
Abstract
Purpose
Nasal continuous positive airway pressure (nCPAP) is currently the gold standard for respiratory support for moderate to severe acute viral bronchiolitis (AVB). Although oxygen delivery via high flow nasal cannula (HFNC) is increasingly used, evidence of its efficacy and safety is lacking in infants.
Methods
A randomized controlled trial was performed in five pediatric intensive care units (PICUs) to compare 7 cmH2O nCPAP with 2 L/kg/min oxygen therapy administered with HFNC in infants up to 6 months old with moderate to severe AVB. The primary endpoint was the percentage of failure within 24 h of randomization using prespecified criteria. To satisfy noninferiority, the failure rate of HFNC had to lie within 15% of the failure rate of nCPAP. Secondary outcomes included success rate after crossover, intubation rate, length of stay, and serious adverse events.
Results
From November 2014 to March 2015, 142 infants were included and equally distributed into groups. The risk difference of −19% (95% CI −35 to −3%) did not allow the conclusion of HFNC noninferiority (p = 0.707). Superiority analysis suggested a relative risk of success 1.63 (95% CI 1.02–2.63) higher with nCPAP. The success rate with the alternative respiratory support, intubation rate, durations of noninvasive and invasive ventilation, skin lesions, and length of PICU stay were comparable between groups. No patient had air leak syndrome or died.
Conclusion
In young infants with moderate to severe AVB, initial management with HFNC did not have a failure rate similar to that of nCPAP. This clinical trial was recorded in the National Library of Medicine registry (NCT 02457013).
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute viral bronchiolitis (AVB) is the most common respiratory infection in infancy and the leading cause of hospitalization among infants in high-income countries [1]. While most cases require supportive management only, a severe form of illness observed in 8–13% of the cases requires hospitalization in a pediatric intensive care unit (PICU) for evolving respiratory distress [2]. Although AVB may present as a restrictive parenchymal disease, most of these infants have severe obstructive lung disease [3] with markedly increased inspiratory load [4, 5], rapid shallow breathing pattern [5, 6], and gradual increase in end-expiratory volume [6] that adversely affects their work of breathing [5–7]. Use of nasal continuous positive airway pressure (nCPAP) levels of 6–7 cmH2O in this situation has been associated with rapid unloading of respiratory muscles, increased expiratory time, and concomitantly improved respiratory distress [5, 6, 8]. In comparison with historical cohorts supported exclusively by invasive ventilation, more recent studies have reported that first-line nCPAP also reduces duration of ventilation and hospital stay [9, 10]. Thus, the preemptive nCPAP strategy has been increasingly used over the last decade, and it is currently the gold-standard respiratory support for moderate to severe AVB [10].
The provision of CPAP requires specific equipment, trained teams, continuous monitoring, and a level of supervision that is usually found only in PICUs. Oxygen delivery with high flow nasal cannula (HFNC) allows the administration of a heated and humidified mixture of air and oxygen at a flow higher than the patient’s inspiratory flow [11]. It has been widely adopted in PICUs and for interhospital transport of critically ill children, as the system is easily set up and is well tolerated by patients [12]. In the context of AVB, retrospective audits and observational studies have suggested promising outcomes on both physiological [7, 13] and clinical variables [14–18]. Two randomized controlled studies in infants not affected by a severe form of AVB reported efficiency comparable to that of hypertonic saline in treating respiratory distress signs [19] and a significant increase in SpO2 within the first 12 h of management compared with head-box oxygen therapy [20]. However, no study has yet provided a direct demonstration of HFNC efficacy and safety compared with the gold-standard respiratory support, nCPAP [21]. Given the effects of HFNC on the work of breathing and lung volumes [13, 22], the ease of installation, and the good tolerance [23], we hypothesized that this support would be an appropriate alternative to nCPAP. We performed a multicenter, randomized, noninferiority trial of HFNC compared with nCPAP for the initial respiratory management in young infants with moderate to severe AVB.
Methods
This prospective randomized multicenter trial was conducted in five PICUs from five French university hospital centers.
