnote 24 Indeed, when people exhibit a higher preference for health, it is optimal for a government that seeks to maximise welfare to increase health-related taxes. Conversely, the optimal level of \(\tau _1\) becomes positive only for a sufficiently high level of \(\gamma \). The mechanism behind this result runs as follows. When \(\gamma \) increases, \(\tau _h\) increases which decreases savings in the first period as well as the overall return individuals can obtain during old age. Appendix A.2 shows that this is effectively the case. When \(\gamma \) is low, pension benefits together with savings are high enough to guarantee sufficient consumption in old age. Yet, when \(\gamma \) increases further, savings decrease further and it becomes more difficult to obtain sufficient old-age consumption since the pension contribution rate \(\tau _0\) is fixed, and may not be enough to compensate for the decrease in savings. It then becomes desirable to activate the health-dependent component of the pension benefit \(\tau _1>0\), so as to ensure that enough resources are effectively transferred for old age without undercutting first-period consumption too much (since better health also implies lower contribution rates through higher \(d^*\)).
All in all, this section shows that while it is always optimal to have a health system (\(\tau _h^*>0\)), introducing a health component in the pension benefit (i.e. an augmented pension benefit with \(\tau _1^*>0\)) becomes desirable only above some high enough level of \(\gamma \), in order to compensate for lower savings.
Relating these findings with what we observe in reality, it is reasonable to assume that in recent years individuals have become more concerned with their health (in all stages of life) as a consequence of first, population ageing (and with it, an increasing probability to become dependent) and second, of our economies becoming richer and more informed about health issues. The above results then demonstrate that it would indeed be optimal to implement a health-dependent pension system in this context.
4.2 Quantification of welfare
We now concentrate on quantifying the welfare effect of implementing an augmented pension system, that is the welfare effect of allowing the pension benefits to be conditioned on the average disability level in society. To do so, we set \(\tau _0=8\%\) as in the average of OECD countries and compare the welfare of the representative individual in steady state when \(\tau _1=0\) (that is, when the pension system is a ‘traditional’ one ) with his welfare when \(\tau _1^*>0\) is set at its optimal steady-state level (i.e. the pension benefit is ‘disability-augmented’). In both cases, \(\tau _h\) is chosen optimally (i.e. as a solution of the individual’s problem). We then quantify by how much society’s welfare is increased when augmenting the standard PAYG pension system by its disability-related component. As we showed in the previous section, whether the optimal level of \(\tau _1^*\) is strictly positive depends on the size of the health-preference parameter.
Our results are reported in Table 2, which is divided in three parts. In the first four columns, we report the values of \(c_1^{*}\), \(c_2^{*}\), \(h^*\) (and \(\tau ^*_h\)) when \(\tau _0\) is fixed to \(8\%\), \(\tau _1\) is exogenously fixed to \(0\%\) but \(\tau _h^*\) maximises the steady-state utility of the representative agent. In the second part of the table (columns six, seven, eight and nine), we report the values of \(c_1^{*}\), \(c_2^{*}\), \(h^*\) (and \(\tau ^*_h\)) when \(\tau _0\) is still fixed to \(8\%\) but both \(\tau ^*_1\) and \(\tau ^*_h\) are (jointly) chosen to maximise the utility of the representative agent at the steady state.Footnote 25 The last column reports the relative variation in the utility between a standard PAYG system (\(\tau _1=0\%\)) and the augmented PAYG system (\(\tau _1^{*}>0\)).
Table 2 clearly shows that, given the existence of a universal PAYG pension system, augmenting the system with a health-dependent pension increases welfare when \(\tau _1\) and \(\tau _h\) are set at their optimal levels and, provided that \(\gamma \) is sufficiently high.Footnote 26 The effects of augmenting the pension system may look small when considering variations in utility, but this is due to the concavity of the log-utility function: for large values of c, the utility function is not very sensible to variations of c. Still, we can observe a relevant change in the consumption behaviour of the agents.
5 Concluding remarks
This paper shows that introducing a Social Security system that combines both a public health system and a health-dependent pension system to account for average old-age disability in the economy can be beneficial to society.
We do so by studying an OLG problem that includes both a health system and a PAYG pension scheme in which pension benefits are augmented by a health-related component, indexed to the average level of disability during old age. We show how such a modification of the pension system affects capital accumulation and welfare.
Our analysis produces several insightful predictions regarding the effects of Social Security taxation on individual decisions, capital accumulation, and welfare. First, an increase in public health investment through an increase in the health tax can boost the steady-state stock of capital. This result emerges because health taxation (financing curative health care) improves health during old age, mitigating average disability in society, which in turn allows to reduce taxation for financing pensions. This increases the willingness to save for old age, as a result of consumption smoothing. Second, given the existing PAYG pension system, we show that introducing a disability-linked component to the pension benefit allows for welfare improvements. This will even be the case more often if the preference for health in society is high enough.
