
Abstract
Objectives
To examine the patterning of four behavior-related health risk factors (tobacco smoking, risky alcohol drinking, overweight, and physical inactivity) among job-seekers and to investigate socio-demographic and health-related predictors of patterning.
Methods
The sample of 3,684 female and 4,221 male job-seekers was proactively recruited at three job agencies in northeastern Germany in 2008/09. Participants provided data on socio-demographics, substance use, body mass index, physical activity and self-rated health. Latent class analyses (LCA) and multinomial logistic regression analyses were applied to identify health risk patterns and possible predictors of patterning, respectively.
Results
Forty-three percent of the female and 58 % of the male participants had two or more health risk factors. LCA revealed three similar patterns for women and men: Substance use (tobacco smoking, risky drinking), Non-exercising overweight (physical inactivity, overweight/obesity) and Health-conscious (non-smoking, low-risk drinking, under-/normal weight, physical activity). Age, education, marital status, life-time unemployment and self-rated health were significantly associated with patterning in both genders.
Conclusions
Our results may help to define target populations for improving health behaviors among job-seekers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Behavior-related health risk factors (HRF), i.e., tobacco smoking, risky alcohol drinking, unhealthy diet and physical inactivity, account for the vast majority of preventable causes of premature morbidity and mortality in developed countries (Lim et al. 2012). All-cause mortality risk increases with increasing number of HRF (Heroux et al. 2012; Mitchell et al. 2010). International evidence strongly supports the notion that multiple HRF occurring in distinctive patterns within a single individual are rather the rule than the exception (e.g., Fine et al. 2004; Spring et al. 2012). These patterns provide information on quantifiable co-occurrence of the four HRF. Multiple HRF have been found to be more common at younger ages, among men, lower educated or with lower socio-economic status, unemployed, single, divorced or widowed individuals as well as among those with lower self-rated health (Berrigan et al. 2003; Laaksonen et al. 2003; Poortinga 2007; Schuit et al. 2002).
For public health purposes, high-risk populations may be of special interest. One such population may be job-seekers. Several studies confirmed that unemployment is associated with poorer physical and mental health together with an elevated risk for premature mortality (Gerdtham and Johannesson 2003; McKee-Ryan et al. 2005; Paul and Moser 2009). The elevated risk of morbidity is reflected in the increased utilization of the health care system among the unemployed (Grobe and Schwartz 2003), resulting in high healthcare expenditures. Particularly men are affected by the negative consequences of unemployment to health: they are more often smokers and spend less time with sports than employed men (Grobe and Schwartz 2003). Furthermore, more unemployed women and men drink heavily and more unemployed women and men are obese than stably employed individuals (Henkel 2011; Hollederer 2011). Freyer-Adam et al. (2011) found that 52 % of job-seekers had three or more of the six HRF investigated, with men having three or more HRF significantly more often than women. Due to these findings, gender differences of health risk behavior patterns among job-seekers seem plausible and should be considered.
Previous evidence on the patterning of HRF in other populations (e.g., Chiolero et al. 2006; Laaksonen et al. 2001) mostly found quantitative gender differences, e.g., women were more likely than men to partake in a “healthy lifestyle” pattern (Conry et al. 2011). However, Laska et al. (2009) also identified qualitatively different patterns: the “health conscious” pattern (healthy diet and physical activity but unhealthy weight control) was uniquely detected in women and the “classic jocks” pattern (high physical activity but binge drinking and intoxicated sex) was uniquely detected in men.
This study aimed to examine the patterning of four key HRF (tobacco smoking, risky alcohol drinking, overweight, physical inactivity) among job-seekers. We wanted to explore whether patterns are different between female and male job-seekers. We further aimed to investigate which socio-demographic and health-related variables are associated with these patterns.
Methods
Sample
The study was based on the baseline data of the randomized controlled Trial Of Proactive Alcohol interventions among job-Seekers (TOPAS, ClinicalTrials.gov Identifier: NCT01311245). TOPAS was approved by the ethics committee of the University Medicine Greifswald.
The sample was recruited over 12 months in 2008/09 at three job agencies in Germany (Freyer-Adam et al. 2011). In 2008/09, eight percent of the German adult population was unemployed (Federal Employment Agency 2014). All job-seekers who appeared in the waiting area to talk to a job agent were asked to respond to questions on health behaviors provided by handheld computers. Exclusion criteria were: being under 18 or over 64 years of age, being cognitively/physically incapable or having insufficient language/reading skills. A total of 9,913 job-seekers were eligible for study participation, of whom 7,920 (79.9 %) participated and 7,905 provided sufficient data for the following study.
