
Abstract
Purpose
To determine the incidence of and risk factors for adverse cardiac events during catecholamine vasopressor therapy in surgical intensive care unit patients with cardiovascular failure.
Methods
The occurrence of any of seven predefined adverse cardiac events (prolonged elevated heart rate, tachyarrhythmia, myocardial cell damage, acute cardiac arrest or death, pulmonary hypertension-induced right heart dysfunction, reduction of systemic blood flow) was prospectively recorded during catecholamine vasopressor therapy lasting at least 12 h.
Results
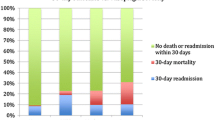
Fifty-four of 112 study patients developed a total of 114 adverse cardiac events, an incidence of 48.2 % (95 % CI, 38.8–57.6 %). New-onset tachyarrhythmia (49.1 %), prolonged elevated heart rate (23.7 %), and myocardial cell damage (17.5 %) occurred most frequently. Aside from chronic liver diseases, factors independently associated with the occurrence of adverse cardiac events included need for renal replacement therapy, disease severity (assessed by the Simplified Acute Physiology Score II), number of catecholamine vasopressors (OR, 1.73; 95 % CI, 1.08–2.77; p = 0.02) and duration of catecholamine vasopressor therapy (OR, 1.01; 95 % CI, 1–1.01; p = 0.002). Patients developing adverse cardiac events were on catecholamine vasopressors (p < 0.001) and mechanical ventilation (p < 0.001) for longer and had longer intensive care unit stays (p < 0.001) and greater mortality (25.9 vs. 1.7 %; p < 0.001) than patients who did not.
Conclusions
Adverse cardiac events occurred in 48.2 % of surgical intensive care unit patients with cardiovascular failure and were related to morbidity and mortality. The extent and duration of catecholamine vasopressor therapy were independently associated with and may contribute to the pathogenesis of adverse cardiac events.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cardiovascular failure is one of the leading causes of death in surgical intensive care unit (SICU) patients [1]. Aside from fluids, the vast majority of pharmacological agents used to treat cardiovascular failure are catecholamine derivatives or drugs interacting with adrenergic post-receptor pathways [2]. Despite their widespread use [3], catecholamine vasopressor drugs carry a high potential to induce adverse side effects and increase the risk of in-hospital mortality [4]. As a result of the ubiquitous distribution of adrenergic receptors, catecholamine-associated side effects can impair several organ functions, but are most serious when affecting heart function [5].
Adverse cardiac events may include prolonged elevated heart rate, tachyarrhythmia, myocardial ischemia and cell damage, cardiac arrest, pulmonary artery hypertension-induced right heart dysfunction, and reduction of systemic blood flow [5]. Adverse cardiac events can perpetuate cardiovascular failure and worsen patient outcome. Although the potential of catecholamine vasopressors to induce adverse side effects in general, and adverse cardiac events in particular, is well known, their actual incidence has not been systematically reported thus far. Determination of the true burden of adverse cardiac events during catecholamine vasopressor therapy could help clinicians to better assess the risk of unwanted adrenergic effects affecting the heart and stimulate research to identify alternative non-adrenergic treatment strategies for cardiovascular failure.
In this prospective observational study, the incidence of seven predefined adverse cardiac events was systematically evaluated in 112 consecutive SICU patients with cardiovascular failure during catecholamine vasopressor therapy. Furthermore, we sought to determine independent risk factors for the occurrence of adverse cardiac events and appraise the association between catecholamine vasopressor exposure as well as different catecholamine vasopressor drugs and the occurrence of adverse cardiac events. Our hypothesis was that adverse cardiac events frequently occur during catecholamine vasopressor therapy and that catecholamine vasopressor support is associated with both morbidity and mortality.
Patients and methods
This prospective observational study was performed between January 1 and December 31, 2009, in a 12-bed general and surgical ICU in a tertiary university teaching hospital. The study protocol was reviewed by the Ethics Committee of Innsbruck Medical University. Since no blood was sampled, patient treatment was not affected by study enrollment, and as exclusively anonymous data were retrieved, written informed consent was waived.
