
Abstract
Background
A growing number of studies have suggested that the single nucleotide polymorphism (SNP) rs662 (G>A) in paraoxonase 1 (PON1) is significantly associated with susceptibility to coronary heart disease (CHD) in the Chinese population. To further evaluate the effects of the PON1 RS662 (G>A) polymorphism on the risk of CHD, we performed a meta-analysis in a Chinese population.
Methods
PubMed, Embase, Wanfang Data, Chinese National Knowledge Infrastructure (CNKI) were searched to identify eligible studies. Pooled odds ratios (ORs) and 95% confidence intervals (CIs) were used to evaluate the strength of the associations between RS662 (G>A) and CHD.
Result
In the meta-analysis, we identified 14 articles, including a total of 4835 CHD patients and 5111 controls in the Chinese population. Our result showed that overall rs662 (G>A) was significantly associated with susceptibility to CHD in the Chinese population when compared with healthy controls. Furthermore, a G allele suggested an elevated risk of CHD. In the subgroup analyses stratified by ethnicity and geographic areas, significant associations were found in Chinese Han and South China, but not in North China.
Conclusion
The present meta-analysis suggests that rs662 (G>A) SNP in PON1 is associated with CHD risk; the G allele might be the risk allele for CHD susceptibility in the Chinese population. However, more research is required to make a definite conclusion.
Zusammenfassung
Hintergrund
Immer mehr Studien liefern Belege, dass der Einzelnukleotidpolymorphismus („single nucleotide polymorphism“ [SNP]) rs662 (G>A) in der Paraoxonase 1 (PON1) signifikant mit der Anfälligkeit für die koronare Herzkrankheit (KHK) in der chinesischen Bevölkerung assoziiert ist. Zur genaueren Untersuchung der Effekte des PON1-rs662-(G>A)-Polymorphismus auf das KHK-Risiko wurde eine Metaanalyse mit chinesischen Populationen durchgeführt.
Methoden
PubMed, Embase, Wanfang Data und Chinese National Knowledge Infrastructure (CNKI) wurden nach relevanten Studien durchsucht. Mit gepoolten Odds Ratios (OR) und 95 %-Konfidenzintervallen (KI) wurde die Stärke der Assoziationen zwischen RS662 (G>A) und KHK untersucht.
Ergebnisse
In der Metaanalyse wurden 14 Beiträge mit insgesamt 4835 KHK-Patienten und 5111 Kontrollen aus der chinesischen Bevölkerung identifiziert. Die Analyse ergab im Vergleich mit gesunden Kontrollen, dass rs662 (G>A) insgesamt signifikant mit der KHK-Anfälligkeit in der chinesischen Bevölkerung assoziiert war. Darüber hinaus wies ein G‑Allel auf ein erhöhtes KHK-Risiko hin. In der Subgruppenanalyse mit Stratifizierung nach ethnischer Zugehörigkeit und geografischer Region wurden signifikante Assoziationen bei Han-Chinesen gefunden, ebenso in Südchina, nicht jedoch in Nordchina.
Schlussfolgerung
Gemäß der vorliegenden Metaanalyse ist der rs662-(G>A)-SNP in PON1 mit dem KHK-Risiko assoziiert; das G‑Allel könnte das Risikoallel für KHK-Anfälligkeit in der chinesischen Bevölkerung sein. Eine endgültige Beurteilung setzt allerdings weitere Forschungsbemühungen voraus.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A growing number of epidemiological studies indicate that coronary heart disease (CHD) has become a main cause of high morbidity and mortality worldwide [1]. With the improvement of living conditions and lifestyle in China, the incidence of CHD has continually increased over the years. In 2009, the mortality rate of CHD increased to 94.96/100,000 in the urban setting and 71.27/100,000 in rural China [2]. Researchers have shown that a variety of factors contribute to the pathogenetic process of CHD, including hyperlipidemia, hypertension, diabetes, and smoking. However, in recent years, a large number of studies have indicated that genetic factors play an important role in the pathogenesis of CHD [3]. Research on different populations and ethnicities indicated that patients whose first-degree relatives (<60 years old) with early onset CHD had a 2–10 times higher incidence of CHD compared with people who have no family history of CHD [4]. Therefore, genetic predisposition has gradually attracted attentions of researchers.