Measures
Socio-demographics
Gender, age and three further demographic variables were assessed. School education was assessed asking for common German types of school graduation. These were categorized as: <10, 10–11, and >11 years of school (including those still in school). Marital status was measured using one item with four response categories: single, married, divorced/separated, and widowed. For further analyses and due to small cell occupation, divorced/separated and widowed were summarized to one category. Having own children was assessed using a single item with yes and no as response categories.
Duration of unemployment
Duration of total life-time unemployment was assessed asking for the total number of months or years unemployed. Using 34 and 67 % tertiles, three groups were obtained: non- or short-term unemployed (0–6 months), medium-term unemployed (6–24 months), and long-term unemployed (>24 months).
HRF
Tobacco smoking was assessed using the question “Are you a tobacco smoker currently?” Three response categories differentiated between current daily smoking, current less than daily smoking, and current non-smoking. The first two categories were considered current smokers.
Risky alcohol drinking was determined using the German adaptation of the AUDIT-Consumption (AUDIT-C, Bush et al. 1998). Three items assess frequency of drinking from “never” (0) to “four or more times per week” (4), number of drinks per occasion from “one or two” (0) to “ten or more” (4), and frequency of drinking six or more drinks per occasion, from “never” (0) to “daily or almost daily” (4). The AUDIT-C sum score ranges from 0 to 12. Gender-specific cut-off values of 4 for women and 5 for men were applied to determine risky alcohol drinking (Reinert and Allen 2007). Participants beneath the cut-off values were considered low-risk drinkers, and those with AUDIT-C = 0 abstainers.
The body mass index (BMI) was used as proxy for an unhealthy diet (Fine et al. 2004). It was obtained by self-reported weight (kg) and height (cm). The obtained BMI (=kg/m2) was then categorized into four groups (WHO report obesity 1998): underweight (BMI < 18.5), normal weight (BMI 18.5–<25.0), overweight (BMI 25.0–< 30.0), and obesity (BMI ≥ 30.0). Due to small cell occupation, underweight and normal weight were further summarized to one category.
Physical activity was measured using two items. Every day physical activity was measured using the question “How many minutes per day do you spend walking or cycling, e.g., to do your (grocery) shopping, to go to school or to work?” with five response categories: <5, 5–15, 15–30, 30–45, and >45 min. Sports activity was measured using the question “Do you also do sports?” with six response categories: none, <1 h per week, 1–2 h, 2–3 h, 3–4 h, and >4 h per week. A conglomerate of both items with four categories was used: active (≥30 min of every day physical activity and ≥1 h of additional sports per week), exercising (≥1 h of sports per week, and <30 min of every day physical activity), active in daily life (≥30 min of every day physical activity, and <1 h of sports per week) and inactive (<30 min of every day physical activity and <1 h of additional sports per week).
The total number of HRF was calculated on the basis of four HRF: current tobacco smoking, risky alcohol drinking, overweight/obesity, and physical inactivity; each was coded as 1 (present) or 0 (absent), so that the total HRF score ranged from 0 to 4.
Self-rated health
Self-rated health was assessed with the question “Would you say your health in general is: excellent (1), very good (2), good (3), fair (4), poor (5)?” This item is known to be an independent predictor of mortality (Idler and Benyamini 1997).