Inclusion and exclusion criteria
All SICU patients with cardiovascular failure—defined as a mean arterial pressure less than 65 mmHg despite adequate fluid resuscitation and blood flow requiring catecholamine vasopressor therapy for at least 12 h—were eligible for study enrollment. Catecholamine vasopressor therapy was defined as infusion of one or more of the following drugs: norepinephrine, epinephrine, phenylephrine, and/or dopamine at dosages greater than 5 µg/kg/min. Age less than 18 years, pregnancy, non-surgical critical illness, and limitation/withholding of intensive care therapy were exclusion criteria.
Hemodynamic and general patient management
The institutional hemodynamic management has been described before [6]. SICU patients with cardiovascular failure were routinely monitored with an arterial and central venous line. A pulmonary artery or transpulmonary thermodilution catheter (PiCCO plus®; Pulsion, Munich, Germany) was placed at the discretion of the attending physician. Transesophageal echocardiography was used liberally in patients without cardiac output measurement. Fluid resuscitation was performed according to the response of arterial blood pressure, filling pressures (e.g., central venous pressure, pulmonary arterial occlusion pressure), stroke volume variation, and/or stroke volume/cardiac index to repetitive fluid loading using crystalloids or gelatine-based colloids (Gelofusin®; B. Braun, Melsungen, Germany). If cardiac index remained less than 2–2.5 L/min/m2 or central/mixed venous oxygen saturation was less than 60 % despite volume loading and/or blood transfusion, milrinone (0.3–0.7 µg/kg/min) and/or epinephrine was continuously infused. Norepinephrine (Arterenol®; Sanofi-Aventis, Frankfurt, Germany) was infused to increase mean arterial blood pressure to greater than 60–65 mmHg. In septic shock, hydrocortisone (200–300 mg/day) was added as a continuous infusion if escalating norepinephrine doses could not stabilize hemodynamic function. On the basis of clinical symptoms, erythrocyte concentrates were transfused to maintain hemoglobin above 70 g/L. Endotracheally intubated patients were sedated, whenever required, by infusing sufentanil and midazolam or morphine alone. Continuous veno-venous hemofiltration (CVVH) was employed for renal indications only.
Data documentation
Upon study enrollment, the following data were collected in all patients: age, gender, body mass index, premorbid conditions, type of surgery, cause of cardiovascular failure, the Simplified Acute Physiology Score II (SAPS II) [7], the Sequential Organ Failure Assessment (SOFA) score [8], heart rate, mean arterial blood pressure, central venous pressure, serum troponin T concentrations (Modular E, Roche Diagnostics GmbH, Mannheim, Germany; detection limit 5–10,000 ng/L), the type, dose, and number of catecholamine vasopressor drugs infused, the overall catecholamine vasopressor load, as well as the need for mechanical ventilation, intra-aortic balloon pump and/or renal replacement therapy. Because different catecholamine vasopressor drugs were used, the overall catecholamine vasopressor load was calculated according to the formula suggested by Russell et al. [9]: vasopressor load (µg/kg/min) = norepinephrine (µg/kg/min) + [dopamine (µg/kg/min/kg)]/2 + epinephrine (µg/kg/min) + [phenylephrine (µg/kg/min)]/10. Upon SICU discharge, the duration of catecholamine vasopressor therapy and mechanical ventilation, length of SICU stay, and mortality were documented.
Adverse cardiac events
Using a standardized protocol, we recorded the occurrence of any of the following adverse cardiac events during catecholamine vasopressor therapy: prolonged elevated heart rate, tachyarrhythmia, myocardial cell damage, acute cardiac arrest, acute cardiac death, pulmonary artery hypertension-induced right heart dysfunction, and reduction of systemic blood flow (Table 1). Each time an adverse cardiac event occurred, the type and dose of the catecholamine vasopressor infused as well as the overall catecholamine vasopressor load was recorded.
Statistical analysis
Assuming a 50 % incidence of adverse cardiac events during catecholamine vasopressor therapy [10, 11], a sample size calculation revealed that inclusion of 110 patients could predict the incidence of adverse cardiac events with a 95 % confidence interval (CI) extending by 9.3 % in both directions.
