
Abstract
Purpose
Diagnosis of pneumothorax relies on clinical suspicion and chest X-ray, and is often delayed. We aimed to determine whether electrical impedance tomography (EIT) can accurately identify the presence of surgically created pneumothoraces before significant changes in clinical parameters.
Methods
Six anesthetized and muscle-relaxed piglets with surfactant-depleted lungs were studied. Following chest drain insertion into the right ventral chest, 10–20 ml aliquots of air were instilled into the pleural space to a maximum volume of 200 ml. The pneumothorax was drained by attaching a Heimlich valve to the chest drain. At each instillation and after draining the pneumothorax, global and regional end-expiratory intra-thoracic volumes (EEV) were measured using respiratory inductive plethysmography (RIP) and EIT concurrently with \( {\text{Sp}}_{{{\text{O}}_{2} }} \), heart rate and blood pressure.
Results
A significantly greater change in both global EEVRIP and EEV within the right ventral quadrant was seen at all volume instillations, from as little as 10 ml, compared with all other quadrants. There was no difference in EEV within the left ventral and both dorsal quadrants. \( {\text{Sp}}_{{{\text{O}}_{2} }} \) fell below 90% at 100 ml instillation. Tachycardia occurred at 140 ml instillation. EIT identified a 60% resolution of pneumothoraces within 60 s of attachment of the Heimlich valve.
Conclusions
EIT accurately detects very small pneumothoraces before physiological parameters change.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pneumothoraces are a frequent complication in infants with respiratory distress, with reported rates of between 0.5–1% in term [1] and 4–14% in preterm infants [2–4]. Pneumothoraces increase the risk of mortality [5, 6] and neurological morbidity [7]. They occur in infants who are mechanically ventilated and in spontaneously breathing infants receiving continuous positive airway pressure (CPAP) [6, 8–10]. The presentation may be sudden or slow in onset. The clinical signs of pneumothorax are non-specific, and a reliable real-time diagnostic tool is lacking. Transillumination of the chest is usually reserved for deteriorating infants, when the pneumothorax is likely to be large or under tension. Interpretation is operator dependent and associated with high false-negative and false-positive rates [11]. Chest X-ray (CXR) is considered the gold standard diagnostic test, but access is often delayed [12].
Early detection is important as a delay in pneumothorax recognition can have harmful consequences, including cardiovascular collapse and hypoxia [13]. Electrical impedance tomography (EIT) is a real-time radiation-free technique that that can detect changes in lung volume non-invasively at the bedside [14]. EIT allows imaging of regional volumetric change by generating cross-sectional images of the changes in distribution of electrical impedance within the thorax [15]. Recently, we and others [16, 17] have shown that EIT has sufficient resolution to detect regional differences in tidal ventilation and aeration in preterm infants. EIT has been validated for the imaging of pathologic pulmonary air against computed tomography (CT) [18] and scintigraphy [19]. Costa et al. [20] have demonstrated the usefulness of a custom-built EIT in the real-time detection of pneumothoraces in a larger adult animal model, but did not evaluate its utility in determining resolution of the pneumothorax. The ability of EIT to detect pathological pulmonary air in the infant lung has not been evaluated. Detection of a pneumothorax before clinical deterioration occurs may reduce the risk of long-term harm in this vulnerable population.
This study aimed to determine, in a surfactant-depleted piglet lung model, (1) whether EIT could accurately identify the location and resolution of surgically created pneumothoraces of varying sizes and (2) to compare the ability of EIT to detect pneumothoraces with other bedside monitoring tools.
Methods
A detailed description of the experimental protocol can be found in the Electronic Supplementary Material (ESM) online.
The study was performed in the Animal Research Laboratory Facility at the Royal Children’s Hospital, Melbourne, Australia, after approval by the institution’s animal ethics committee and adhered to national codes of practice as outlined by the Australian National Health and Medical Research Council.