Paraoxonase 1 (PON1), located on the long arm of chromosome 7 at q21.3, plays an important role in antiatherosclerosis. Single-nucleotide polymorphism (SNP), the most common type of DNA sequence deviation, has been reported to account for approximately 90% of genetic variations in the human genome [5]. The genetic polymorphisms in the PON gene might affect the concentration and activity of PON enzyme in serum, thus, ultimately impacting enzyme function in vivo. Among all the SNPs in the PON1 gene, rs662 has been studied intensively by many researchers. The relationship between rs662 and susceptibility to CHD has been widely studied in Chinese population; however, the results have been inconsistent. Wang et al. [6] suggested that rs662 was significantly associated with susceptibility to CHD in North China; however, the study by Su et al. [7] came to the opposite conclusion. Xie et al. [8] reported that there was no significant impact of rs662 genetic variations on CHD in a southern Chinese population. Zhu et al. [9], however, indicated that CHD patients carrying rs662 were not significantly different from controls. To draw a precise conclusion on the relationship between rs662 and susceptibility to CHD, we conducted this meta-analysis.
Method
Search strategy
Two researchers respectively searched electronic search platforms, including PubMed, Embase, Wanfang Data, and Chinese National Knowledge Infrastructure (CNKI), to identify eligible studies published before July 2017. There was no restriction imposed on search language. The search terms were as follows: (1) PON, paraoxonase; (2) coronary heart disease, coronary artery disease, arteriosclerosis, myocardial infarction, ischemic heart disease, carotid atherosclerosis, atherosclerosis; (3) Chinese, China. All the terms were combined in the search.
Inclusion criteria
The following inclusion criteria were used: (1) case–control or cohort studies on the association between rs662 polymorphism and CHD; (2) providing the distribution data in patients and controls; (3) study describing a Chinese population. Exclusion criteria were (1) duplicate data, (2) incomplete rs662 distribution data, and (3) meta-analyses, letters, reviews, meeting abstracts, or editorial articles.
Data extraction
Two authors independently read the 14 studies that were included and extracted the following study characteristics: first author, year of publication, geographic area(s), ethnicity, sample size, distribution data in patients and controls.
Statistical analysis
We used pooled odds ratio (ORs) and 95% confidence intervals (CIs) to evaluate the strength of the association between the rs662 polymorphism and CHD. Heterogeneity in these studies was evaluated by χ2-based Q statistic test and I2 statistics. The fixed-effects model and random-effects model based on the Mantel–Haenszel method and the DerSimonian and Laird method were used to evaluate the sensitivity analysis. Publication bias by the method of Egger’s linear regression test was assessed by funnel plots. Stratified analyses were performed by ethnicity and geographic areas, including Han Chinese, South China, and North China. All data were analyzed with Review Manager (version 5.0.0), using two-sided P values.
Results
Description of included studies
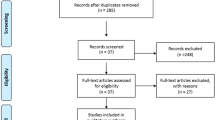
The flow diagram for the literature selection is shown in Fig. 1. After searching the electronic search platforms, a total of 233 articles that studied the association between the rs662 polymorphism and risk of CHD were identified. Based upon the exclusion criteria, 219 studies were excluded, while 14 studies met the inclusion criteria. The characteristics of the included studies were summarized in Table 1. Thus, 4835 CHD patients and 5111 controls from 14 included articles were included in the present meta-analysis to evaluate the relationship between rs662 polymorphism and susceptibility to CHD in the Chinese population.

Flow diagram of study selection
Meta-analysis for the PON1 rs662 G>A polymorphism
In order to evaluate the precise association between the rs662 polymorphism and CHD risk, we compared the healthy group to the CHD group. In the total analysis, there was a significant association between rs662 and risk of CHD for all genetic models (G vs. A, OR 1.34, 95% CI 1.13–1.58; GG vs. AA, OR 1.72, 95% CI 1.25–2.36; GG+GA vs. AA, OR 0.74, 95% CI 0.60–0.90; GA+AA vs. GG, OR 1.48, 95% CI 1.14–1.93; Fig. 2). Furthermore, Figs. 3 and 4 showed, in the stratified analysis of ethnicity and geographic areas, the same results in the Chinese Han population (G vs. A, OR 1.30, 95% CI 1.09–1.54; GG vs. AA, OR 1.20, 95% CI 1.08–1.32; GG+GA vs. AA, OR 0.77, 95% CI 0.64–0.92; GA+AA vs. GG, OR 1.46, 95% CI 1.08–1.97) and the Southern Chinese population (G vs. A, OR 1.19, 95% CI 1.09–1.30; GG vs. AA, OR 1.40, 95% CI 1.17–1.68; GG+GA vs. AA, OR 0.80, 95% CI 0.70–0.91; GA+AA vs. GG, OR 1.25, 95% CI 1.06–1.47) for all genetic models. However, as illustrated in Fig. 5, no significant association was observed between rs662 and the population of North China (G vs. A, OR 1.39, 95% CI 0.97–1.98; GG vs. AA, OR 1.82, 95% CI 0.89–3.71; GG+GA vs. AA, OR 0.73, 95% CI 0.51–1.05; GA+AA vs. GG, OR 1.60, 95% CI 0.86–2.98). In addition, both in the total and the stratified analysis, the G allele suggested a higher susceptibility to CHD.