All statistical analyses were performed with the SPSS software package (SPSS 13.0.1; SPSS Inc., Chicago, Illinois, USA). Descriptive methods were applied to determine the incidence of adverse cardiac events. Comparisons between patients with or without adverse cardiac events as well as between specific subgroups (patients with or without cardiac surgery, patients with or without chronic cardiovascular diseases) were performed using the Mann–Whitney U test, Fisher’s exact test, and the chi-squared test, as applicable. To determine independent risk factors for the occurrence of adverse cardiac events, a multivariate logistic regression model was calculated. Variables showing significant (p < 0.1) or clinically relevant differences between patients with or without adverse cardiac events in a bivariate analysis (for statistical tests applied see above) were included in the multivariate regression model. If variables exhibited collinearity between each other (correlation coefficient greater than 0.4) the one with the highest correlation coefficient was included in the multivariate regression model. Since we sought to specifically evaluate the association between catecholamine vasopressor exposure and the occurrence of adverse cardiac events, regression models were built for each aspect of catecholamine vasopressor exposure (vasopressor load at study enrollment, number of catecholamine vasopressors infused at study enrollment, duration of catecholamine vasopressor therapy) and each catecholamine vasopressor drug (binary use and dose at study enrollment). p values less than 0.05 were considered to indicate statistical significance. All data are presented as median values with interquartile ranges (IQRs), unless otherwise indicated.
Results
During the observation period, 422 patients were admitted to the SICU. One hundred and twelve patients (26.5 %) were eligible for enrollment and were included. One hundred and fourteen new-onset adverse cardiac events occurred in 54 patients during catecholamine vasopressor therapy (Table 2), an incidence of 48.2 % (95 % CI, 38.8–57.6 %). No difference in the rate and type of adverse cardiac events was observed between patients with or without cardiac surgery as well as between patients with or without chronic cardiovascular diseases (Table 2). In 17 patients, an adverse cardiac event already existed at study enrollment. These patients could only be screened for the development of other adverse cardiac events.
Patients developing one or more adverse cardiac events more frequently suffered from chronic liver diseases and had a higher SAPS II than patients without adverse cardiac events (Table 3). At study enrollment, patients who subsequently developed adverse cardiac events presented with higher heart rates and serum troponin T concentrations, were treated with epinephrine more frequently and with phenylephrine at a higher dosage, received more catecholamine vasopressors simultaneously, had higher vasopressor loads and SOFA scores, and required continuous veno-venous hemofiltration more often than patients who did not develop adverse cardiac events (Table 4). Until SICU discharge, patients experiencing adverse cardiac events required catecholamine vasopressor therapy and mechanical ventilation for a longer time, stayed in the SICU longer, and had higher mortality than those without adverse cardiac events (Table 4).
The vasopressor load at the time adverse cardiac events occurred differed between single adverse cardiac events (Fig. 1). Chronic liver disease, need for renal replacement therapy, the SAPS II, the number of catecholamine vasopressor drugs infused at study enrollment, and the duration of catecholamine vasopressor therapy were independently associated with the occurrence of adverse cardiac events (Table 5; Fig. 2). When binary use and the dose of single vasopressive agents at study enrollment were introduced into the multivariate model, use of epinephrine (OR 3.35; CI 95 % 1.27–8.87; p = 0.02) and the dose of phenylephrine (OR 2.1; CI 95 % 1.04–4.26; p = 0.04) were independently associated with the occurrence of adverse cardiac events.

Median values and IQRs of vasopressor loads at occurrence of single adverse cardiac events. *Significant difference in the vasopressor load at occurrence of single adverse cardiac events; PEHR prolonged elevated heart rate (n = 56), aMI acute myocardial ischemia and cell damage (n = 27), TA tachyarrhythmia (n = 20), RedSBF reduction in systemic blood flow (n = 6). The vasopressor load at occurrence of acute cardiac arrest [n = 4; 0.1 (0.03–0.22) µg/kg/min] and pulmonary artery hypertension-induced right heart dysfunction (n = 1; 0.34 µg/kg/min) were not included because of their low incidence

Incidence of adverse cardiac events as predicted by catecholamine vasopressor exposure (adjusted logistic regression models). *Independent association with the occurrence of adverse cardiac events. Each logistic regression model was adjusted for the SAPS II, need for continuous veno-venous hemofiltration, and presence of chronic liver disease. Quartiles of catecholamine vasopressor load: 1, ≤0.12 µg/kg/min; 2, 0.13–0.25 µg/kg/min; 3, 0.26–0.45 µg/kg/min; 4, ≥0.46 µg/kg/min; quartiles of duration of vasopressor therapy: 1, ≤61 h; 2, 66–151 h; 3, 158–346 h; 4, ≥348 h
Discussion
In this prospective observational study, a 48.2 % incidence of adverse cardiac events was detected in 112 SICU patients with cardiovascular failure during catecholamine vasopressor therapy. Patients who developed adverse cardiac events had higher catecholamine vasopressor loads, were on catecholamine vasopressor drugs for longer, and had greater morbidity and mortality than patients who did not. In addition to chronic liver disease, need for renal replacement therapy, and disease severity (assessed by the SAPS II), the number of catecholamine vasopressor agents infused and the duration of catecholamine vasopressor therapy were independently associated with adverse cardiac events. Of the four vasopressor agents applied, epinephrine and phenylephrine were associated with the occurrence of adverse cardiac events.
