
Abstract
Objective
To report our experience of non-invasive ventilation (NIV) as primary ventilatory support strategy in infants admitted for severe bronchiolitis.
Design and setting
Retrospective study in a paediatric intensive care unit of an university hospital.
Patients
Infants aged less than 12 months, admitted for bronchiolitis during 2003–2004 and 2004–2005 winter epidemics.
Intervention
NIV was used as the primary ventilatory support during the second winter (NIV period), whereas invasive ventilation (IV) was the only support employed during the first winter (IV period). NIV consisted in either continuous positive airway pressure (CPAP from 5 to 10 cmH2O) or bilevel positive airway pressure (inspiratory pressure from 12 to 18 cmH2O) with a nasal mask.
Results
During the IV period, 53 infants were included, compared to 27 during the NIV period. The two groups did not differ in age or in number of premature births. Children in NIV group had less apnoea on admission. The intubation rate was reduced during NIV period (p < 0.001). No children had ventilator-associated pneumonia (VAP) during NIV period compared to nine during IV period (p < 0.05). In the NIV group, 10 infants (37%) required supplemental oxygen for more than 8 days compared to 33 children (65%) in IV group (p < 0.05). The length of hospital stay and the duration of ventilation were similar.
Conclusions
In this retrospective study, the use of NIV decreased the rate of ventilator associated pneumonia and reduced the duration of oxygen requirement without prolonging the hospital stay.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In adults, non-invasive ventilation (NIV) has been shown to obviate intubation, to reduce length of hospital stay, and to reduce in-hospital mortality in chronic obstructive pulmonary disease as well as in acute pulmonary oedema [1–4]. Infectious complications of endotracheal intubation are well documented in children as well as in adults [5, 6]. The need for mechanical ventilation is a significant risk factor for developing bronchiolitis obliterans in children with bronchiolitis, mainly due to adenovirus [7]. Small children are more exposed to intubation-related complications [8], which are associated with a longer duration of mechanical ventilation [9]. Although NIV has been widely studied in children with neuromuscular disease or with obstructive sleep apnoea syndrome [10–12], few experiences have been reported on the use of NIV in acute respiratory failure [13–16]. Theoretically, the application of CPAP may maintain the airways open and therefore may facilitate expiratory flow, may improve compliance, and may decrease the work of breathing [17, 18]. McNamara et al. reported an improvement of RSV infection-related apnoea with the use of CPAP [19]. However, experiences of NIV, mainly CPAP, in bronchiolitis are scarce [18, 20–22]. Recently, a randomised controlled trial with cross-over design showed that infants treated by nasal CPAP with moderate bronchiolitis and mild hypercapnoea decreased their pCO2 level. This reduction was better if CPAP was used first than if it was used after a 13-h period with standard treatment [23]. The success rate of NIV in bronchiolitis found in two recent French studies varied from 75 to 83% [24, 25]. Few studies have compared NIV to conventional ventilation in terms of infectious complications, particularly ventilator-associated pneumonia (VAP), and length of hospital stay or oxygen requirement. The aim of this study was to compare an NIV-based ventilatory strategy with an IV-based strategy in terms of rate of complications, duration of oxygen requirement, and duration of ventilatory support [26]. Our hypothesis was that NIV in severe bronchiolitis decreases the rate of PAV and reduces the duration of oxygen requirement, therefore, shortening the hospital stay.
Methods
Setting
This study was performed in a multidisciplinary 10-bed Paediatric Intensive Care Unit of an university teaching hospital which has experience in managing both chronic and acute respiratory failures with NIV. Therefore, all the attending physicians as well as the nurses were well-trained for NIV management.
Patients
Patients younger than 1 year were included in this retrospective study if they were admitted to the PICU for acute respiratory failure or apnoea associated with clinical and radiological signs of bronchiolitis during the 2003–2004 and 2004–2005 winter RSV epidemic seasons (between 1 October and 30 April).
Severe bronchiolitis was defined as the presence of cough, tachypnea, retraction of the chest wall or grunting, wheezing, rales or rhonchi. Infants who presented with SpO2 < 92% in room air were defined as “hypoxemic at admission”. Apnoeas were considered when they were combined with a drop of SpO2 under 90% or if cardiac frequency was observed to be under 90 per minute without stimulation. Ventilatory support was used when these apnoeas continued for more than half an hour despite standard treatment.