In a context where LTC expenditures are projected to rise dramatically in the near future, and where society’s preference for health improvements has been increasing over the last decades, our model highlights the possible positive spillovers of linking the effects of public health investment (i.e. reducing old-age dependency) to public pension benefits. Indeed, under some conditions, investment in curative health programs together with health-dependent pension benefits is shown to increase social welfare.
Lastly, let us note that in order to obtain clear results we voluntarily abstracted from modelling preventive health expenditures, which may also reduce the extent of dependency in old age. Doing so would require to make several further hypotheses, in particular, whether such spending is decided publicly or results from private decisions. In addition, we would need to make assumptions regarding the relationship between preventive and curative health spending, and whether these are substitutes or complements. Depending on the preferred assumptions, we may then obtain different conclusions. We believe that this would be an interesting extension, left for future work.
Availability of data and materials
the code for generating figures and conducting numerical simulations in the paper is accessible at the following link: https://sites.google.com/site/giorgiofabbri1979/code.
Notes
We follow Cremer (2014) in defining long-term care as ‘the provision of assistance and services to people who, because of disabling illnesses or conditions, have limited ability to perform daily activities such as bathing and preparing meals’. LTC is mainly targeted toward the elderly, with needs arising from various chronic diseases (mostly diabetes and -increasingly- cancer), Alzheimer or other forms of dementia.
Multiple explanations have been suggested for this ‘LTC insurance puzzle’, both on the supply side (e.g. adverse selection leading to high loading costs) as well as on the demand side (e.g. myopia, bequest motives). See, among others, Pauly (1990); Pestieau and Ponthière (2012); Brown and Finkelstein (2009, 2007); Lockwood (2018) and Boyer et al. (2020).
In Québec in 2015, the implementation of an additional benefit to retirees above a given age was discussed in order to cope with the potential additional costs due to a loss of autonomy at older age (Hébert 2016). Because of a change in government majority, this so-called ‘assurance autonomie’ was never implemented.
This is inherent to the design of PAYG pension systems, where working individuals pay for the pensions of retired individuals. If healthier people live longer, there will logically be fewer working contributors for each pensioner, a downward trend projected to accelerate (Pecchenino and Pollard 2005). See also Cigno and Werding (2007) on increasing age-dependency ratios.
Grossmann and Strulik (2019) come closest, by studying the effect of medical progress on health spending, pension savings for old age and the retirement age. They show that medical progress is in conflict with reducing health inequalities. Contrary to us, they have no private savings and the pension system does not include an ‘augmented’ disability component.
In reality, the individual health condition, even in old age, depends on many factors such as for example, personal behaviour and lifestyle, as well as health investments (see among others, Balia and Jones 2008; Contoyannis and Jones, 2004; Ettner, 1996; Kaplan et al., 1987). Modelling private investments in health would require to make further assumptions regarding complementarity or substitutability between public and private health spending. In any case, we would find some crowding-out effect of private health spending by public ones, the extent to which would depend on the relative return of private versus public spending, on the form of the health production function and on the levels of the pension contributions and benefits. This would complicate our model without further qualitative results. In the extreme end, and for some parameter values, it may even be the case that private spending is fully crowded out by public spending, which brings us back to the special case in our model with only public spending.
This is comparable to the ‘Journée de la solidarité’ (i.e. ‘solidarity day’) which was implemented in France in 2004. This policy measure consisted in suppressing one vacation day to finance LTC at the old age and disability programs. This can equivalently be seen as imposing an additional contribution based on the average old-age disability level in the society.
We implicitly assume here that becoming dependent in old age entails higher overall financial needs than remaining autonomous. On this, see De Donder and Leroux (2021).
In psychology and related fields, ‘future orientation’ is broadly defined as the extent to which an individual thinks about the future, anticipates future consequences, and plans ahead before acting. In a survey covering French respondents, Apouey (2018) explores this broader notion of time preferences over the future, and finds correlational evidence linking it to preparation for old age (showing, for example, in saving behaviour, home adaptation and ownership, but not in LTC insurance). Similarly to Reckers-Droog et al. (2021), this preference parameter can therefore be seen as representing the marginal willingness to pay for health, but specifically oriented towards old age.
Values for \(\alpha \) typically range between 0.3 and 0.4 (see for example Gollin 2002). In the case where \(\alpha \) is greater than 1/2, we may have multiplicities of stable equilibria.
To see this, note that in Eq. 1 the larger \(d_0\), the smaller the marginal impact of \(h_t\) on \(d_t(h_t)\).