The finding that nearly half of our study population developed adverse cardiac events during catecholamine vasopressor therapy should stimulate reflection. In view of the current lack of alternative drugs to treat cardiovascular failure, catecholamine vasopressor agents should be used judiciously, and catecholamine-sparing strategies should be pursued. Such strategies may include the enforcement of adequate fluid and inotropic resuscitation, targeting reasonable cardiovascular endpoints (e.g., tissue perfusion instead of arbitrary arterial blood pressure targets), and the avoidance of practices which again might increase the need for catecholamine vasopressors (e.g., non-targeted sedation). In addition, future research is required to identify alternative vasopressive drugs for the treatment of cardiovascular failure.
Considering that this study specifically evaluated adverse cardiac events, the true incidence of adverse systemic events during catecholamine vasopressor therapy is likely to be even higher, as suggested by other studies [9, 12–14]. Since this was an observational study, no conclusions on the cause of adverse cardiac events can be drawn. Cardiovascular failure [15, 16], disease severity [17–19], acute kidney injury [20], and chronic liver diseases [21] have been associated with cardiac pathologies and, as suggested by the multivariate regression model, played a role in the pathogenesis of adverse cardiac events in this population as well. Pharmacologic effects of catecholamine vasopressors on the heart would support a causative association with the occurrence of adverse cardiac events [22–27]. Such drug-related effects may influence the heart directly through stimulation of alpha and beta receptors [27] or indirectly through alpha-receptor-mediated vasoconstriction and increased ventricular afterload [28, 29]. These negative effects might be reduced by a catecholamine-sparing treatment regimen through adding vasopressin to the treatment plan which has been shown to significantly reduce norepinephrine requirement without increasing the risk of serious adverse events in vasodilatory shock states [30].
Although indicated by a weak trend in the adjusted regression model, an independent association between the catecholamine vasopressor dose at study enrollment and the development of adverse cardiac events was not observed. There may be several reasons for the absence of a dose–response effect in our study. First, the catecholamine vasopressor doses included in the regression models were not recorded at the time the adverse cardiac event occurred. Second, single adverse cardiac events occurred at different vasopressor doses, indicating that a wide range of critical catecholamine doses can induce single adverse cardiac events. Furthermore, moderate r 2 values (0.3–0.44) suggest that other factors not included in the regression models played a role in the pathogenesis of adverse cardiac events during catecholamine vasopressor therapy. Interestingly, these factors do not appear to include specific surgical subpopulations (e.g., cardiovascular surgery) or common chronic conditions such as arterial hypertension, coronary artery disease, or congestive heart failure, but may comprise individual factors such as genetic predisposition [31].
In view of the small number of patients receiving single vasopressive agents, data on the association between particular catecholamine agents and the occurrence of adverse cardiac events must be interpreted with caution. In our analysis, epinephrine and phenylephrine were the catecholamine agents independently associated with the occurrence of adverse cardiac events. While the binary use but not the dose of epinephrine was associated with the occurrence of adverse cardiac events, phenylephrine was linked with the occurrence of adverse cardiac events in a dose-dependent fashion. Although no causative association has so far been proven in the clinical setting, adverse cardiac events have been reported with both catecholamine agents [32–34].