In patients with multiple admissions, only the first RSV episode was considered for analysis. Infants in ventilation on tracheotomy, those who had laryngotracheomalacia were excluded (cf. ESM).
Periods of the study
During the first study period, the 2003–2004 epidemic period of RSV infection, the attending physicians usually used endotracheal intubation with mechanical ventilation as the sole ventilatory support strategy. During this period, NIV was never proposed for infants with bronchiolitis, therefore no infant were ventilated by NIV before winter 2004/2005. This period was called “Invasive ventilation (IV) period”. During the second year (2004–2005), referred to as the “Non-invasive ventilation (NIV) period”, the attending physicians were encouraged to use NIV as the primary ventilation support strategy when the infants required ventilatory support. All the medical staff agreed to use NIV as primary ventilatory support in this situation.
Ventilatory support strategies
The decision to initiate ventilation was at the discretion of the attending physician without a priori criteria. During the two study periods, infants were intubated if they were in an impending arrest situation, or if their disease proceeded too rapidly for a trial of NIV.
NIV was delivered by a bilevel positive airway pressure (BiPAP) flow generators (Synchrony®, Respironics, Murrysville, PA or Eclipse, Taema, Nanterre, France). Modes were set up either in continuous (CPAP) or in BiPAP through a nasal mask (Infant nasal mask, Resmed, Sydney, Australia). CPAP was usually started at 5 cmH2O and increased as necessary up to a maximum of 10 cmH2O. If needed, inspiratory positive airway pressure was started at 12 cmH2O and gradually increased to a maximum of 18 cmH2O. A backup rate at 30 and the lowest sensitive flow-trigger were systematically used in BiPAP mode. Humidification was performed using heated humidifier and supplemental oxygen was administered via the circuit to achieve SpO2 of at least 92%. Infants were treated continuously during the first 24 h of NIV followed by periods of spontaneous ventilation which were attempted for at least 1 h twice a day, according to clinical tolerance. NIV failure was defined as the need for endotracheal intubation.
Invasive ventilation was performed using either the Servo900C (Siemens Electra, Uppsala, Sweden), or Evita 4 (Dräger, Lubeck, Germany) with either pressure or volume controlled modes. When the infants had a normal conscious level, without signs of bacterial infection, and when the FiO2 level decreased fewer than 30%, a weaning procedure was started, using a progressive decrease of ventilatory rate or of inspiratory pressure. When the infants maintained adequate SpO2 (FiO2 < 30% to maintain SpO2 > 92%) and respiratory rate with minimal pressure (inspiratory pressure <16 cmH2O) or ventilatory rate (15 or 20 cycles/min), they were extubated.
Standard treatment of bronchiolitis
All infants included were in dorsal 30° proclivity, received continuous enteral feedings via naso or oro-gastric tubes, and chest physiotherapy in order to clear secretions using forced expiratory technique. Infants intubated and ventilated were sedated using midazolam and sometimes received morphinomimetics or oral hydroxyzine. Infants in NIV were not sedated. Following the French consensus conference on the management of infant bronchiolitis, corticosteroids and caffeine were never used [27].
Data collection and end-points
Data collected for each infant included age, history of prematurity, other risk factors of severe bronchiolitis (chronic lung disease, congenital heart disease, immunocompromised states) [28], and presenting symptoms (apnoea, oxygen requirement, atelectasis).The study end-points included rates of bacterial pneumonia (bacterial pulmonary co-infection and VAP), duration of oxygen requirement, duration of ventilatory support, and hospital length of stay (LOS).
Bacterial pulmonary co-infections were defined as the presence of at least two of the following signs in infants with worsening gas exchange: fever>38°C or hypothermia, new or progressive infiltrate or consolidation at chest X-ray, and increased C-reactive protein up to 30 mg/l. These criteria were usually used to start antibiotics. VAP was defined as the occurrence of bacterial pulmonary co-infection more than 48 h after initiation of a ventilatory support. Bacterial analysis of tracheal aspirates was conducted for intubated infants who met the criteria for bacterial pneumonia.
Statistical analysis
Results of quantitative variables were expressed in median values, and first- and third quartiles. Categorical values were compared using Chi-square test or Fischer exact test when relevant. For continuous variables, t test, Kruskal–Wallis and Wilcoxon Signed-Ranks test were used. We have calculated for our criteria of bacterial pneumonia the positive likelihood ratio, which is the sensitivity divided by 1 − specificity, and its 95% confidence interval (95%CI). A p value of <0.05 was considered statistically significant.