Five-week-old piglets [n = 6; mean (SD) weight 5.0 (1.2) kg] were anesthetized, sedated and mechanically ventilated in the supine position in 1.0 fraction inspired oxygen (\( {\text{F}}_{{{\text{IO}}_{ 2} }} \)) using time-cycled pressure-limited ventilation (TCPL; VIP Bird Gold, Viasys Healthcare, Yorba Linda, CA, USA). Median (IQR) peak end-expiratory pressure (PEEP) was set at 6 (5–7) cm H2O, and peak inspiratory pressure (PIP) was adjusted to achieve tidal volumes (V T) of 6–10 ml/kg (Florian Respiratory Mechanics monitor, Acutronic Medical Systems, Hirzel, Switzerland) and a PaCO2 between 45 and 55 mmHg. The ventilator rate was set at 40 inflations per min.
Measurements
Oxygen saturation (\( {\text{Sp}}_{{{\text{O}}_{2} }} \)), heart rate (HR) and mean arterial blood pressure (ABP) were continuously measured (HP48S monitor, Hewlett Packard, Andover, MA, USA). Electrical impedance tomography (EIT; Geo MF II EIT system, Cardinal Health, Hoechberg, Germany) sampling at 25 Hz was used to measure regional relative impedance change (∆Z) [21]. DC-coupled respiratory inductive plethysmography (RIP; Respitrace 200, Non-invasive Monitoring Systems Inc., North Bay Village, FL, USA), sampling at 200 Hz, was used to measure changes in global end-expiratory intra-thoracic volume (∆EEVRIP) and tidal volume (V TRIP) [22, 23].
Pneumothorax model
A closed chest drain (10FG) was inserted 2–3 cm into the right ventral chest approximately 5 cm below the EIT electrodes at the anterior axillary line and angled superiorly and anteriorly by a single operator (GMS). This resulted in the tip of the chest drain lying immediately below the EIT electrodes in the right ventral thorax and was confirmed in the first animal by autopsy. Increasing amounts of air were instilled into the pleural space every 5 min in 10-ml aliquots to a volume of 20 ml and then 20-ml aliquots to a maximum accumulated volume of 200 ml. Aliquot instillation was ceased at a lower accumulated volume if severe cardio-respiratory deterioration occurred. This model is similar to that used previously by Costa et al. [20] and Liu et al. [24]. At the maximum instillation tolerated, a Heimlich valve (Pneumostat Chest Drain Valve, Atrium Medical Corp., NH, USA) was attached to the chest drain to relieve the pneumothorax. \( {\text{F}}_{{{\text{IO}}_{ 2} }} \) and ventilator settings were not altered during the protocol. Each animal served as its own control. The animals were humanely euthanized at the end of the study using an overdose of intravenous pentobarbital sodium.
Data and statistical analyses
\( {\text{Sp}}_{{{\text{O}}_{2} }} \), HR, ABP, EEVRIP and V TRIP were digitized (Powerlab 16/30, AD Instruments, Sydney, Australia) and continuously recorded at 200 Hz during each instillation and for 90 s afterwards using LabChart 7® (AD Instruments, Sydney, Australia). EEVRIP during each measurement period was referenced to the EEVRIP prior to the first instillation of intra-pleural air (baseline) to determine the ΔEEVRIP caused by the addition of each aliquot. V TRIP was defined as the average tidal trough to peak value for each measurement period.
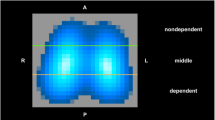
The EIT data were analyzed offline, reconstructed to create a cross-sectional image of the chest using proprietary software (AUSPEX Version 1.5, Cardinal Health, Hoechberg, Germany) [25, 26] and the cross-sectional slices of the thorax divided into four regions of interest for comparison, namely the right and left ventral and dorsal quadrants. Relative end-expiratory intra-thoracic volume (ΔZ EEVroi), in countless units (c.u), within each region was determined from the trough of the time course signal referenced to the baseline impedance values.