Ethical consideration
This study was conducted in accordance with the amended Declaration of Helsinki. The study protocol was approved by the South Mediterranean IV Ethics Committee (ID-RCB: 2014-A01029-38; 2014-09-09), and no amendment was made thereafter. This clinical trial was recorded in the National Library of Medicine registry (NCT 02457013; 2015-01-27).
Written authorization was obtained from the two parents. If one of the parents was absent, deferred signed authorization was accepted after a telephone call and oral agreement.
Population
Patients aged from 1 day to 6 months and hospitalized in the PICU were eligible for inclusion if the following conditions were all met: (1) clinical diagnosis of bronchiolitis; (2) moderate to severe respiratory distress, defined by a modified Wood’s clinical asthma score (mWCAS) >3; (3) no underlying cardiac or neuromuscular disease and no pneumothorax on chest radiograph; (4) absence of indication for imminent intubation; and (5) authorization to perform the study signed by both parents.
Study design
On admission, the nurse started monitoring the infant with pulse oximetry (SpO2), blood pressure, and transcutaneous CO2 (TcCO2). A mixture of air/oxygen was provided at a flow rate of 1 L/min, with FiO2 set in order to reach SpO2 of 94–97%. Corticosteroid, bronchodilator, and chest physiotherapy were stopped if provided beforehand. Chest X-ray and capillary blood gas measurements were performed, and the infant was maintained in a quiet environment. Baseline observation was made 15 min later to collect respiratory rate (RR), heart rate (HR), mWCAS [24], and neonatal pain and discomfort using the EDIN scale [25].
When an infant met the inclusion criteria, respiratory support was randomly allocated as nCPAP or HFNC. Two different systems were used to generate nCPAP: the Infant Flow Ventilator (Electro Medical Equipment, Brighton, UK), and the FlexiTrunk infant interface (Fisher and Paykel, Villebon, France) connected to ventilator CPAP setups. Whatever the system, positive continuous pressure was set at +7 cmH2O [6]. The sole HFNC device used was the Optiflow (Fisher and Paykel, Villebon France). Flow was delivered at 2 L/kg/min, with the device equipped with a pressure release valve set at 45 cmH2O. In both groups, FiO2 was titrated in order to achieve a normoxic SpO2 of 94–97%, as usually recommended in PICUs [10, 15, 26], and the humidifier was auto set at 37 °C.
The protocol lasted a minimum of 24 h after the allocated treatment had begun. In both groups, RR, HR, mWCAS, EDIN score, skin lesion score, FiO2, SpO2, and TcCO2 were systematically assessed 1 h, 12 h, and 24 h after the start of the procedure. Detailed information on the protocol was given to the nursing teams in each PICU to ensure that an investigator would be notified as soon as the continuous monitoring or scores indicated worsening in an infant’s condition. At any moment during this period, occurrence of at least one failure criterion justified a switch to the alternative respiratory support. Patients switched from one group to the other were maintained on the second support for 24 h, and the data were again collected 1 h, 12 h, and 24 h following the crossover. A patient failing with the alternative respiratory support was maintained in the study, but the protocol was stopped and the next therapeutic step was decided by the physician involved in the patient’s care.
Randomization and masking
Patients were centrally randomized to assign them to receive either nCPAP or HFNC. Randomization was performed using block sizes of two and four and was stratified by center. Randomization lists were prepared by the Clinical Research and Epidemiology Unit of Montpellier University Hospital. Allocations were concealed in opaque sealed envelopes.
Failure criteria
Failure was defined by the occurrence of one of the following criteria: (1) a 1-point increase in mWCAS compared with baseline; (2) RR rise >10 bpm compared with baseline, with RR >60 bpm; (3) a 1-point increase in the EDIN score compared with baseline, with EDIN >4 despite the use of hydroxyzine (1 mg/kg); and (4) more than two severe apnea episodes per hour (i.e., requiring bag and mask ventilation), despite a loading dose of caffeine (20 mg/kg) after the first apnea.
Outcome
The primary outcome was treatment failure within 24 h after randomization. This limited duration took into account (1) the policy in some participating PICUs of transferring stabilized patients after a few days and (2) several reports that the risk of failure is highest within 24 h of commencing the two techniques [16, 17, 27, 28]. Prespecified secondary outcomes included delay, causes, and predictors of failure [29], success rate after crossover, intubation rate, occurrence of skin lesions, length of stay, and serious adverse events (air leak syndrome and death).