Results
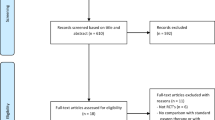
Over the two periods 87 infants were admitted in PICU for bronchiolitis. Two infants with ventilation on tracheotomy, three with laryngo-tracheomalacia, and two infants who received NIV only after extubation were excluded (Cf. ESM). During IV period, 53 infants were included compared to 27 during NIV period.
During the IV period, 47 (89%) infants were intubated compared to 14 (52%) during the NIV period (p < 0.001). During the second year, 15 (56%) infants were treated with NIV. Median duration of NIV was 10 h (0–65). The rate of RSV infection, as confirmed by ELISA detection, was 72% for each study period without difference in the distribution of type A and type B virus. One child died during IV period. None died during the NIV period.
There was no difference in presenting symptoms between the two populations except for apnoea on admission which was more frequent in the first group (Tables 1, 2). Infants in the IV group were more likely to require oxygen therapy after 8 days (Table 2). Bacterial pulmonary co-infections were similar over the two periods. Among the 31 specimens identified in tracheal aspirates from IV group infants, we found 14 Haemophilus influenzae, 6 Streptococcus pneumoniae, 5 Staphylococcus aureus, 3 Branhamella catharralis, and 3 other specimens. Only four infants were considered infected according to our criteria when no bacteria could be identified. The likelihood ratio of bacterial pulmonary infection criteria was 3.28 (95%CI 1.02–12.43). After excluding the nine infants who had been intubated at admission, no VAP was found in the NIV group, compared to nine in the IV group (p < 0.05).
NIV was successful for ten children (group 1), five patients required intubations despite NIV (group 2), and nine were directly intubated (group 3) (Table 3). Two infants only received CPAP (one success), the 13 others required BiPAP ventilation (seven success). Three infants were not ventilated. Infants who were intubated prior to their admission to the PICU (group 3) tended to require oxygen therapy more frequently than those who were treated with NIV (78 vs. 40%, p = 0.17). The ventilatory support duration was longer for infants who failed to NIV compared to those for whom NIV was successful (Table 3). Among the five infants who failed to NIV, two had bacterial pulmonary co-infection of whom one had concomitant urinary infection. The two others had history of prematurity and heart disease, and presented with severe apnoea.
Discussion
In our PICU, a ventilation strategy based on NIV as the primary ventilation support in infants with severe bronchiolitis was associated with a lower rate of ventilator-associated pneumonia, with a shortened duration of supplemental oxygen and with a trend of a reduction in the length of hospital stay.
Previous studies carried out in adults with COPD had shown that NIV may reduce the rates of bacterial pulmonary infections and improve the survival [6, 29, 30]. For children, the mean duration of mechanical ventilation and PICU stay is longer for patients with VAP [31, 32]. The rates of bacterial pulmonary co-infection observed in our study (28% in IV group, 22% in the NIV group) are consistent with previous studies [5, 33–35]. Kneyber et al. showed that infants with a positive culture (blood or endotracheal aspirate) were ventilated 4 days longer than those for whom bacteriological documentation was not obtained (difference not statistically significant) [34]. The presence of bacterial pneumonia did not influence the hospital stay of infants with severe bronchiolitis in a previous study [5]. On the contrary, Thorburn et al. found that children with bacterial co-infection (40%) required ventilatory support for a longer period than those with RSV only [33]. Using bacteriological data and polymorphonuclear neurophil count obtained from endotracheal sputum specimens, Randolph et al. found 17.5% of probable bacterial pneumonia and 20.6% of possible bacterial pneumonia in children intubated for a severe bronchiolitis [36]. Criteria used for the definition of acquired pneumonia in these studies were mainly based on bacteriological data obtained by tracheal aspirates. On the other hand, in our study, bacterial pulmonary co-infections were defined without any bacteriological criteria. However, the positive predictive value for bacterial identification of our criteria was more than 80%. We used the same criteria over the two study periods. The lack of bacteriological criteria was justified by the inability to obtain comparable bacteriological criteria for children treated by NIV and those managed by IV. The definition of nosocomial pneumonia proposed by the Centre for Disease Control (CDC) is difficult to apply to infants admitted for severe bronchiolitis because it does not allow us to distinguish between a bacterial pneumonia and a pulmonary viral infection [37]. The clinical and vital signs used in these criteria are those we used to determine admission of infants with bronchiolitis to the PICU. Clinical criteria are likely to be sensitive but have a lower specificity [36]. This is probably the reason why, at present, no study has been carried out on VAP in children with bronchiolitis using the CDC criteria. The reduction of VAP rate found in our study is probably due to the absence of tracheal tube. Infants admitted to PICU during both periods were similarly co-infected by bacterial at admission, and the PICU admission delays were similar in both groups.