Regional changes in tidal ventilation within each quadrant were calculated from the tidal impedance amplitude and expressed as a percentage of the mean global impedance amplitude for each recording (∆Z VTroi%). For example, a ΔZ VTroi of 30% in the right ventral quadrant represents a V T of 30% of the global V T. Finally, functional EIT (fEIT) images of each recording were generated to create a visual display of relative ventilation and aeration within the thorax using a colorimetric scale [20].
Differences at each instillation volume were compared with a repeated measures ANOVA or Kruskal-Wallis test, and Bonferroni or Dunn’s multiple comparison post-tests, as appropriate. The relationship between changes in volumetric values against time was assessed using linear regression analysis. Statistical analysis was performed using GraphPad Prism version 4.02 for Windows (GraphPad software, San Diego, CA, USA). A p value <0.05 was considered significant.
Results
Four piglets completed the entire study protocol to 200 ml instillation. Two piglets only tolerated 120 ml instillation before rapid clinical deterioration. The alveolar-arterial oxygen difference (AaDO2) prior to surgical creation of the pneumothorax was mean (SD) 451.4 (174) mmHg. No intra-subject variability was seen in ∆P during the study.
Physiological parameters
The baseline mean (SD) \( {\text{Sp}}_{{{\text{O}}_{2} }} \) was 95 (3)% and remained stable up to 80 ml instilled air. A significant deterioration in \( {\text{Sp}}_{{{\text{O}}_{2} }} \) to 89 (6)% occurred at 100 ml instillation (p < 0.001; Bonferroni post-test). A significant increase in HR from baseline occurred at 140 ml instillation: mean (SD) HR 245 (44) bpm, compared with 200 (54) bpm at baseline (p = 0.001; Bonferroni post-test). In the animals that completed the protocol, ABP did not significantly change during the entire protocol.
Respiratory inductive plethysmography
ΔEEVRIP (ml/kg) at each volume instillation is shown in the Electronic Supplementary Material (ESM Figure A). There was a significant increase in ΔEEVRIP at each volume instillation from a mean (SD) 3 (1) ml/kg increase after 10 ml instillation of air to 20 (7) ml/kg by 200 ml (p < 0.0001 ANOVA). V TRIP fell from a median (interquartile range; IQR) 11 (9, 15) ml/kg at baseline to 9 (6, 13) ml/kg after 100 ml of intra-pleural air had been instilled (p < 0.05; Dunn’s multiple comparison test); thereafter, it did not change significantly.
Electrical impedance tomography
Global ∆ZEEV increased linearly with each volume instillation (ESM Figure A; line of best fit r 2 0.96; slope 0.288). A mean (SD) global ∆Z EEV of 9 (4) c.u. occurred after a 10 ml instillation of air. This increased to 66 (51) c.u. by 200 ml instillation (p < 0.0001, Bonferroni post-test).
Figure 1 shows that at all volume instillations, mean ΔZ EEV within the right ventral quadrant was significantly higher than in all other quadrants (p < 0.0001; Bonferroni post-test). In all animals, there was a similar relationship between volume instilled and regional change in intra-thoracic volume (r 2 0.701–0.985). A significantly greater increase in ΔZ EEV was identified in the EIT time-course signal in the right ventral quadrant after as little as a 10 ml instillation (p < 0.0001; Bonferroni post-test).

Relative change in regional thoracic volume in countless impedance units (c.u.) during the instillation of increasing volumes of air to induce a pneumothorax. In the right ventral quadrant (closed diamonds), resolution is seen following drainage with a Heimlich valve. An instillation volume of 100 and 140 ml, respectively, was required to initiate a significant decrease in \( {\text{Sp}}_{{{\text{O}}_{2} }} \) and heart rate, respectively (long and medium dashed lines). Data mean ± SEM. Solid lines represent line of best fit (linear regression model) within each region and the dashed lines the 95% confidence interval. Within the right ventral region of interest, the r 2 was 0.940 (slope = 0.29)
No statistically significant differences were seen in the ∆Z VTroi% in the right ventral and right dorsal quadrants. The ∆Z VTroi% in the right ventral quadrant was mean (SD) 30 (7)% at baseline and fell to 26 (10)% at 200 ml. In the right dorsal quadrant, ∆Z VT was 22 (18)% at baseline, 19 (14)% at 10 ml instillation and 20 (14)% at 200 ml. The ∆Z VTroi% trended to fall in the left ventral quadrant at increasing volumes with a concomitant increase in the left dorsal quadrant.