Scales and scores
mWCAS is a composite score assessing the severity of bronchiolitis through five components: cyanosis, inspiratory breath sounds, accessory muscle use, expiratory wheezing, and cerebral function. Each is rated as follows: 0 for none, 0.5 for mild, 1 for moderate, and 2 for maximal [5]. A visual analog scale is used to standardize the scoring of accessory muscle use and wheezing [30].
EDIN is a neonatal pain and discomfort scale comprising five behavioral indicators: facial activity, body movements, quality of sleep, quality of contact, and consolability [25].
Skin lesions were documented according to the National Pressure Ulcer Advisory Panel (NPUAP) definitions [31].
Statistical analyses
To satisfy the noninferiority criterion, we considered that the failure rate of the HFNC device should lie within 15% of the failure rate of the CPAP device. A power calculation indicated that 142 patients were needed for the study, using an estimated 85% success rate for both devices, power of 80%, and p < 0.05. This success rate was extrapolated from key studies using either of the two techniques [9, 10, 14–18, 27, 28]. The noninferiority of the HFNC device was assessed by the one-sided Farrington–Manning confidence limit for the risk method using the prespecified noninferiority margin of 15%. Both intention-to-treat and per-protocol analyses were performed. Other outcomes were compared using the Fisher, Wilcoxon–Mann–Whitney, and Chi-squared tests as appropriate. All analyses were made using an intention-to-treat approach unless otherwise stated. SAS Enterprise Guide 4.3 (SAS Institute, Cary, NC, USA) was used to generate the randomization list and perform all statistical analyses.
Results
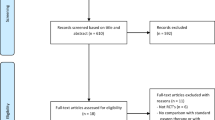
From 1 November 2014 to 1 March 2015, 342 infants were admitted to the PICUs with a diagnosis of AVB. A total of 142 (77.6%) were included from the 183 eligible patients (Fig. 1). Twenty six (18%) had been born prematurely. Their postnatal age was comparable (p = 0.21) but their weight was lower (p < 0.001) than that of the other infants. Respiratory syncytial virus (RSV) was positive for 125 (88%). Following randomization, patients—including those born preterm—were equally distributed into the CPAP and HFNC groups (n = 71 in each, Table 1).

Flowchart of the study population. PICUs pediatric intensive care units, mWCAS modified Wood’s clinical asthma score, nCPAP nasal continuous positive airway pressure, HFNC high flow nasal cannula
Primary endpoint
Failure occurred in 22 of 71 infants (31.0%) in the nCPAP group and 36 of 71 infants (50.7%) in the HFNC group.
Noninferiority analysis
With a risk-difference of −19% (95% CI −35 to −3%), the prespecified noninferiority margin of −15% was included in the confidence limit, not allowing the conclusion of noninferiority (p = 0.707). Hence, the result allowed us to test the superiority of nCPAP compared with HFNC.
Superiority analysis
The intention-to-treat population was used to test the superiority of nCPAP compared with HFNC. With a difference of 20% (95% CI 4–36%), success was higher in the nCPAP group (p = 0.001), suggesting the superiority of nCPAP and a relative risk of success 1.63 (95% CI 1.02–2.63) higher with nCPAP compared with HFNC.
Secondary endpoints
Timing and causes of failure
Sixty percent of failures (35/58) were observed during the first 6 h following treatment allocation (Fig. 2). The mean time to failure was comparable between groups [6.7 (5.7) vs 9.7 (8.8) h, p = 0.19].

Probability of treatment failure with nasal continuous positive airway pressure (nCPAP, blue diamonds) or high flow nasal cannula (HFNC, red squares) according to time (h) in infants with acute viral bronchiolitis. p values were 0.29 at 1 h, 0.12 at 6 h, 0.04 at 12 h, and 0.05 at 24 h using a mixed model
The reasons for treatment failure in the two study groups were rise in m-WCAS (31 cases), rise in RR (27 cases), rise in EDIN score (19 cases), and apnea (7 cases). Discomfort was the leading cause of failure in the nCPAP group. Worsening of respiratory distress signs was more frequent in the HFNC group (Table 2).