Association of the rs662 gene polymorphism on coronary heart disease susceptibility in the Chinese population. The association were assessed under four genetic models: a G vs A model, b GG vs AA model, c GA+AA vs GG model, d GG+GA vs AA model

Association of the rs662 gene polymorphism on coronary heart disease susceptibility in Chinese Han. The association were assessed under four genetic models: a G vs A model, b GG vs AA model, c GA+AA vs GG model, d GG+GA vs AA model

Association of the rs662 gene polymorphism on coronary heart disease susceptibility in South China. South China included Guangdong, Fujian, Shanghai, Hongkong, Jiangsu province. The association were assessed under four genetic models: a G vs A model, b GG vs AA model, c GA+AA vs GG model, d GG+GA vs AA model

Association of the rs662 gene polymorphism on coronary heart disease susceptibility in North China. North China included Beijing, Liaoning, Hebei, Shandong, Xinjiang province. The association were assessed under four genetic models: a G vs A model, b GG vs AA model, c GA+AA vs GG model, d GG+GA vs AA model
Publication bias
Begg’s funnel plot and Egger’s test were used to estimate publication bias. As shown in Fig. 6, there was no significant asymmetry in the funnel plot shapes.

Funnel plots for allele contrast of the rs662 polymorphism. The association were assessed under four genetic models: a G vs A model, b GG vs AA model, c GA+AA vs GG model, d GG+GA vs AA model
Discussion
Currently, there are about 100 million cardiovascular patients in China; in addition, the mortality rate due to cardiovascular disease is significantly higher than that of cancer and other diseases. It is estimated that about 10,000 people die of cardiovascular disease every year in China [18]. A large number of researchers have suggested that the main mechanisms of CHD pathogenesis include lipid infiltration, chronic inflammation, and oxidation [19,20,21]. However, CHD is a complex disease with multiple factors that work together leading to the pathogenesis of the disease. Convincing evidence, recently, has emerged to indicate that individual susceptibility to CHD might be partially determined by genetic predisposition.
Paraoxonase 1 (PON1), a glycoprotein synthesized in the liver and secreted into the blood, might take part in the pathogenesis of arterial thrombosis and atherosclerosis [22]. There are approximately 200 single nucleotide polymorphisms (SNPs) in the human PON1 gene. Rs662 is one SNP in the PON1 gene, which has attracted much attention from researchers. Large numbers of studies have researched the relationship between rs662 and the risk of CHD. However, recent results have been inconsistent. Therefore, we performed this meta-analysis to conduct a more precise estimate.
This is the first meta-analysis to evaluate the association of rs662 with CHD in the Chinese population. There were 14 studies, including 4835 CHD patients and 5111 controls in our meta-analysis. In the total analysis, there was a significant association of rs662 with susceptibility to CHD in China. G allele carries have a higher risk of CHD. In the subgroup analysis, the same result was also observed in Chinese Han and South China, but not in North China. In addition, the HWE data in the control and CHD patients groups suggest that there is no significant genetic background differences between the participants. The reliability and stability of the meta-analysis were examined by sensitivity analysis. In all, the results of our meta-analysis provide strong evidence for the association between the rs662 polymorphism and susceptibility to CHD in the Chinese population.
Our present study has demonstrated that there is an association between the rs662 polymorphism and risk of CHD; however, there are several limitations. First, the number of cases and controls included in our study is relative small, so there is insufficient statistical power to investigate the association between the rs662 polymorphism and risk of CHD. Second, the results of our study are only applicable to China because data from Chinese patients were included. Third, the heterogeneity in the study was high, and a stratification analysis was not possible due to the limited data of the included studies.
Taken together, our study provides evidence that the single nucleotide polymorphism rs662 has a significant association with susceptibility to CHD; the G allele might be the risk allele. Furthermore, studies with a larger number of patients with an association between rs662 and CHD are required to confirm the present findings.