See for instance the graphs available at https://data.oecd.org/tax/social-security-contributions.htm. Over the period 2000–2020, Social Security contribution rates in the OECD countries varied around an average of 8%.
Our results are robust to alternative levels of \(d_0\). Yet, for higher levels of \(d_0\), our results, although qualitatively similar, are quantitatively less strong. This is a consequence of the marginal effect of \(h_t\) on \(d_t\) being smaller for higher levels of \(d_0\) (see footnote 15).
The code for generating figures and conducting numerical simulations in the paper is accessible at the following link: https://sites.google.com/site/giorgiofabbri1979/code.
To prove this, we use the implicit function theorem on \(k^*\) similar to the comparative statics derivation with respect to \(\tau _h\) (see eq. (18) in the proof of Proposition 2, Appendix A.1).
In a situation where agents do not value their health (i.e. \(\gamma =0\)), we find that it is optimal to set \(\tau ^*_h=\tau ^*_1=0\) for two reasons. On the one hand, individuals do not obtain direct utility from investing in health and, on the other hand, the agents’ savings (and eventually the fixed part of the pension system) are already sufficient to ensure that enough resources are transferred to the next period.
We use the same parametrization as in the previous section: \(\alpha =0.33\), \(\beta =0.6\), \(A=50\), \(d_0=0.25\) and \(n=1.2\). In the simulations, we also find that the level of health \(d^*\) is always comprised between 0.81 and 0.95.
Note that the optimal tax rates increase nonetheless at a lower rate when \(\gamma \) becomes higher, which is due to the concavity of the utility function in consumption.
We do not report the values of \(\tau _1^{*}\) here, but these correspond to the values reported in the part of Table 1 where \(\tau _0=8\%\).
These results are robust to other values of \(\tau _0\).
References
Apouey BH (2018) Preparation for old age in France: the roles of preferences and expectations. J Econ Ageing 12:15–23
Balia S, Jones AM (2008) Mortality, lifestyle and socio-economic status. J Health Econ 27(1):1–26
Bhattacharya J, Qiao X (2007) Public and private expenditures on health in a growth model. J Econ Dyn Control 31(8):2519–2535
Blackburn K, Cipriani GP (2002) A model of longevity, fertility and growth. J Econ Dyn Control 26(2):187–204
Boyer MM, De Donder P, Fluet C, Leroux M-L, Michaud P-C (2020) Long-term care insurance: information frictions and selection. Am Econ J Econ Policy 12(3):134–69
Brown JR, Finkelstein A (2007) Why is the market for long-term care insurance so small? J Public Econ 91(10):1967–1991
Brown JR, Finkelstein A (2009) The private market for long-term care insurance in the united states: a review of the evidence. J Risk Insur 76(1):5–29
Canta C, Pestieau P (2013) Long-term care insurance and family norms. BE J Econ Anal Policy 14(2):401–428
Canta C, Pestieau P, Thibault E (2016) Long-term care and capital accumulation: the impact of the state, the market and the family. Econ Theory 61(4):755–785
Chakraborty S (2004) Endogenous lifetime and economic growth. J Econ Theory 116(1):119–137
Cigno A, Werding M (2007) Children and pensions. MIT Press
Contoyannis P, Jones AM (2004) Socio-economic status, health and lifestyle. J Health Econ 23(5):965–995
Cremer H (2014) The economics of long-term care: an introduction. BE J Econ Anal Policy 14(2):339–342
Davila J, Leroux M-L (2015) Efficiency in overlapping generations economies with longevity choices and fair annuities. J Macroecon 45:363–383
De Donder P, Leroux M-L (2014) Behavioral biases and long term care insurance: a political economy approach. BE J Econ Anal Policy Adv 14(2):551–575
De Donder P, Leroux M-L (2017) The political choice of social long term care transfers when family gives time and money. Soc Choice Welf 49:755–786
De Donder P, Leroux M-L (2021) Long term care insurance with state-dependent preferences. Health Econ 30(12):3074–3086
De Donder P, Pestieau P (2017) Private, social and self insurance for long-term care in the presence of family help. J Public Econ Theory 19(1):18–37
de la Croix D, Licandro O (2013) The child is father of the man: implications for the demographic transition. Econ J 123(567):236–261
de la Croix D, Michel P (2002) A theory of economic growth: dynamics and policy in overlapping generations. Cambridge University Press
de la Croix D, Ponthiere G (2010) On the golden rule of capital accumulation under endogenous longevity. Math Soc Sci 59(2):227–238
Diamond PA (1965) National debt in a neoclassical growth model. The American economic review, pp 1126–1150