Resolution of the pneumothorax
There was a significant fall in ΔEEVRIP from mean (SD) 20 (7) ml/kg at 200 ml instillation to 4 (13) ml/kg 60 s after attachment of the Heimlich valve (ESM Figure A). V TRIP improved by 0.5 ml/kg but remained significantly lower than at baseline (p < 0.001; Bonferroni post-test).
Within 60 s of attaching the Heimlich valve to the chest drain, ΔZ EEV in the right ventral quadrant fell from mean (SD) 46 (39.5) to 18.3 (20.5) c.u., suggesting a 60% resolution of the pneumothorax (p < 0.001; Bonferroni post-test). No significant change was seen in the other three quadrants. ΔZ EEV in the regional EIT time course signal in each quadrant following drainage of the pneumothorax in a representative animal is shown in Fig. 2.

Change in the regional EIT time-course signal in each quadrant (dotted line) following use of a Heimlich valve to drain the induced pneumothorax in a representative animal. The trough of the EIT signal represents end-expiratory intra-thoracic volume and the amplitude tidal ventilation within that region. Maximal change in end-expiratory intra-thoracic volume and tidal ventilation occurred in the right ventral quadrant (location of pneumothorax)
Functional EIT images
The fEIT images displayed reduction in ventilation with incremental intra-pleural gas instillations within the right ventral quadrant and resolution after drainage (Fig. 3a). Aeration maps (Fig. 3b) demonstrated accumulation of intra-pleural air as well as resolution when the Heimlich valve was attached.

a Representative functional EIT (fEIT) images of the regional changes in ventilation (from left to right) prior to instillation of any intrapleural gas (baseline), instillation of a total of 200 ml of gas into the right ventral intrapleural space and after attachment of a Heimlich valve. Regional volumetric change is demonstrated using a colorimetric scale that ranges from dark blue (minimum) to red (maximum). These images demonstrate a reduction of tidal ventilation in the right ventral quadrant associated with the 200 ml intrapleural gas and evolving improvement with drainage. b fEIT of aeration during the same phases demonstrating the presence of right ventral quadrant intrapleural gas that is not engaged in tidal ventilation after 200 ml accumulated instillation
Discussion
This study found that, in an animal model of neonatal lung injury, it was possible to detect the magnitude and location of pneumothoraces as small as 10 ml in size using EIT. This was significantly smaller than the pneumothorax volume that resulted in a change in the parameters (HR and \( {\text{Sp}}_{{{\text{O}}_{2} }} \)), which are routinely used to guide clinicians. We also found that it was possible to monitor resolution of the pneumothorax and observe the re-emergence of tidal ventilation in the affected lung after drainage of the extra-pleural gas. To our knowledge, the time course of drainage and re-expansion of the lung post drainage of a pneumothorax have not been previously described.
The detection of pneumothoraces is currently based on clinical suspicion and chest radiography. Typically, an infant receiving respiratory support starts to deteriorate slowly with non-specific signs and symptoms. Various maneuvers, including repositioning the infant, changing or recalibrating the monitoring devices and suctioning the infant, may occur before a pneumothorax is considered. Transillumination may be attempted, but is an unreliable test for small pneumothoraces. A CXR is ultimately obtained to confirm the diagnosis. The delay between onset of pneumothorax and confirmation on CXR may be considerable.