The two adverse cardiac events most frequently observed in this study were tachyarrhythmia and prolonged elevated heart rate, both of which were correlated with significant morbidity and mortality. A close relationship between the use of catecholamine vasopressor drugs and the occurrence of tachycardia and/or tachyarrhythmia has been reported by several authors [35, 36]. Particularly striking was the 17.9 % incidence of myocardial cell damage, as reflected by increases in troponin T serum levels during catecholamine vasopressor therapy. Given that troponin T serum levels can be influenced by renal function, we chose to consider only relevant (greater than 25 %) increases in serum troponin T levels to reflect myocardial cell damage. In cardiac surgery patients, this was done 48 h after surgery, a time interval during which troponin usually decreases [37]. Indeed, troponin T levels increased by a median percentage of 52 % (95 % CI, 28–99 %) in patients with detectable troponin T at study enrollment (n = 8).
Given that a reduction in systemic blood flow and pulmonary artery hypertension-induced right heart dysfunction could only be detected in patients monitored with a pulmonary artery or transpulmonary thermodilution catheter, it must be assumed that the true incidence of these adverse cardiac events was underestimated in our population. Compared to other adverse cardiac events, however, the incidence of pulmonary artery hypertension-induced right heart dysfunction appears low, suggesting that this may not be a common complication during catecholamine vasopressor therapy. Myocardial stunning, diastolic dysfunction, and increased afterload may all explain persistent reductions in systemic blood flow during vasopressor infusion [25]. Although most studies evaluating the effect of catecholamine vasopressors, such as norepinephrine, on hemodynamics reported unchanged or increased cardiac output [38], our data indicate that at least some patients may experience a relevant reduction in systemic blood flow which may, in conjunction with peripheral vasoconstriction, precipitate tissue hypoperfusion.
Additional limitations need to be considered when interpreting our study results. By enrolling 112 patients, we could report the incidence of adverse cardiac events during catecholamine vasopressor therapy with a 95 % CI of 39–58 %. Inclusion of a larger patient population would have allowed more accurate determination of the incidence of adverse cardiac events. Taking into account that an incidence in the lower ranges of the 95 % CI would still be clinically relevant, inclusion of more patients would have most likely not changed the clinical conclusion of this study. The list of adverse cardiac events systematically screened for in this study is incomplete and lacks pathologies which are difficult to assess at the bedside (e.g., myocardial cell apoptosis [39]). Furthermore, our results cannot be extrapolated to other non-SICU populations. Surgery triggers a systemic inflammatory response which may itself predispose to the development of adverse cardiac events during catecholamine vasopressor therapy. Despite considering multiple constellations of various vasopressive agents, different adverse cardiac events, and finally different confounding factors, we failed to identify a critical cumulative dose of a particular vasopressive agent or a particular combination of vasopressive agents which was associated with adverse cardiac events. Finally, the reported incidence of adverse cardiac events during catecholamine vasopressor therapy must be closely interpreted together with the institutional hemodynamic protocol applied. It is conceivable that the incidence of adverse cardiac events varies if different resuscitation strategies are applied.
In conclusion, adverse cardiac events occur in almost half of SICU patients during catecholamine vasopressor therapy and are related to both morbidity and mortality. Although our study cannot prove a causative relationship, the extent and duration of catecholamine vasopressor therapy were independently associated with and may contribute to the pathogenesis of adverse cardiac events. Clinicians need to be aware of this high incidence of adverse cardiac events when starting SICU patients on catecholamine vasopressor drugs.