Statistical analyses
Statistical data analyses were performed using MPlus Version 6.12 (Muthén and Muthén 1998–2010) and STATA/SE 12.0 (StataCorp. 2011). First, we computed the proportions of HRF and the mean values for female and male job-seekers. Second, we conducted a latent class analysis (LCA) to identify the patterning of the four categorized HRF within the entire sample. LCA is a model-based approach used to identify underlying unobserved (latent), mutually exclusive subgroups (classes) comprised of similar individuals based on their response patterns to a set of observed variables (Wang and Wang 2012). Because LCA provides a statistically appropriate way to identify unobservable subgroups (e.g., lifestyle patterns, risk profiles) within a population, it is increasingly applied to health issues (e.g., Agrawal et al. 2007; Lanza and Rhoades 2013; Laska et al. 2009; Reboussin et al. 2006). One of the major benefits of LCA over cluster analysis is the availability of statistical indices and tests, such as the goodness-of-fit measures, by which the most appropriate class solution for the data (in terms of number of classes and interpretable results) can be determined (Wang and Wang 2012). Third, gender was added as a covariate to predict class membership. Fourth, given a significant effect of gender in the latent multinomial logit model, we applied two separate LCAs for women and men, using the same HRF categories as for the whole sample. To decide on the most adequate number of latent classes, models with one to five classes were estimated. For each model, we used 10,000 different start value sets to avoid local solutions. The best-fitting model was determined based on size and meaningfulness of the latent classes (Nagin 2005), the sample-size adjusted Bayesian information criterion (ABIC, Sclove 1987), the bootstrap likelihood ratio test (BLRT, Mclachlan 1987), and the estimated posterior probabilities of correct class-classification (Wang and Wang 2012). ABIC balances global fit and parsimony of a model, with smaller values indicating a better model fit. BLRT p values <0.05 indicate that the k − 1 class model is rejected in favor of the k class model. Probabilities of correct class assignment of ≥0.70 indicate adequate classification (Wang and Wang 2012). We used a maximum likelihood estimator with robust standard errors to estimate the parameters. Fifth, descriptives and bivariate analyses (ANOVAs, χ 2 statistics) stratified by class membership were conducted for women and men to examine class differences regarding socio-demographic variables, self-rated health and the total number of HRF. Sixth, multinomial multivariable logistic regression analyses were calculated for women and men to identify the best socio-demographic and health-related predictors of class membership. Variables that were significant (p < 0.01) in bivariate models were included in the multivariable models, except for the total number of HRF. Relative risk ratios (RRR) and 95 % confidence intervals (95 % CI) were calculated. Cases with missing values (1.4 %) were deleted list wise.
Results
Sample
Of the 7,905 participants, 53.4 % were male, the mean age was 33.5 years (SD = 12.5), 63.1 % were single, 25.3 % married, and 11.5 % divorced/widowed. Most of the participants (57.5 %) had 10–11 years of school education, 22.5 % had less than 10 years, and 20.0 % had more than 11 years of school education. The mean duration of total life-time unemployment was 29.2 months (SD = 41.2).
The mean number of HRF was 1.4 (SD = 0.9) in women and 1.7 (SD = 1.0) in men. Of the females (males), 16.1 % (9.7 %) had none, 40.6 % (32.5 %) one, 31.1 % (38.3 %) two, 10.8 % (16.6 %) three and 1.3 % (2.9 %) four of the examined HRF. Thus, 43.2 % (57.8 %) had ≥2 HRF.
Latent class analyses
Model selection
For the entire sample, the ABIC suggested three classes, whereas the BLRT p values indicated four (Table 1). Moreover, only the two- and three-class models showed adequate probabilities of correct class-classification. By further considering meaningfulness of the latent classes, the three-class model was preferred and selected for further analyses as it produced a solution with a logical meaningful interpretation. Thus, we included gender as a covariate in the three-class model to predict class membership. It revealed a significant positive effect of gender in the multinomial model, i.e., women were more likely to be classified in class two rather than in class three and in class one (p < 0.001). Therefore, we estimated two gender-specific LCA models.
For both genders, both the ABIC and the BLRT p values suggested that the three-class model was preferable (Table 1). Only the two-class models showed adequate probabilities of correct class-classification. However, by further considering meaningfulness of the latent classes, the three-class model was preferred and selected for further analyses for both women and men. It produced a solution with a logical meaningful interpretation.
Characterization of the latent classes
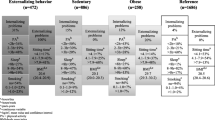
Job-seekers in the first latent class, representing 48.1 % of the entire sample, had a 1.00 probability of reporting tobacco smoking (Table 2). In comparison to the other classes, they also had the highest probabilities of reporting risky drinking (0.37) and under-/normal weight (0.66). This class was labeled Substance use. The same pattern emerged within the gender-specific models; it corresponded to class 2 in the female (representing 50.6 % women) and to class 3 in the male (representing 44.0 % men) model. Those in the second latent class, comprising 34.0 % of the sample, were most likely to report obesity (0.26) compared to the other classes. Moreover, they were extremely unlikely to report that they were physically active (0.03) and exercising (0.00). This class was labeled Non-exercising overweight. The same pattern emerged within the gender-specific models, corresponding to class 1 in both models (representing 19.9/34.1 % women/men). The third latent class comprised 17.9 % of the job-seekers and yielded the most favorable distribution of all four HRF, relative to the other classes. These individuals were likely to report non-smoking (0.78), low-risk drinking (0.67), under-/normal weight (0.55), physical activity (0.57) and exercise (0.36). This class was labeled Health-conscious. The same pattern emerged within the gender-specific models; it corresponded to class 3 in the female (representing 29.6 % women) and class 2 in the male (representing 21.8 % men) model.