It is essential that better methods for early detection of a pneumothorax are developed. Detection using pulmonary acoustic transmission [27] or computerized analysis of breath sounds [28] have been investigated in animal models and found to be promising, but neither have been studied in infants. Our study suggests that the use of EIT may accurately identify the location of pneumothorax, potentially allowing the diagnosis of pneumothoraces to be made earlier, before clinical signs develop. EIT may also identify successful drainage of the pneumothorax.
EIT is not widely available, cannot be calibrated to a known volume and the regional values generated are relative rather than absolute. To account for this, we used RIP to demonstrate that a progressive global change in thoracic volume occurred as we induced the pneumothorax. Our data show that the global EIT signal demonstrated a similar pattern to the RIP signal. EIT was able to detect pneumothoraces as small as 10 ml in volume in our pediatric ARDS experimental model, a finding that is similar to that of Costa and co-workers in an adult pig model [20]. Total lung capacity in our piglet model is of the order of 60 ml/kg [29], and therefore, it may be argued that a pneumothorax 10 ml (~2 ml/kg in this model) in size may be clinically irrelevant. Although EIT cannot be calibrated to a known volume, it is still possible to use it to provide relative measurements. As a result, it may not detect a pre-existing pneumothorax (that is, one existing prior to attachment of the EIT device to the patient) but will detect a change in the size of an existing pneumothorax. It may be useful to provide continuous monitoring of known small pneumothoraces that are being managed expectantly [30]. We have also shown that EIT has utility in determining resolution of the pneumothorax once drained. The use of EIT has the added advantage of limiting radiation exposure from repeated CXR in a susceptible population.
In its current form, EIT reports behavior within a single slice of the chest. In our study we intentionally created an artificial pneumothorax within the region of sampling. In the clinical environment it is possible a pneumothorax may occur outside the monitoring region. Paradoxically, more of the chest will be included in the EIT sampling region in the neonate compared with the adult. EIT has been used in preterm infants less than 1 kg [16], but EIT electrode application is difficult and accurate positioning important, with the most validated location being around the chest at the level of the nipples. This may interfere with the insertion of the chest tube. It must also be recognized that changes in intra-thoracic blood volume and pulmonary blood flow can also influence EIT signals. These issues need to be overcome before EIT can be useful as a clinical tool.
Others have recommended monitoring \( {\text{Sp}}_{{{\text{O}}_{2} }} \), PaO2 [24] and transcutaneous carbon dioxide tension trends to detect early pneumothoraces [12]. Clinically, arterial blood gas sampling is an intermittent investigation; as such, we elected not to measure arterial blood gases after each instillation. An instillation of at least 20 ml/kg into the pleural space was shown to be required to result in an appreciable decrease in \( {\text{Sp}}_{{{\text{O}}_{2} }} \) [24]. In contrast, HR does not decrease until the pneumothorax volume reaches approximately 40 ml/kg [24]. Our study was consistent with these findings. Arguably the most appropriate time to intervene is before the pneumothorax becomes large enough to cause blood gas parameters to deteriorate and expose the infant to resultant significant complications. In this context, EIT may have utility in conjunction with standard cardio-respiratory monitoring.
In four animals we did not observe a change in ABP during the entire study protocol in this muscle-relaxed and sedated model. However, in two animals a rapid deterioration in all cardiovascular parameters occurred at 120 ml of intra-pleural air. This is in contrast to a previous report of a sustained elevated ABP lasting up to 2 h, associated with pneumothoraces prior to thoracocentesis in spontaneously ventilating infants [31].
The major limitation of this study is that this is an artificial pneumothorax model and as such there may be differences in lung behavior when compared with the spontaneous pneumothorax. It is important to note that the behavior of the lung may differ during the development of a slow, progressive pneumothorax compared with lung behavior during a rapid onset tension pneumothorax. It may be that this difference in lung behavior may explain the lack of any major change in ΔZ VTroi% during the study. Our data suggest there may be regional compression of the lung (Fig. 2), and EIT may be useful in further defining this observation.