Predictors of failure
Among the data collected at baseline (Table 1), univariate analysis found that higher weight (p = 0.04) was the only predictor of failure in the nCPAP group. For infants randomized into the HFNC group, higher baseline FiO2 (p = 0.02) was the sole predictor of failure.
The failure rate of infants born preterm did not differ from that of the other infants (p = 0.38). Despite a broader use of caffeine (p = 0.008), apnea—whatever the randomization group—was a more frequent cause of failure in these patients (15.3 vs 2.5%; p = 0.02).
Failure rate was not different among centers (p = 0.48) or among interfaces used for nCPAP (p = 0.76).
Prespecified patient’s outcomes
All patients who failed were switched to the alternative respiratory support (Fig. 3). The success rate with the alternative support did not differ between groups (p = 0.53).

Patient outcome after crossover. nCPAP nasal continuous positive airway pressure, HFNC high flow nasal cannula, BiPAP bilevel positive airway pressure
The main prespecified data collected after the protocol was revealed no significant difference between groups (Table 3). Eight (5.7%) infants were intubated during PICU hospitalization. Two, both randomized into the HFNC group, were intubated during the protocol period, and six after its completion. Three of them had been randomized into the nCPAP group, including one switched to HFNC. The three others had been randomized into the HFNC group and were all switched to nCPAP. Intubation tended to be associated with HFNC failure (p = 0.054) but not with nCPAP failure (p = 1).
All skin lesions were classified as NPUAP stage 1, including redness of the philtrum and the nasal bridge. None of the patients had air leak syndrome or died.
Discussion
In this multicenter randomized trial, the effectiveness of HFNC was not equivalent to that of nCPAP as the initial respiratory support for young infants with moderate to severe AVB. A majority of the failures with HFNC occurred early, within 6 h of initiation, and worsening of respiratory distress was the leading cause. When treatment with HFNC failed, about two-thirds of the infants were successfully treated with nCPAP, resulting in nonsignificant between-group differences in the rate of intubation, serious adverse events, and length of stay in the PICU.
When planning the study, we assumed a success rate of 85% on the basis of previous reports on preemptive ventilatory strategies with nCPAP or HFNC in infants with AVB [9, 10, 14–18, 27, 28]. Our results showed lower performances, with both nCPAP and HFNC, which may be explained by the selection of a homogeneous population with a serious form of the disease.
Among the failure criteria, we selected two indicators predictive of respiratory muscle fatigue and escalation toward invasive ventilation. The mWCAS was chosen, as this scoring tool has been the most frequently used to assess change over time in respiratory distress in both trials and clinical practice [32, 33]. Previous studies using this score have found significant correlations between mWCAS and indices of inspiratory effort, which estimates the metabolic cost of breathing [5, 34]. An increase in RR was also chosen because several reports have suggested that this objective variable may be an early predictor of the response to nCPAP or HFNC [13, 16, 18, 28, 35]. The results of our study suggested that HFNC was less efficient than nCPAP in rapidly improving the breathing pattern and unloading the respiratory muscles in infants with hypercapnic AVB [6, 8].
A common reason for PICU referral in cases of AVB is apnea requiring mechanical respiratory support [36]. Despite the characteristics of our population, notably the young age of the infants and the significant proportion of preterms [37], apnea was a cause of failure in less than 5% of patients. Throughout the TRAMONTANE study, the use of caffeine was considered as a standard of care in all the investigation centers. Since then, however, a randomized trial did not demonstrate the usefulness of this treatment [38], yet it should be noted that the use of nCPAP and HFNC was very low in this work.
Intolerance of nCPAP was observed in nearly 20% of the infants. By comparison, HFNC was associated with a higher degree of comfort: prongs are softer, and connected to a lightweight circuit fixed under the nose that does not interfere with the visual field and the infant’s communication skills.
Switching a patient from one group to the other was a successful strategy in most cases, either early in patients supported by HFNC requiring high levels of oxygen, or later in patients uncomfortable with nCPAP. Downstream of the initial management, none of the prespecified secondary outcomes differed between groups. As the TRAMONTANE study was not powered to investigate intubation rates, larger multicenter studies will be required to assess the difference between nCPAP and HFNC for this critical outcome.