A ventilation strategy based on NIV as the primary ventilation support was associated with a decrease on oxygen requirement greater than 8 days and tended to reduce the LOS, as previously shown [25]. The use of sedative drugs in intubated infants can explain this difference. However, this was not associated with a significant reduction in ventilation duration. The lack of a standardised weaning protocol for infants treated by NIV and the low duration of ventilation in IV group (almost 4 days) can both explain the absence of reduction in ventilation duration with NIV [5, 25, 33, 34]. No study has previously reported weaning strategy for children in acute respiratory failure treated by NIV. The reason why the duration of ventilatory support was not reduced in our study, whereas the rate of VAP was decreased is unclear. One possible explanation is that VAP was over-diagnosed given that we used clinico-biological criteria. Another hypothesis is that colonisation may lead to a weak impact of VAP on the outcome of infants ventilated for a severe bronchiolitis. Otherwise, the fact that we found a longer duration of ventilatory support to be associated with NIV failure suggests that it might be better to assess the response to NIV earlier. This recommendation is consistent with the results of previous studies on NIV in children for acute respiratory failure [13, 15]. The median hospital LOS (12 days for IV and NIV group) was higher than those recently reported [5, 35, 38]. The hospital stay of infants with bronchiolitis can be prolonged because of many reasons, such as feeding troubles, social problems, or differences in the discharged policy.
Our results do not seem to be explained by a lower severity in infants during the NIV period. The risk factors of severe RSV infection are mostly related to preexisting factors [28, 39, 40]. Indeed, base-line characteristics as age, premature birth, were similar in the two groups, except for apnoea on admission. This difference could mitigate our result even though, no study has shown that infants with apnoeas on admission had a shorter length of hospital stay, neither more pulmonary bacterial infections [40, 41]. Infants younger than 2 months were reported to be the strongest independent risk factor for RSV associated apnoea, but not infections [40]. The PRISM II scores, the rates of ventilatory support requirement and of bacterial pulmonary co-infection on admission were similar in both groups. Moreover, the rate of RSV infection and the distribution of type A and B virus did not differ between groups.
This study is limited by the retrospective nature of data and by the small sample sizes. Some biological data on admission, particularly blood gas analysis, are lacking. No written standardised protocols were used to set up and to wean from IV or NIV over the two study periods. However, the study was undertaken in the same PICU, with the same physicians over two successive years so that we can assume that habits did not change over the study.
Our experience on a ventilation support strategy based on NIV in infants admitted for severe viral bronchiolitis suggests that NIV may be an alternative to invasive ventilation. This strategy was associated with a lower rate of VAP and a shorter duration of oxygen therapy. Prospective controlled trial will be crucial to confirm the efficiency of NIV compared with intubation, and to assess potential benefits in length of ICU and hospital stay.