The use of EIT to document a spontaneous pneumothorax in an infant has been described [32]. In our study, similar EIT results were found. Also, CXR currently remains the gold standard for diagnosis of a pneumothorax, and no CXR or other imaging was performed on these piglets. However, in a clinical scenario, CXRs are usually performed after clinical deterioration occurs and provide information only at the moment it is taken, rather than to document evolution of the event. CXRs are also not a reliable method of quantifying subtle changes in intra-thoracic volume during mechanical ventilation [33]. We conducted a pragmatic study and used RIP, which is the only non-invasive, commercially available bedside tool that can be calibrated with good correlation to a known volume [34] to determine changes in thoracic volume. Although RIP detected as little as 10 ml instillation of air, it cannot differentiate the location or cause of a volume change. Given the compressibility of lung tissue and the circulatory system within the chest, the strong linear relationship between instillation and thoracic volumes was unexpected. This may be due to a compliant chest wall in our animal model.
There are some limitations to the EIT algorithm we used. The algorithm is known to over-represent the middle regions of the thorax. A pneumothorax is likely to influence peripheral lung regions initially. These issues may account for the difference in fEIT and Z VTroi% results, given the lower spatial resolution in the latter. It is likely clinicians would use the fEIT display as a clinical monitor.
Conclusion
This study shows that EIT can accurately detect and localize small pneumothoraces before clinical changes occur. EIT also allows monitoring of the resolution of the pneumothorax. Further studies are required to determine if EIT can be used to accurately detect pneumothoraces in an infant population and guide ventilation practices following drainage of the pneumothorax.
Abbreviations
- AaDO2 :
-
Alveolar-arterial oxygen gradient
- ABP:
-
Arterial blood pressure
- Bpm:
-
Beats per minute
- ∆Z :
-
Relative impedance change
- CXR:
-
Chest X-ray
- CI:
-
Confidence interval
- c.u:
-
Countless units
- EEV:
-
End-expiratory intra-thoracic volume
- EEVroi:
-
End-expiratory intra-thoracic volume (region of interest)
- EIT:
-
Electrical impedance tomography
- \( {\text{F}}_{{{\text{IO}}_{ 2} }} \) :
-
Fraction of inspired oxygen
- HR:
-
Heart rate
- IQR:
-
Inter-quartile range
- IPPV:
-
Intermittent positive pressure ventilation
- PEEP:
-
Positive end expiratory pressure
- PIP:
-
Positive inspiratory pressure
- RIP:
-
Respiratory inductive plethysmography
- SD:
-
Standard deviation
- \( {\text{Sp}}_{{{\text{O}}_{2} }} \) :
-
Oxygen saturations
- TCPL:
-
Time cycled pressure limited
- V T :
-
Tidal volume
- V TRIP :
-
Tidal volume as measured by RIP
- ∆Z VTroi :
-
Tidal volume as measured by EIT (region of interest)
References
Katar S, Devecioglu C, Kervancioglu M, Ulku R (2006) Symptomatic spontaneous pneumothorax in term newborns. Pediatr Surg Int 22:755–758
Horbar JD, Badger GJ, Carpenter JH, Fanaroff AA, Kilpatrick S, LaCorte M, Phibbs R, Soll RF (2002) Trends in mortality and morbidity for very low birth weight infants, 1991–1999. Pediatrics 110:143–151
Watkinson M, Tiron I (2001) Events before the diagnosis of a pneumothorax in ventilated neonates. Arch Dis Child Fetal Neonatal Ed 85:F201–F203
Klinger G, Ish-Hurwitz S, Osovsky M, Sirota L, Linder N (2008) Risk factors for pneumothorax in very low birth weight infants. Pediatr Crit Care Med 9:398–402
Powers WF, Clemens JD (1993) Prognostic implications of age at detection of air leak in very low birth weight infants requiring ventilatory support. J Pediatr 123:611–617