The strengths of this study include the multicenter design, a study protocol that included prespecified criteria for failure, and an intention-to-treat analysis. TRAMONTANE is one of the largest interventional studies performed in a PICU on this topic, and it is the first trial to directly compare two modalities of noninvasive ventilation for the initial management of AVB.
Limitations
The need for intubation, which is the gold standard in trials on acute respiratory failure, was not selected as the primary outcome because very low rates have been reported since the introduction of noninvasive ventilation for primary respiratory support in AVB [10, 14, 15, 18, 39]. Given these findings, we thought it would be unethical to compare the two devices with low flow oxygen therapy in a control group. We therefore used a set of criteria rather than a single criterion, which may limit comparisons with other studies in this field.
The 15% margin of noninferiority between the devices may also appear generous, but this choice took into account an acceptable risk in the case of HFNC being truly inferior, as the failure criteria did not include a critical outcome like intubation.
Given the noninferiority trial design of this study, the superiority analysis should be interpreted with caution. Indeed, this secondary analysis was conducted to help understand the absence of noninferiority, which remains in any event our primary result. This primary endpoint was evaluated over the short term, but clinical experience indicates that, beyond the initial management, multiple changes in the ventilatory strategy are made to fit the lability of respiratory distress in these infants.
The possibility of switching to alternative respiratory support in the presence of failure criteria may have influenced the secondary outcomes of main clinical interest, like intubation rate, duration of ventilation, and LOS in the PICU. The EDIN score has not been validated in young infants, and a 1-point change in the scale could be considered excessively sensitive. The scale was nevertheless chosen because it is widely used in French PICUs and the age of AVB onset is close to the neonatal period.
Conclusion
This study suggested that nCPAP may be more efficient than HFNC for initial respiratory support in young infants hospitalized in a PICU for moderate to severe AVB. Preemptive respiratory support with nCPAP or HFNC was safe, with very low rates of intubation and skin lesions and the absence of air leak syndrome and death.
References
Hall CB, Simőes EA, Anderson LJ (2013) Clinical and epidemiologic features of respiratory syncytial virus. Curr Top Microbiol Immunol 372:39–57
Pierce HC, Mansbach JM, Fisher ES et al (2015) Variability of intensive care management for children with bronchiolitis. Hosp Pediatr 5:175–184
Hammer J, Numa A, Newth CJ (1997) Acute respiratory distress syndrome caused by respiratory syncytial virus. Pediatr Pulmonol 23:176–183
Stokes GM, Milner AD, Groggins RC (1981) Work of breathing, intra-thoracic pressure and clinical findings in a group of babies with bronchiolitis. Acta Paediatr Scand 70:689–694
Cambonie G, Milési C, Jaber S et al (2008) Nasal continuous positive airway pressure decreases respiratory muscles overload in young infants with severe acute viral bronchiolitis. Intensive Care Med 34:1865–1872
Essouri S, Durand P, Chevret L et al (2011) Optimal level of nasal continuous positive airway pressure in severe viral bronchiolitis. Intensive Care Med 37:2002–2007
Pham TM, O’Malley L, Mayfield S, Martin S, Schibler A (2015) The effect of high flow nasal cannula therapy on the work of breathing in infants with bronchiolitis. Pediatr Pulmonol 50:713–720
Milési C, Matecki S, Jaber S et al (2013) 6 cmH2O continuous positive airway pressure versus conventional oxygen therapy in severe viral bronchiolitis: a randomized trial. Pediatr Pulmonol 48:45–51
Borckink I, Essouri S, Laurent M et al (2014) Infants with severe respiratory syncytial virus needed less ventilator time with nasal continuous airways pressure then invasive mechanical ventilation. Acta Paediatr 103:81–85
