
Abstract
The causes and risk factors of symptomatic spontaneous pneumothorax in term newborns are not completely understood. In the present study, our aim was to investigate the risk factors for and clinical and laboratory characteristics of term newborns with spontaneous symptomatic pneumothorax and to evaluate the outcome of management in this condition. A total of 11 term newborns admitted to the newborn intensive care unit with a diagnosis of symptomatic spontaneous pneumothorax were included during a 22-month period. Female to male ratio was 4:7, mean gestational age was 39.5 weeks, and 63% were delivered with a cesarean section, 18% of patients had renal and 55% had congenital cardiac anomalies. Rate of cardiac anomalies was more frequent in the study group compared to control group. Echocardiography in addition to renal ultrasonography may also be needed in term newborns with spontaneous symptomatic pneumothorax and further studies may be warranted to evaluate this association.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Symptomatic spontaneous pneumothorax occurs in 0.05–1% of all term newborns [1]. Familial and autosomal dominant cases have been reported [1–3]. In children, incidence of spontaneous pneumothorax is highest during neonatal period [4]. This is most probably due to high transpulmonary pressure generated with the onset of breathing [1]. Risk factors for spontaneous pneumothorax in term newborns have not been adequately studied. Risk factors, clinical and laboratory characteristics, and the outcome of the treatment were evaluated in 11 term newborns that were diagnosed with symptomatic spontaneous pneumothorax during a 22-month period in our unit.
Materials and methods
In this prospective study, the population consisted of 11 term newborns that were diagnosed with symptomatic spontaneous pneumothorax between May 2004 and November 2005 in the Newborn Intensive Care Unit, Medical Faculty of Dicle University. Maternal age, gestational age, gender, Apgar score, route of delivery, birth weight, meconium aspiration, the need for respiratory support, age at the time of admission, lung X-ray, renal ultrasonography, echocardiography, and the outcome of the treatment were assessed. Patients were excluded if resuscitation or positive pressure ventilation was performed or if they had meconium aspiration. Lung X-rays were taken within the first 30 min of admission, and an echocardiographic examination was performed by an experienced pediatric cardiologist for cardiac anomalies, as all patients had cyanosis and respiratory difficulty. Renal ultrasonography was performed in all patients for renal anomalies before discharge. Oxygen treatment was given to maintain oxygen saturation between 90 and 96%; tube thoracostomy was applied in patients with severe respiratory difficulty. Also, mechanical ventilation or nasal CPAP (continuous positive airway pressure) treatment was given if severe respiratory difficulty and low oxygen saturation persisted. The study patients were compared with 11 control term newborn infants, randomly selected. Data were analyzed using Mann–Whitney U test for nonparametric data and a Fisherȁ9s Exact Test for parametric data. P < 0.05 was considered significant.
Results
A total of 11 consecutive patients with symptomatic spontaneous pneumothorax were included in this study from 1,799 patients who were admitted to our newborn intensive care unit during a 22-month period. There was no family history of pneumothorax in any of the cases. The incidence of symptomatic spontaneous pneumothorax in this series was 0.6%. There were more boys than girls, with a male to female ratio of 7:4. There were no statistically significant differences between the gender, maternal age, maternal gravidity, spontaneous vaginal delivery (SVD), cesarean section delivery, birth weight, and renal abnormality of the study group and control groups ( Table 1). The average Apgar score of the study group was found to be significantly low compared to the control group (P < 0.01). All patients were admitted in the first 24 h (range 10 min–24 h). Four of the patients were referred to our clinic with a diagnosis of pneumothorax. Even if one patient had a history of oligohidramnios, that patient had premature membrane rupture (22 h before delivery), and was thus included in the study. Sixty-three percent of the cases were delivered with a cesarean section (Table 2).
In all patients, respiratory symptoms (respiratory difficulty, tachypnea, and cyanosis) had started in the first 5–30 min following birth. Eight patients had oxygen saturation below 90%. X-ray examination revealed pneumothorax at the right side in eight patients and at the left side in three patients; one patient had pneumomediastinum. Two patients had Rh incompatibility, and one patient had congenital hypothyroidism. Complete blood counts, biochemical tests, and urine analysis were within normal range in all cases.
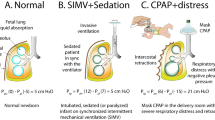
Mechanical ventilatory support was administered to two patients and nasal CPAP to two patients. Six patients received tube thoracostomy, and five received oxygen treatment only. Drainage was closed and the tube was removed after 24–48 h in patients with tube thoracostomy. Two patients who were given mechanical ventilatory support were extubated within 48 h. Normal flow oxygen treatment was started after 24 h upon stabilization of oxygen saturation in patients who received nasal CPAP. The average length of hospital stay was 7.7 days, and the mean duration of oxygen treatment was 52.8 h. One patient had Grade 4 hydronephrosis due to narrowed ureteral pelvic junction (UPJ) obstruction, and one patient had Grade 2 pelvic-caliceal ectasia. Echocardiography revealed ASD in four, ASD and pulmonary stenosis (PS, light degree, and asymptomatic) in one, and ASD and patent ductus arteriosus (PDA) in one patient. Dopamine and enalapril were given to the patient with PDA. The follow-up echocardiography after 3 days showed closure of PDA. Rate of cardiac abnormality of the study group was found to be significantly high compared to the control group (P < 0.01).