Bhatia R, Davis PG, Doyle LW, Wong C, Morley CJ (2011) Identification of pneumothorax in very preterm infants. J Pediatr 159:115–120
Hill A, Perlman JM, Volpe JJ (1982) Relationship of pneumothorax to occurrence of intraventricular hemorrhage in the premature newborn. Pediatrics 69:144–149
Finer NN et al (2010) Early CPAP versus surfactant in extremely preterm infants. N Engl J Med 362:1970–1979
Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB (2008) Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med 358:700–708
Rojas MA et al (2009) Very early surfactant without mandatory ventilation in premature infants treated with early continuous positive airway pressure: a randomized, controlled trial. Pediatrics 123:137–142
Wyman ML, Kuhns LR (1977) Accuracy of transillumination in the recognition of pneumothorax and pneumomediastinum in the neonate. Clin Pediatr (Phila) 16:323–324
McIntosh N, Becher JC, Cunningham S, Stenson B, Laing IA, Lyon AJ, Badger P (2000) Clinical diagnosis of pneumothorax is late: use of trend data and decision support might allow preclinical detection. Pediatr Res 48:408–415
Ogata ES, Gregory GA, Kitterman JA, Phibbs RH, Tooley WH (1976) Pneumothorax in the respiratory distress syndrome: incidence and effect on vital signs, blood gases, and pH. Pediatrics 58:177–183
Wolf GK, Arnold JH (2005) Noninvasive assessment of lung volume: respiratory inductance plethysmography and electrical impedance tomography. Crit Care Med 33:S163–S169
Frerichs I (2000) Electrical impedance tomography (EIT) in applications related to lung and ventilation: a review of experimental and clinical activities. Physiol Meas 21:R1–R21
Armstrong RK, Carlisle HR, Davis PG, Schibler A, Tingay DG (2011) Distribution of tidal ventilation during volume-targeted ventilation is variable and influenced by age in the preterm lung. Intensive Care Med 37:839–846
Miedema M, de Jongh FH, Frerichs I, van Veenendaal MB, van Kaam AH (2011) Changes in lung volume and ventilation during lung recruitment in high-frequency ventilated preterm infants with respiratory distress syndrome. J Pediatr 159:199–205
Hahn G, Just A, Dudykevych T, Frerichs I, Hinz J, Quintel M, Hellige G (2006) Imaging pathologic pulmonary air and fluid accumulation by functional and absolute EIT. Physiol Meas 27:S187–S198
Hinz J, Neumann P, Dudykevych T, Andersson LG, Wrigge H, Burchardi H, Hedenstierna G (2003) Regional ventilation by electrical impedance tomography: a comparison with ventilation scintigraphy in pigs. Chest 124:314–322
Costa EL et al (2008) Real-time detection of pneumothorax using electrical impedance tomography. Crit Care Med 36:1230–1238
Frerichs I, Dargaville PA, Dudykevych T, Rimensberger PC (2003) Electrical impedance tomography: a method for monitoring regional lung aeration and tidal volume distribution? Intensive Care Med 29:2312–2316
Tingay DG, Mills JF, Morley CJ, Pellicano A, Dargaville PA (2006) The deflation limb of the pressure-volume relationship in infants during high-frequency ventilation. Am J Respir Crit Care Med 173:414–420
Tingay DG, Copnell B, Mills JF, Morley CJ, Dargaville PA (2007) Effects of open endotracheal suction on lung volume in infants receiving HFOV. Intensive Care Med 33:689–693
Liu J, Joynt C, Tymafichuk C, Cheung PY (2009) Sequential changes of hemodynamics and blood gases in newborn piglets with developing pneumothorax. Pediatr Pulmonol 44:70–75
Dunlop S, Hough J, Riedel T, Fraser JF, Dunster K, Schibler A (2006) Electrical impedance tomography in extremely prematurely born infants and during high frequency oscillatory ventilation analyzed in the frequency domain. Physiol Meas 27:1151–1165
Barber DC (1989) A review of image reconstruction techniques for electrical impedance tomography. Med Phys 16:162–169