References
American Thoracic Society, the European Respiratory Society, the European Society of Intensive Care Medicine, the Société de Réanimation de Langue Française (2001) International Consensus Conferences in Intensive Care Medicine: noninvasive positive pressure ventilation in acute Respiratory failure. Am J Respir Crit Care Med 163:283–291
Bersten AD, Holt AW, Vedig AE, Skowronski GA, Baggoley CJ (1991) Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med 325:1825–1830
Brochard L, Mancebo J, Wysocki M, Lofaso F, Conti G, Rauss A, Simonneau G, Benito S, Gasparetto A, Lemaire F et al. (1995) Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med 333:817–822
Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito JA (2005) Noninvasive ventilation in acute cardiogenic pulmonary edema: systematic review and meta-analysis. JAMA 294:3124–3130
Duttweiler L, Nadal D, Frey B (2004) Pulmonary and systemic bacterial co-infections in severe RSV bronchiolitis. Arch Dis Child 89:1155–1157
Girou E, Schortgen F, Delclaux C, Brun-Buisson C, Blot F, Lefort Y, Lemaire F, Brochard L (2000) Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA 284:2361–2367
Colom AJ, Teper AM, Vollmer WM, Diette GB (2006) Risk factors for the development of bronchiolitis obliterans in children with bronchiolitis. Thorax 61:503–506
Black AE, Hatch DJ, Nauth-Misir N (1990) Complications of nasotracheal intubation in neonates, infants and children: a review of 4 years’ experience in a children’s hospital. Br J Anaesth 65:461–467
Rivera R, Tibballs J (1992) Complications of endotracheal intubation and mechanical ventilation in infants and children. Crit Care Med 20:193–199
Fauroux B, Pigeot J, Polkey MI, Roger G, Boule M, Clement A, Lofaso F (2001) Chronic stridor caused by laryngomalacia in children: work of breathing and effects of noninvasive ventilatory assistance. Am J Respir Crit Care Med 164:1874–1878
Essouri S, Nicot F, Clement A, Garabedian EN, Roger G, Lofaso F, Fauroux B (2005) Noninvasive positive pressure ventilation in infants with upper airway obstruction: comparison of continuous and bilevel positive pressure. Intensive Care Med 31:574–580
Bach JR, Niranjan V (2000) Spinal muscular atrophy type I: a noninvasive respiratory management approach. Chest 117:1100–1105
Bernet V, Hug MI, Frey B (2005) Predictive factors for the success of noninvasive mask ventilation in infants and children with acute respiratory failure. Pediatr Crit Care Med 6:660–664
Fortenberry JD, Del Toro J, Jefferson LS, Evey L, Haase D (1995) Management of pediatric acute hypoxemic respiratory insufficiency with bilevel positive pressure (BiPAP) nasal mask ventilation. Chest 108:1059–1064
Essouri S, Chevret L, Durand P, Haas V, Fauroux B, Devictor D (2006) Noninvasive positive pressure ventilation: five years of experience in a pediatric intensive care unit. Pediatr Crit Care Med 7:329–334
Padman R, Lawless ST, Kettrick RG (1998) Noninvasive ventilation via bilevel positive airway pressure support in pediatric practice. Crit Care Med 26:169–173
Leclerc F, Scalfaro P, Noizet O, Thumerelle C, Dorkenoo A, Fourier C (2001) Mechanical ventilatory support in infants with respiratory syncytial virus infection. Pediatr Crit Care Med 2:197–204
Soong WJ, Hwang B, Tang RB (1993) Continuous positive airway pressure by nasal prongs in bronchiolitis. Pediatr Pulmonol 16:163–166
McNamara F, Sullivan CE (1997) Nasal CPAP treatment in an infant with respiratory syncytial virus-associated apnea. Pediatr Pulmonol 24:218–221
Pirret AM, Sherring CL, Tai JA, Galbraith NE, Patel R, Skinner SM (2005) Local experience with the use of nasal bubble CPAP in infants with bronchiolitis admitted to a combined adult/paediatric intensive care unit. Intensive Crit Care Nurs 21:314–319
Kristensen K, Dahm T, Frederiksen PS, Ibsen J, Iyore E, Jensen AM, Kjaer BB, Olofsson K, Pedersen P, Poulsen S (1998) Epidemiology of respiratory syncytial virus infection requiring hospitalization in East Denmark. Pediatr Infect Dis J 17:996–1000
Beasley JM, Jones SE (1981) Continuous positive airway pressure in bronchiolitis. Br Med J (Clin Res Ed) 283:1506–1508
Thia LP, McKenzie SA, Blyth TP, Minasian CC, Kozlowska WJ, Carr SB (2007) Randomised controlled trial of nasal continuous positive airways pressure (CPAP) in bronchiolitis. Arch Dis Child 93:45–47