Further description of classes
Age, education, marital status, life-time unemployment and self-rated health were significant predictors of class membership in the female and male multinomial logistic regression models (Tables 3, 4).
In both genders, a younger age was positively associated with the Substance use while it was negatively associated with the Non-exercising overweight class membership. Higher school education was negatively associated with the Substance use and the Non-exercising overweight class membership. Being single and being divorced/widowed were positively associated with belonging to the Substance users, while it was negatively associated with belonging to the Non-exercising overweight. Long-term unemployment was positively associated with both the Substance use and the Non-exercising overweight class membership. The Non-exercising overweight and the Substance users rated their health inferior to the Health-conscious class and the Substance users rated their health superior to the Non-exercising overweight.
Only in women, having children was positively associated with belonging to the Substance users. Only in men, medium-term unemployment was positively associated with both belonging to the Substance users and to the Non-exercising overweight.
Discussion
Our findings suggest a considerable patterning of HRF among job-seekers with more similarities than differences between women and men. Three distinct patterns were identified for both genders and these patterns were qualitatively almost identical: a Substance use pattern with smoking and risky drinking as key characteristics; an unhealthy diet and inactive pattern with overweight/obesity and lack of physical activity/exercise as key characteristics; and a Health-conscious pattern with the most preferable distribution of all four HRF. The co-existence of two distinct unhealthy patterns, namely addictive behaviors (smoking and risky drinking) and health promoting behaviors (unhealthy diet and physical inactivity), has been reported previously (de Vries et al. 2008). De Vries et al. (2008, p. 206) argued that the former “require restraining, refraining or abstinence,” whereas the latter “require actively engaging in health promoting activities,” and that differently tailored intervention strategies may be needed.
Looking at quantitative differences, the proportions of the three patterns differed slightly between both genders: the healthiest pattern was the second largest class in women but the smallest class in men. This is in accordance with previous findings stating that women were more likely to adopt a healthier lifestyle pattern (e.g., Conry et al. 2011). However, the Substance use pattern was by far the largest class in both women and men, indicating that combined tobacco smoking and risky drinking might be the most common health threat to job-seekers, irrespective of gender. By further comparing the predictors of patterning by gender, the similarities were remarkably large. For instance, lower education, long-term unemployment and poorer self-rated health were positively associated with belonging to the two “unhealthy” classes in both genders, confirming previous findings (e.g., Schuit et al. 2002).
Strengths and limitations
This study is among the first to examine the patterning of the four major HRF among the high-risk group of job-seekers—a typically hard to reach group of the general population (Bender et al. 2012). Our proactively recruited sample had a high screening adherence. We used categorized variables with at least three categories if possible to identify health-related patterns. Previous studies on the patterning of HRF almost exclusively used dichotomized risk variables to enhance interpretability (Laska et al. 2009), but this simplification approach may have been accompanied by substantial loss of information (Laaksonen et al. 2002; for an overview of problems associated with dichotomization, see MacCallum et al. 2002).
Three limitations of our study should be considered. First, we used cross-sectional data only. Second, our findings refer to one region of Germany only. Third, all four HRF were assessed by self-report only and may be biased. Generally, it can be stated that there are more objective measures available for the assessment of all four HRF, e.g., the accelerometry assessment for physical activity. However, by pursuing a proactive screening approach, we depended on quick measures. If target populations for brief health behavior change interventions are to be reached, self-statements remain indispensable.
Conclusions
Our findings indicate that job-seekers perform the same HRF patterns as previously found in other populations. As individuals who engage in specific HRF patterns may respond to interventions differently, it might be useful to provide combined interventions for tobacco smoking and risky drinking, as well as for unhealthy diet and physical inactivity. Furthermore, gender does not seem to make relevant difference in HRF patterning.