Mansy HA, Royston TJ, Balk RA, Sandler RH (2002) Pneumothorax detection using pulmonary acoustic transmission measurements. Med Biol Eng Comput 40:520–525
Mansy HA, Royston TJ, Balk RA, Sandler RH (2002) Pneumothorax detection using computerised analysis of breath sounds. Med Biol Eng Comput 40:526–532
Bhatia R, Loughnan P, Derham J, Tingay DG (2009) Open lung ventilation improves and maintains regional lung volume and ventilation using both conventional and high-frequency ventilation. Pediatric Academic Societies
Litmanovitz I, Carlo WA (2008) Expectant management of pneumothorax in ventilated neonates. Pediatrics 122:e975–e979
Goldberg RN (1981) Sustained arterial blood pressure elevation associated with pneumothoraces: early detection via continuous monitoring. Pediatrics 68:775–777
Miedema M, Frerichs I, de Jongh FH, van Veenendaal MB, van Kaam AH (2010) Pneumothorax in a preterm infant monitored by electrical impedance tomography: a case report. Neonatology 99:10–13
Thome U, Topfer A, Schaller P, Pohlandt F (1998) Comparison of lung volume measurements by antero-posterior chest X-ray and the SF6 washout technique in mechanically ventilated infants. Pediatr Pulmonol 26:265–272
Gothberg S, Parker TA, Griebel J, Abman SH, Kinsella JP (2001) Lung volume recruitment in lambs during high-frequency oscillatory ventilation using respiratory inductive plethysmography. Pediatr Res 49:38–44
Lachmann B, Robertson B, Vogel J (1980) In vivo lung lavage as an experimental model of the respiratory distress syndrome. Acta Anaesthesiol Scand 24:231–236
Copnell B, Tingay DG, Kiraly NJ, Sourial M, Gordon MJ, Mills JF, Morley CJ, Dargaville PA (2007) A comparison of the effectiveness of open and closed endotracheal suction. Intensive Care Med 33:1655–1662
Tingay DG, Copnell B, Grant CA, Dargaville PA, Dunster KR, Schibler A (2010) The effect of endotracheal suction on regional tidal ventilation and end-expiratory lung volume. Intensive Care Med 36:888–896
Konno K, Mead J (1967) Measurement of the separate volume changes of rib cage and abdomen during breathing. J Appl Physiol 22:407–422
Markhorst DG, Van Gestel JP, Van Genderingen HR, Haitsma JJ, Lachmann B, Van Vught AJ (2006) Respiratory inductive plethysmography accuracy at varying PEEP levels and degrees of acute lung injury. J Med Eng Technol 30:166–175
Acknowledgments
The authors wish to thank Mr. Madgy Sourial and the staff of the RCH Animal Research Facility for assistance with animal preparation. DGT is supported by a National Health and Medical Research Council (NHMRC) Clinical Research Fellowship (grant ID 491286). PGD is supported by a NHMRC Program Grant (grant ID 606789). GMS is a past recipient of a Royal Women’s Hospital Postgraduate Scholarship and is supported in part by a Monash International Postgraduate Research Scholarship.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
134_2011_2421_MOESM2_ESM.tif
ESM Figure A: Global change in end-expiratory intra-thoracic volume (EEV) (closed diamonds) as measured by RIP, expressed as mL/kg, and global relative impedance change (open circles) as measured by EIT, expressed as countless units (c.u), at each volume instillation to create a pneumothorax. Data points represent mean ± SEM. Both RIP and EIT were able to identify a linear relationship between instillation volume and EEV; slope 0.096, r2 0.96 and slope 0.288, r2 0.96 respectively (TIF 119 kb)
Rights and permissions
About this article
Cite this article
Bhatia, R., Schmölzer, G.M., Davis, P.G. et al. Electrical impedance tomography can rapidly detect small pneumothoraces in surfactant-depleted piglets. Intensive Care Med 38, 308–315 (2012). https://doi.org/10.1007/s00134-011-2421-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2421-z