Ettner S (1996) New evidence on the relationship between income and health. J Health Econ 15(1):67–85
Eurostat (2023) Functional and activity limitations statistics. https://shorturl.at/pHS45
Fanti L, Gori L (2007) From the Malthusian to the modern growth regime in an OLG model with unions. Econ Bull 10(14):1–10
Fanti L, Gori L (2011) Public health spending and unfunded public pensions in an OLG model of neoclassical growth: some new results about the poverty trap problem. Rivista Italiana Degli Economisti 16(2):319–338
Fanti L, Gori L (2011) Public health spending, old-age productivity and economic growth: chaotic cycles under perfect foresight. J Econ Behav Organ 78(1):137–151
Fanti L, Gori L (2014) Endogenous fertility, endogenous lifetime and economic growth: the role of child policies. J Popul Econ 27(2):529–564
Gollin D (2002) Getting income shares right. J Polit Econ 110(2):458–474
Grossmann V, Strulik H (2019) Optimal social insurance and health inequality. Ger Econ Rev Verein für Socialpolitik 20(4):913–948
Hall RE, Jones CI (2007) The value of life and the rise in health spending. Q J Econ 122(1):39–72
Hébert R (2016) Still-born autonomy insurance plan in Quebec: an example of a public long-term care insurance system in Canada. Healthcare Papers 15(4):45–50
Jouvet P, Pestieau P, Ponthiere G (2010) Longevity and environmental quality in an OLG model. J Econ 100(3):191–216
Kaplan GA, Seeman TE, Cohen RD, Knudsen LP, Guralnik J (1987) Mortality among the elderly in the alameda county study: behavioral and demographic risk factors. Am J Public Health 77(3):307–312
Kopecky K, Koreshkova T (2014) The impact of medical and nursing home expenses on savings. Am Econ J Macroecon 6(3):29–72
Lockwood L (2018) Incidental bequests: bequest motives and the choice to self-insure late-life risks. Am Econ Rev 108(9):2513–2550
Marchiori L, Pierrard O (2022) Health subsidies, prevention and welfare. Journal of Public Economic Theory
OECD (2021) Health at a Glance 2021. OECD Publishing, Paris
Pauly M (1990) The rational non-purchase of long-term care insurance. J Polit Econ 95:153–168
Pecchenino RA, Pollard PS (2005) Aging, myopia, and the pay-as-you-go public pension systems of the g7: a bright future? J Public Econ Theory 7(3):449–470
Pestieau P, Ponthière G (2012) Long-term care insurance puzzle. In Financing long-term care in Europe, pp 41–52. Springer
Pestieau P, Sato M (2008) Long-term care: the state, the market and the family. Economica 75(299):435–454
Reckers-Droog V, van Exel J, Brouwer W (2021) Willingness to pay for health-related quality of life gains in relation to disease severity and the age of patients. Value in Health
Siciliani L (2013) The economics of long-term care. BE J Econ Anal Policy 14(2):343–375
Žamac J (2007) Pension design when fertility fluctuates: the role of education and capital mobility. J Public Econ 91(3–4):619–639
Zhao K (2014) Social security and the rise in health spending. J Monet Econ 64:21–37
Acknowledgements
The authors would like to thank three anonymous referees, and the Editor, Gregory Ponthiere, for their valuable comments that helped us improve the paper. We also thank Rym Aloui, David Bell, Rosella Levaggi, Alexander Ludwig and Pierre Pestieau for their suggestions on previous versions of this paper.
Funding
The work of Giorgio Fabbri is partially supported by the French National Research Agency in the framework of the ‘Investissements d’avenir’ program (ANR-15-IDEX-02) and of the center of excellence LABEX MME-DII (ANR-11-LBX-0023-01). Marie-Louise Leroux acknowledges funding from the Fonds de Recherche du Québec-Société et Culture (FRQSC, grant number: 2024-SE3-328700), and from Social Sciences and Humanities Research Council of Canada (Grant number: 435-2020-0787). Paolo Melindi-Ghidi acknowledges financial support from the French government under the ‘France 2030’ investment plan managed by the French National Research Agency Grant ANR-17-EURE-0020, and by the Excellence Initiative of Aix-Marseille University - A*MIDEX.
Author information
Authors and Affiliations
Contributions
The authors have all contributed equally to the submitted paper.
Corresponding author
Ethics declarations
Ethics approval
Not applicable
Conflict of interest
The authors declare no competing interests.
Additional information
Responsible editor: Gregory Ponthiere.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Fabbri, G., Leroux, ML., Melindi-Ghidi, P. et al. Conditioning public pensions on health: effects on capital accumulation and welfare. J Popul Econ 37, 47 (2024). https://doi.org/10.1007/s00148-024-01020-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00148-024-01020-z