Essouri S, Laurent M, Chevret L et al (2014) Improved clinical and economic outcomes in severe bronchiolitis with pre-emptive nCPAP ventilatory strategy. Intensive Care Med 40:84–91
Lee JH, Rehder KJ, Williford L, Cheifetz IM, Turner DA (2013) Use of high flow nasal cannula in critically ill infants, children, and adults: a critical review of the literature. Intensive Care Med 39:247–257
Schlapbach LJ, Schaefer J, Brady AM, Mayfield S, Schibler A (2014) High-flow nasal cannula (HFNC) support in interhospital transport of critically ill children. Intensive Care Med 40:592–599
Milési C, Baleine J, Matecki S et al (2013) Is treatment with a high flow nasal cannula effective in acute viral bronchiolitis? A physiologic study. Intensive Care Med 39:1088–1094
McKiernan C, Chua LC, Visintainer PF, Allen H (2010) High flow nasal cannulae therapy in infants with bronchiolitis. J Pediatr 156:634–638
Schibler A, Pham TM, Dunster KR et al (2011) Reduced intubation rates for infants after introduction of high-flow nasal prong oxygen delivery. Intensive Care Med 37:847–852
Abboud PA, Roth PJ, Skiles CL, Stolfi A, Rowin ME (2012) Predictors of failure in infants with viral bronchiolitis treated with high-flow, high-humidity nasal cannula therapy. Pediatr Crit Care Med 13:e343–e349
Metge P, Grimaldi C, Hassid S et al (2014) Comparison of a high-flow humidified nasal cannula to nasal continuous positive airway pressure in children with acute bronchiolitis: experience in a pediatric intensive care unit. Eur J Pediatr 173:953–958
Mayfield S, Bogossian F, O’Malley L, Schibler A (2014) High-flow nasal cannula oxygen therapy for infants with bronchiolitis: pilot study. J Paediatr Child Health 50:373–378
Bueno Campaña M, Olivares Ortiz J, Notario Muñoz C et al (2014) High flow therapy versus hypertonic saline in bronchiolitis: randomised controlled trial. Arch Dis Child 99:511–515
Hilliard TN, Archer N, Laura H et al (2012) Pilot study of vapotherm oxygen delivery in moderately severe bronchiolitis. Arch Dis Child 97:182–183
Sinha IP, McBride AK, Smith R, Fernandes RM (2015) CPAP and high-flow nasal cannula oxygen in bronchiolitis. Chest 148:810–823
Hough JL, Pham TM, Schibler A (2014) Physiologic effect of high-flow nasal cannula in infants with bronchiolitis. Pediatr Crit Care Med 15:e214–e219
Milési C, Boubal M, Jacquot A et al (2014) High-flow nasal cannula: recommendations for daily practice in pediatrics. Ann Intensive Care 4:29
Hollman G, Shen G, Zeng L et al (1998) Helium-oxygen improves clinical asthma scores in children with acute bronchiolitis. Crit Care Med 26:1731–1736
Debillon T, Zupan V, Ravault N, Magny JF, Dehan M (2001) Development and initial validation of the EDIN scale, a new tool for assessing prolonged pain in preterm infants. Arch Dis Child Fetal Neonatal Ed 85:F36–F41
Khemani RG, Rubin S, Belani S et al (2015) Pulse oximetry vs. PaO2 metrics in mechanically ventilated children: Berlin definition of ARDS and mortality risk. Intensive Care Med 41:94–102
Ganu SS, Gautam A, Wilkins B, Egan J (2012) Increase in use of non-invasive ventilation for infants with severe bronchiolitis is associated with decline in intubation rates over a decade. Intensive Care Med 38:1177–1183
Larrar S, Essouri S, Durand P et al (2006) Effects of nasal continuous positive airway pressure ventilation in infants with severe acute bronchiolitis. Arch Pediatr 13:1397–1403
Bakalli I, Celaj E, Simaku A, Kola E, Sallabanda S (2015) Predictors of noninvasive ventilation success in children with acute respiratory failure. Intensive Care Med 41:950–951
Cambonie G, Milési C, Fournier-Favre S et al (2006) Clinical effects of heliox administration for acute bronchiolitis in young infants. Chest 129:676–682
Black J, Baharestani MM, Cuddigan J et al (2007) National Pressure Ulcer Advisory Panel’s updated pressure ulcer staging system. Adv Skin Wound Care 20:269–274
Donlan M, Fontela PS, Puligandla PS (2011) Use of continuous positive airway pressure (CPAP) in acute viral bronchiolitis: a systematic review. Pediatr Pulmonol 46:736–746