All patients were discharged with complete resolution of the signs and symptoms of symptomatic spontaneous pneumothorax. The length of follow-up ranged between 3 and 22 months, and no recurrences were observed during this period. Also, no pathology was observed in the follow-up echocardiography in patients with ASD or PDA.
Discussion
Although intubation, resuscitation, meconium aspiration, and respiratory distress syndrome frequently co-exist with spontaneous pneumothorax in newborns, it may also occur without these risk factors [5]. Pneumothorax may develop in term newborns without pulmonary pathology or positive pressure ventilation, and this is most probably due to high transpulmonary pressure generated with the onset of breathing [1]. Male gender and excessive birth weight are among the reported risk factors [6]. In our study, male gender and delivery with cesarean section seemed to increase the likelihood of spontaneous pneumothorax. No statistically significant differences were found in the male gender, birth weight, and cesarean delivery between the study and control groups (P > 0.05). However, cesarean delivery was more frequent (63%) compared to reported (17.5%) [4]. None of our patients had a history of vacuum-assisted vaginal delivery, though this is also a reported risk factor [4].
Co-existence of spontaneous pneumothorax and major congenital renal pathologies in term newborns has been reported in some studies [4, 6, 7]. Al Tawil et al. [4] found a urinary tract abnormality in 1.7% among 80 patients. In our study, 18% of patients had renal pathology, which is in line with previous reports [6]. Our literature search has revealed no studies suggesting a link between cardiac anomalies and symptomatic spontaneous pneumothorax; however, 55% of our patients had congenital cardiac problems. Though this may represent a pure coincidence, we believe that this association deserves further study.
Patients with less than 15–20% unilateral pneumothorax and no underlying pulmonary disease usually do not require treatment, as the condition usually resolves spontaneously. However, if more than 20% of the lung field on one side is affected and/or if the patientȁ9s clinical condition is deteriorating and causing respiratory insufficiency, underwater drainage is mandatory [8, 9]. Of our patients, 54.5% received underwater seal drainage and 45.5% received supportive therapy alone. In our patients, mechanical ventilation and CPAP support were received more frequently (18%) compared to reported (1.2%) [4]. This may be attributed to the low number of patients in our study.
No secondary complications due to pneumothorax developed in any of our patients. Signs and symptoms of pneumothorax completely resolved in all cases. Of the two patients with renal pathology, Grade 2 pelvic-caliceal ectasia completely resolved, while the patient with hydronephrosis is still actively followed.
In conclusion, although symptomatic spontaneous pneumothorax is a rare occurrence in term newborns, early recognition and treatment is life saving. Usual manifestation is progressive respiratory difficulty starting soon after birth.
Although our results provide further confirmation for the reported link between congenital renal anomalies and symptomatic spontaneous pneumothorax [7, 8, 10], the high incidence of cardiac abnormalities observed in our series suggests that echocardiography in addition to renal ultrasonography may also be needed in these patients and that further studies may be warranted to evaluate this association.
References
Chernick V, Avery ME (1963) Spontaneous alveolar rupture at birth. Pediatrics 32:816–824
Bagchi I, Nycyk JA (2002) Familial spontaneous pneumothorax. Arch Dis Child Fetal Neonatal Ed 86:F70
Özkiraz S, Tarcan A, Gürakan B (2004) Yenidoğanın geçici takipnesi ve ailevi spontan pnomotoraks. Türk Pediatri Arş 39:185–186
Al Tawil K, Abu-Ekteish FM, Tamimi O et al (2004) Symptomatic spontaneous pneumothorax in term newborn infants. Pediatr Pulmonol 37:443–446
Maya P, Saha SP (1983) Spontaneous pneumothorax in the newborn. Am Surg 49:192–195
Bashour BN, Balfe JW (1977) Urinary tract anomalies in neonates with spontaneous pneumothorax and/or pneumomediastinum. Pediatrics 59:1048–1049
Ashkenazi S, Merlob P, Stark H, Einstein B, Grunebaum M, Reisner SH (1983) Renal anomalies in neonates with spontaneous pneumothorax—incidence and evaluation. Int J Pediatr Nephrol 4:25–27
DeMeester TR, Lafontaine E (1990) The pleura. In: Sabiston DC, Spencer FC (eds) Surgery of the chest. WB Saunders, Philadelphia, pp 440–449
Rowe MI, Oȁ9Neill JA, Grosfeld JL, Fonkalsrud EW, Coran AG (1995) Intrathoracic access and procedures. In: Essentials of pediatric surgery. Mosby, St. Louis, pp 152–156
Orenstein DM (1996) Diseases of the pleura. In: Behrman RI, Kliegman RM, Arvin AM (eds) Nelson textbook of pediatrics. WB Saunders, Philadelphia, pp 1254–1255
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Katar, S., Devecioğlu, C., Kervancıoğlu, M. et al. Symptomatic spontaneous pneumothorax in term newborns. Pediatr Surg Int 22, 755–758 (2006). https://doi.org/10.1007/s00383-006-1740-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-006-1740-6