Abbreviations
- CHD:
-
Coronary heart disease
- CI:
-
Confidence intervals
- CNKI:
-
China National Knowledge Infrastructure
- HWE:
-
Hardy–Weinberg equilibrium
- ORs:
-
Pooled odds ratios
- PON1:
-
Paraoxonase 1
- SNP:
-
Single nucleotide polymorphism
References
Newton JN, Briggs AD, Murray CJ et al (2015) Changes in health in England, with analysis by English regions and areas of deprivation, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386:2257–2274
Hu C, Kong L, Gao R (2012) Cardiovascular disease in China. China encyclopedia press, Beijing
Brass LM, Isaacsohn JL, Merikangas KR et al (1992) A study of twins and stroke. Stroke 23:221–223
Rissanen A, Nikkila E (1984) Identification of the high risk groups in familial coronary heart disease. Atherosclerosis 53:37–46
Collins FS, Brooks LD, Chakravarti A (1998) A DNA polymorphism discovery resource for research on human genetic variation. Genome Res 12:1229–1231
Wang X, Fan Z, Huang J et al (2003) Extensive association analysis between polymorphisms of PON gene cluster with coronary heart disease in Chinese Han population. Arterioscler Thromb Vasc Biol 23(2):328–334
Su S, Chen J, Huang J et al (2005) Paraoxonase gene cluster variants associated with coronary artery disease in Chinese Han women. Chin Med J 114:1167–1174 (article in Chinese)
Xie C, Ding X, Gao J et al (2014) The effects of CES1A2 A (–816) C and CYP2C19 loss-of function polymorphisms on clopidogrel response variability among Chinese patients with coronary heart disease. Pharmacogenet Genomics 24(4):204–210
Zhu J, Gong Y, Pan M, Cui Z, Yuan J (2005) The paraoxonase 1 Gln/Arg 192 polymorphism in patients with coronary heart disease. Journal of Nantong University (Medical Sciences) 25(1):15–19 (article in Chinese)
Liu T, Zhang X, Zhang J et al (2014) Association between PON1 rs662 polymorphism and coronary artery disease. Eur J Clin Nutr 68:1029–1035
Yang Y, Xia Y, Cui D et al (2007) Study on the relationship among the codon 55, 192 gene polymorphisms of paraoxonase-1 and coronary disease as well as its severity of stenosis. J Clin Cardio 23(8):566–569 (article in Chinese)
Zhai Z, Xing X, Qin H et al (2010) A study on PON1 gene polymorphism and the association of pon1 polymorphism with coronary heart disease among chinese han population of shandong weifang district. China Prac Med 5(19):25–27 (article in Chinese)
Du J, Zhang X (2013) Polymorphism of paraoxonase gene in Xinjiang Uygurs and Hans of Cerebral ischemic stroke and Coronary Heart Disease. J Xinjiang Med Fre 33:43–48
Wang M, Lang X, Zou L et al (2011) Four genetic polymorphisms of paraoxonase gene and risk of coronary heart disease: a meta-analysis based on 88 case-control studies. Atherosclerosis 214(2):377–385
Kang YH, Lao HY, Wu H et al (2013) Association of PON1 genotype and haplotype with susceptibility to coronary artery disease and clinical outcomes in dual antiplatelet-treated Han Chinese patients. Eur J Clin Pharmacol 69:1511–1519
Kang YH, Lao HY, Wu H et al (2006) Paraoxonase 1 gene Q192R polymorphism affects stroke and myocardial infarction risk. Clin Biochem 39:191–195
Han Y, Dorajoo R, Ke T et al (2015) Interaction effects between Paraoxonase 1 variants and cigarette smoking on risk of coronary heart disease in a Singaporean Chinese population. Atherosclerosis 240:40–45
Chen W, Fan X, Gao R et al (2012) Cardiovascular disease report in China [M]. Beijing: China encyclopedia press
Mazzali G, Fantin F, Zoico E et al (2015) Heart fat infiltration in subjects with and without coronary artery disease. J Clin Endocrinol Metab 100(9):3364–3371
Meeuwsen JAL, Wesseling M, Hoefer IE et al (2017) Prognostic value of circulating inflammatory cells in patients with stable and acute coronary artery disease. Front Cardiovasc Med 4:44
Steinberg D, Witztum JL et al (2010) Oxidized low-density lipoprotein and atherosclerosis. Arterioscler Thromb Vasc Biol 30(12):2311–2316
Aviram M, Rosenblat M, Bisgaier CL et al (1998) Paraoxonase inhibits highdensity lipoprotein oxidation and preserves its functions. A possible peroxidative role for paraoxonase. J Clin Invest 101:1581–1590
Acknowledgements
We gratefully acknowledge the Yichang Key Laboratory of ischemic cardiovascular and cerebrovascular disease translational medicine foundation (2017KXN09) for generous financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Z. Deng, H. Xiang and W. Gao declare that they have no competing interests.
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Deng, Z., Xiang, H. & Gao, W. Significant association between paraoxonase 1 rs662 polymorphism and coronary heart disease. Herz 45, 347–355 (2020). https://doi.org/10.1007/s00059-018-4737-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-018-4737-8