Liet JM, Ducruet T, Gupta V, Cambonie G (2015) Heliox inhalation therapy for bronchiolitis in infants. Cochrane Database Syst Rev 9:CD006915
Collett PW, Perry C, Engel LA (1985) Pressure-time product, flow, and oxygen cost of resistive breathing in humans. J Appl Physiol 58:1263–1272
Beasley JM, Jones SE (1981) Continuous positive airway pressure in bronchiolitis. Br Med J (Clin Res Ed) 283:1506–1508
Schiller O, Levy I, Pollak U, Kadmon G, Nahum E, Schonfeld T (2011) Central apnoeas in infants with bronchiolitis admitted to the paediatric intensive care unit. Acta Paediatr 100:216–219
Ricart S, Rovira N, Garcia-Garcia JJ et al (2014) Frequency of apnea and respiratory viruses in infants with bronchiolitis. Pediatr Infect Dis J 33:988–990
Alansari K, Toaimah FH, Khalafalla H, El Tatawy LA, Davidson BL, Ahmed W (2016) Caffeine for the treatment of apnea in bronchiolitis: a randomized trial. J Pediatr. doi:10.1016/j.jpeds.2016.04.060
Javouhey E, Barats A, Richard N et al (2008) Non-invasive ventilation as primary ventilatory support for infants with severe bronchiolitis. Intensive Care Med 34:1608–1614
Acknowledgements
Members of the Respiratory GFRUP Study Group substantially contributed to study conception, data interpretation, manuscript revision, and final approval. It includes, in addition to the authors of the manuscript, the following members: Guillaume Emeriaud, MD, PhD (Division of Pediatric Critical Care, Department of Pediatrics, Sainte-Justine University Hospital, University of Montréal, Montréal, QC, Canada); Philippe Jouvet, MD, PhD (Division of Pediatric Critical Care, Department of Pediatrics, Sainte-Justine University Hospital, University of Montréal, QC, Canada); Julie Guichoux, MD (Pediatric Intensive Care Unit, Pellegrin University Hospital, Bordeaux, France); Fabrice Michel, MD, PhD (Department of Pediatric Anesthesia, La Timone University Hospital, Marseille, France); Marti Pons Odena, MD, PhD (Pediatric Intensive Care Unit, Hospital Universitario Sant Joan de Deu University Hospital, Barcelona, Spain); Florent Baudin, MD (Pediatric Intensive Care Unit, Women-Mothers & Children’s University Hospital, Lyon, France); Chloe Genier, GN (Pediatric Intensive Care Unit, Women & Children’s University Hospital, Nantes, France); Ingrid Nissen, MD (Pediatric Intensive Care Unit, St Olavs University Hospital, Trondheim, Norway); Olivier Brissaud, MD (Pediatric Intensive Care Unit, Pellegrin University Hospital, Bordeaux, France); Stéphane Dauger MD, PhD (Pediatric Intensive Care Unit, Robert-Debré University Hospital, Paris, France).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Funding source
All phases of this study were supported by Montpellier University Hospital (Grant: research contract 2012–2015). This study has also been supported by Fisher and Paykel Healthcare with the provision of 30 HFNC circuits. Fisher and Paykel was not involved in the study design and had no role in data management, data analysis and data interpretation, nor in the writing of the report and the decision to submit it for publication.
Conflicts of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Additional information
The members of the Respiratory GFRUP Study Group are listed in the acknowledgements and in the electronic supplementary material.
Take-home message: In young infants with acute viral bronchiolitis, the effectiveness of HFNC was not equivalent to that of nCPAP as the initial respiratory support. A majority of the failures with HFNC occurred within 6 h after initiation, and worsening of respiratory distress was the leading cause.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Milési, C., Essouri, S., Pouyau, R. et al. High flow nasal cannula (HFNC) versus nasal continuous positive airway pressure (nCPAP) for the initial respiratory management of acute viral bronchiolitis in young infants: a multicenter randomized controlled trial (TRAMONTANE study). Intensive Care Med 43, 209–216 (2017). https://doi.org/10.1007/s00134-016-4617-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-016-4617-8