References
Mayr VD, Dünser MW, Greil V, Jochberger S, Luckner G, Ulmer H, Friesenecker BE, Takala J, Hasibeder WR (2006) Causes of death and determinants of outcome in critically ill patients. Crit Care 10:R154
Dellinger RP, Levy MM, Carlet JM et al (2008) Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock. Crit Care Med 36:296–327
Torgersen C, Dünser MW, Schmittinger CA, Pettilä V, Ruokonen E, Wenzel V, Jakob SM, Takala J (2011) Current approach to the haemodynamic management of septic shock patients in European intensive care units: a cross-sectional, self-reported questionnaire-based survey. Eur J Anaesthesiol 28:284–290
Mebazaa A, Parissis J, Porcher R, Gayat E, Nikolaou M, Boas FV, Delgado JF, Follath F (2011) Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med 37:290–301
Dünser MW, Hasibeder WR (2009) Sympathetic overstimulation during critical illness: adverse effects of adrenergic stress. J Intensive Care Med 24:293–316
Torgersen C, Dünser MW, Wenzel V, Jochberger S, Mayr V, Schmittinger CA, Lorenz I, Schmid S, Westphal M, Grander W, Luckner G (2010) Comparing two different arginine vasopressin doses in advanced vasodilatory shock: a randomized, controlled, open-label trial. Intensive Care Med 36:57–65
Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG (1996) The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 22:707–710
Russell JA, Walley KR, Singer J, Gordon AC, Hébert PC, Cooper DJ, Holmes CL, Mehta S, Granton JT, Storms MM, Cook DJ, Presneill JJ, Ayers D, VASST Investigators (2008) Vasopressin versus norepinephrine infusion in patients with septic shock. N Engl J Med 358:877–887
Dünser MW, Mayr AJ, Ulmer H, Ritsch N, Knotzer H, Pajk W, Luckner G, Mutz NJ, Hasibeder WR (2001) The effects of vasopressin on systemic hemodynamics in catecholamine-resistant septic and postcardiotomy shock: a retrospective analysis. Anesth Analg 93:7–13
Dünser MW, Mayr AJ, Stallinger A, Ulmer H, Ritsch N, Knotzer H, Pajk W, Mutz NJ, Hasibeder WR (2002) Cardiac performance during vasopressin infusion in postcardiotomy shock. Intensive Care Med 28:746–751
Annane D, Vignon P, Renault A, Bollaert PE, Charpentier C, Martin C, Troché G, Ricard JD, Nitenberg G, Papazian L, Azoulay E, Bellissant E, CATS Study Group (2007) Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomised trial. Lancet 370:676–684
De Backer D, Biston P, Devriendt J, Madl C, Chochrad D, Aldecoa C, Brasseur A, Defrance P, Gottignies P, Vincent JL, SOAPII Investigators (2010) Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med 362:779–789
Dünser MW, Ruokonen E, Pettilä V, Ulmer H, Torgersen C, Schmittinger CA, Jakob S, Takala J (2009) Association of arterial blood pressure and vasopressor load with septic shock mortality: a post hoc analysis of a multicenter trial. Crit Care 13:R181
Bay M, Kirk V, Parner J, Hassager C, Nielsen H, Krogsgaard K, Trawinski J, Boesgaard S, Aldershvile J (2003) NT-proBNP: a new diagnostic screening tool to differentiate between patients with normal and reduced left ventricular systolic function. Heart 89:150–154
Talwar S, Squire IB, Downie PF, Mccullough AM, Campton MC, Davies JE, Barnett DB, Ng LL (2000) Profile of plasma N-terminal proBNP following acute myocardial infarction; correlation with left ventricular systolic dysfunction. Eur Heart J 21:1514–1521
Chua G, Kang-Hoe L (2004) Marked elevations in N-terminal brain natriuretic peptide levels in septic shock. Crit Care 8:R248–R250
Januzzi JL, Morss A, Tung R, Pino R, Fifer MA, Thompson BT, Lee-Lewandrowski E (2006) Natriuretic peptide testing for the evaluation of critically ill patients with shock in the intensive care unit: a prospective cohort study. Crit Care 10:R37
Wolff B, Haase D, Lazarus P, Machill K, Graf B, Lestin HG, Werner D (2007) Severe septic inflammation as a strong stimulus of myocardial NT-pro brain natriuretic peptide release. Int J Cardiol 122:131–136
Ronco C (2011) Cardio-renal syndromes: from foggy bottoms to sunny hills. Heart Fail Rev 16:509–517
Zardi EM, Abbate A, Zardi DM, Dobrina A, Margiotta D, Van Tassell BW, Afeltra A, Sanyal AJ (2010) Cirrhotic cardiomyopathy. J Am Coll Cardiol 56:539–549