Campion A, Huvenne H, Leteurtre S, Noizet O, Binoche A, Diependaele JF, Cremer R, Fourier C, Sadik A, Leclerc F (2006) Non-invasive ventilation in infants with severe infection presumably due to respiratory syncytial virus: feasibility and failure criteria. Arch Pediatr 13:1404–1409
Larrar S, Essouri S, Durand P, Chevret L, Haas V, Chabernaud JL, Leyronnas D, Devictor D (2006) Effects of nasal continuous positive airway pressure ventilation in infants with severe acute bronchiolitis. Arch Pediatr 13:1397–1403
Barats A, Javouhey E, Richard N, Stamm D, Floret D (2006) Non-invasive ventilation in infants with severe bronchiolitis. In: 8th European pediatric conference in pediatric and neonatal ventilation, Montreux, Switzerland March 29–April 1 2006
Stagnara J, Balagny E, Cossalter B, Dommergues JP, Dournel C, Drahi E, Gauchez H, Guillot F, Javault D, Lagardère B, Le Masne A, Lesprit E, Maidenberg M, Maufroy D, Picherot G, Renaud H, Undreiner F (2001) Management of bronchiolitis in the infant. Recommendations. Long text. Arch Pediatr 8(Suppl1):11S–23S
Welliver RC (2003) Review of epidemiology and clinical risk factors for severe respiratory syncytial virus (RSV) infection. J Pediatr 143:S112–S117
Brochard L (2003) Mechanical ventilation: invasive versus noninvasive. Eur Respir J Suppl 47:31s–37s
Antonelli M, Conti G, Rocco M, Bufi M, De Blasi RA, Vivino G, Gasparetto A, Meduri GU (1998) A comparison of noninvasive positive-pressure ventilation and conventional mechanical ventilation in patients with acute respiratory failure. N Engl J Med 339:429–435
Almuneef M, Memish ZA, Balkhy HH, Alalem H, Abutaleb A (2004) Ventilator-associated pneumonia in a pediatric intensive care unit in Saudi Arabia: a 30-month prospective surveillance. Infect Control Hosp Epidemiol 25:753–758
Tullu MS, Deshmukh CT, Baveja SM (2000) Bacterial nosocomial pneumonia in Paediatric Intensive Care Unit. J Postgrad Med 46:18–22
Thorburn K, Harigopal S, Reddy V, Taylor N, van Saene HK (2006) High incidence of pulmonary bacterial co-infection in children with severe respiratory syncytial virus (RSV) bronchiolitis. Thorax 61:611–615
Kneyber MC, Blusse van Oud-Alblas H, van Vliet M, Uiterwaal CS, Kimpen JL, van Vught AJ (2005) Concurrent bacterial infection and prolonged mechanical ventilation in infants with respiratory syncytial virus lower respiratory tract disease. Intensive Care Med 31:680–685
Randolph AG, Reder L, Englund JA (2004) Risk of bacterial infection in previously healthy respiratory syncytial virus-infected young children admitted to the intensive care unit. Pediatr Infect Dis J 23:990–994
Rello J, Paiva JA, Baraibar J, Barcenilla F, Bodi M, Castander D, Correa H, Diaz E, Garnacho J, Llorio M, Rios M, Rodriguez A, Sole-Violan J (2001) International conference for the development of consensus on the diagnosis and treatment of ventilator-associated pneumonia. Chest 120:955–970
Langley JM, Bradley JS (2005) Defining pneumonia in critically ill infants and children. Pediatr Crit Care Med 6:S9–S13
Chevret L, Mbieleu B, Essouri S, Durand P, Chevret S, Devictor D (2005) Bronchiolitis treated with mechanical ventilation: prognosis factors and outcome in a series of 135 children. Arch Pediatr 12:385–390
Navas L, Wang E, de Carvalho V, Robinson J (1992) Improved outcome of respiratory syncytial virus infection in a high-risk hospitalized population of Canadian children. Pediatric Investigators Collaborative Network on Infections in Canada. J Pediatr 121:348–354
Kneyber MC, Brandenburg AH, de Groot R, Joosten KF, Rothbarth PH, Ott A, Moll HA (1998) Risk factors for respiratory syncytial virus associated apnoea. Eur J Pediatr 157:331–335
Kneyber MC, Moons KG, de Groot R, Moll HA (2002) Prediction of duration of hospitalization in respiratory syncytial virus infection. Pediatr Pulmonol 33:453–457
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at: doi:10.1007/s00134-008-1152-2.
This work was accepted for a poster presentation in the XXXIV° congrès de la Société de Réanimation de Langue Française (SRLF). Paris-la Défense, 18–20 janvier 2006 (Réanimation vol 14, suppl 1, SP126) and for an oral presentation in the 8th European Conference in Paediatric and Neonatal Ventilation, 29 Mars–01 Avril 2006, Montreux, Switzerland.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Javouhey, E., Barats, A., Richard, N. et al. Non-invasive ventilation as primary ventilatory support for infants with severe bronchiolitis. Intensive Care Med 34, 1608–1614 (2008). https://doi.org/10.1007/s00134-008-1150-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1150-4