Iwai-Kanai E, Hasegawa K, Araki M, Kakita T, Morimoto T, Sasayama S (1999) Alpha- and beta-adrenergic pathways differentially regulate cell type-specific apoptosis in rat cardiac myocytes. Circulation 100:305–311
Mann DL, Kent RL, Parsons B, Cooper G 4th (1992) Adrenergic effects on the biology of the adult mammalian cardiocyte. Circulation 85:790–804
Okamoto T, Adachi K, Muraishi A, Seki Y, Hidaka T, Toshima H (1996) Induction of DNA breaks in cardiac myoblast cells by norepinephrine. Biochem Mol Biol Int 38:821–827
Power I, Kam P (2001) Cardiovascular physiology. In: Power I, Kam P (eds) Principles of physiology for the anaesthetist. Arnold, London, pp 99–165
Sander O, Welters ID, Foëx P, Sear JW (2005) Impact of prolonged elevated heart rate on incidence of major cardiac events in critically ill patients with a high risk of cardiac complications. Crit Care Med 33:81–88; discussion 241–242
Opie L (2004) Receptors and signal transduction. In: Opie L (ed) Heart physiology. From cell to circulation. Lippincott Williams and Wilkins, Philadelphia, pp 186–220
Flavahan NA, Cooke JP, Shepherd JT, Vanhoutte PM (1987) Human postjunctional alpha-1 and alpha-2 adrenoceptors: differential distribution in arteries of the limbs. J Pharmacol Exp Ther 241:361–365
Polito A, Parisini E, Ricci Z, Picardo S, Annane D (2012) Vasopressin for treatment of vasodilatory shock: an ESICM systematic review and meta-analysis. Intensive Care Med 38:9–19
Schreuder WO, Schneider AJ, Groeneveld AB, Thijs LG (1989) Effect of dopamine vs norepinephrine on hemodynamics in septic shock. Emphasis on right ventricular performance. Chest 95:1282–1288
Nakada TA, Russell JA, Boyd JH, Aguirre-Hernandez R, Thain KR, Thair SA, Nakada E, McConechy M, Walley KR (2010) β2-Adrenergic receptor gene polymorphism is associated with mortality in septic shock. Am J Respir Crit Care Med 181:143–149
Levy B, Perez P, Perny J, Thivilier C, Gerard A (2011) Comparison of norepinephrine-dobutamine to epinephrine for hemodynamics, lactate metabolism, and organ function variables in cardiogenic shock. A prospective, randomized pilot study. Crit Care Med 39:450–455
Navarro-Sobrino M, Lorita J, Soley M, Ramírez I (2010) Catecholamine-induced heart injury in mice: differential effects of isoproterenol and phenylephrine. Histol Histopathol 25:589–597
Zdanowicz JA, Utz AC, Bernasconi I, Geier S, Corti R, Beinder E (2011) “Broken heart” after cesarean delivery. Case report and review of literature. Arch Gynecol Obstet 283(4):687–694
Culling W, Penny WJ, Cunliffe G, Flores NA, Sheridan DJ (1987) Arrhythmogenic and electrophysiological effects of alpha adrenoceptor stimulation during myocardial ischaemia and reperfusion. J Mol Cell Cardiol 19:251–258
Mayr A, Knotzer H, Pajk W, Luckner G, Ritsch N, Dünser M, Ulmer H, Schobersberger W, Hasibeder W (2001) Risk factors associated with new onset tachyarrhythmias after cardiac surgery—a retrospective analysis. Acta Anaesthesiol Scand 45:543–549
Peivandi AA, Dahm M, Opfermann UT, Peetz D, Doerr F, Loos A, Oelert H (2004) Comparison of cardiac troponin I versus T and creatine kinase MB after coronary artery bypass grafting in patients with and without perioperative myocardial infarction. Herz 29:658–664
Martin C, Viviand X, Arnaud S, Vialet R, Rougnon T (1999) Effects of norepinephrine plus dobutamine or norepinephrine alone on left ventricular performance of septic shock patients. Crit Care Med 27:1708–1713
Goldspink DF, Burniston JG, Ellison GM, Clark WA, Tan LB (2004) Catecholamine-induced apoptosis and necrosis in cardiac and skeletal myocytes of the rat in vivo: the same or separate death pathways? Exp Physiol 89:407–416
Conflicts of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schmittinger, C.A., Torgersen, C., Luckner, G. et al. Adverse cardiac events during catecholamine vasopressor therapy: a prospective observational study. Intensive Care Med 38, 950–958 (2012). https://doi.org/10.1007/s00134-012-2531-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-012-2531-2