References
Agrawal A, Lynskey MT, Madden PA, Bucholz KK, Heath AC (2007) A latent class analysis of illicit drug abuse/dependence: results from the National Epidemiological Survey on alcohol and related conditions. Addiction 102(1):94–104. doi:10.1111/j.1360-0443.2006.01630.x
Bender AM, Jorgensen T, Helbech B, Linneberg A, Pisinger C (2012) Socioeconomic position and participation in baseline and follow-up visits: the Inter99 study. Eur J Prev Cardiol 21(7):899–905. doi:10.1177/2047487312472076
Berrigan D, Dodd K, Troiano RP, Krebs-Smith SM, Barbash RB (2003) Patterns of health behavior in U.S. adults. Prev Med 36(5):615–623 (S0091743502000671 [pii])
Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA (1998) The AUDIT alcohol consumption questions (AUDIT-C): an effective brief screening test for problem drinking. Ambulatory care quality improvement project (ACQUIP). Alcohol use disorders identification test. Arch Int Med 158(16):1789–1795
Chiolero A, Wietlisbach V, Ruffieux C, Paccaud F, Cornuz J (2006) Clustering of risk behaviors with cigarette consumption: a population-based survey. Prev Med 42(5):348–353. doi:10.1016/j.ypmed.2006.01.011
Conry MC et al (2011) The clustering of health behaviours in Ireland and their relationship with mental health, self-rated health and quality of life. BMC Public Health 11:692. doi:10.1186/1471-2458-11-692
de Vries H et al (2008) Clusters of lifestyle behaviors: results from the Dutch SMILE study. Prev Med 46(3):203–208. doi:10.1016/j.ypmed.2007.08.005
Federal Employment Agency (2014) Statistisches Bundesamt. In. https://www-genesis.destatis.de/genesis/online/data;jsessionid=F0EF7A90B263BE0929E613E8709F8C96.tomcat_GO_1_1
Fine LJ, Philogene GS, Gramling R, Coups EJ, Sinha S (2004) Prevalence of multiple chronic disease risk factors. 2001 national health interview survey. Am J Prev Med 27(2 Suppl):18–24. doi:10.1016/j.amepre.2004.04.0
Freyer-Adam J, Gaertner B, Tobschall S, John U (2011) Health risk factors and self-rated health among job-seekers. BMC Public Health 11:659. doi:10.1186/1471-2458-11-659
Gerdtham UG, Johannesson M (2003) A note on the effect of unemployment on mortality. J Health Econ 22(3):505–518. doi:10.1016/S0167-6296(03)00004-3
Grobe TG, Schwartz FW (2003) Federal health monitoring issue 13. Unemployment and health. Robert Koch-Institute, Berlin
Henkel D (2011) Unemployment and substance use: a review of the literature (1990–2010). Curr Drug Abuse Rev 4(1):4–27 (BSP/CDAR/E-Pub/00026 [pii])
Heroux M, Janssen I, Lee DC, Sui X, Hebert JR, Blair SN (2012) Clustering of unhealthy behaviors in the aerobics center longitudinal study. Prev Sci 13(2):183–195. doi:10.1007/s11121-011-0255-0
Hollederer A (2011) Unemployment and health in the German population: results from a 2005 microcensus. J Public Health 19:257–268
Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 38(1):21–37
Laaksonen M, Prattala R, Karisto A (2001) Patterns of unhealthy behaviour in Finland. Eur J Public Health 11(3):294–300
Laaksonen M, Luoto R, Helakorpi S, Uutela A (2002) Associations between health-related behaviors: a 7-year follow-up of adults. Prev Med 34(2):162–170. doi:10.1006/pmed.2001.0965
Laaksonen M, Prattala R, Lahelma E (2003) Sociodemographic determinants of multiple unhealthy behaviours. Scand J Public Health 31(1):37–43 (H7V3U63D37W9TTQT [pii])
Lanza ST, Rhoades BL (2013) Latent class analysis: an alternative perspective on subgroup analysis in prevention and treatment. Prev Sci Off J Soc Prev Res 14(2):157–168. doi:10.1007/s11121-011-0201-1
Laska MN, Pasch KE, Lust K, Story M, Ehlinger E (2009) Latent class analysis of lifestyle characteristics and health risk behaviors among college youth. Prevention science : the official journal of the Society for Prevention Research 10(4):376–386. doi:10.1007/s11121-009-0140-2
Lim SS et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet 380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8
MacCallum RC, Zhang S, Preacher KJ, Rucker DD (2002) On the practice of dichotomization of quantitative variables. Psychol Methods 7(1):19–40
McKee-Ryan F, Song Z, Wanberg CR, Kinicki AJ (2005) Psychological and physical well-being during unemployment: a meta-analytic study. J Appl Psychol 90(1):53–76. doi:10.1037/0021-9010.90.1.53
Mclachlan GJ (1987) On Bootstrapping the likelihood ratio test statistic for the number of Components in a normal mixture. Appl Stat-J Royal Stat Soc C 36(3):318–324. doi:10.2307/2347790
Mitchell JA et al (2010) The impact of combined health factors on cardiovascular disease mortality. Am Heart J 160(1):102–108. doi:10.1016/j.ahj.2010.05.001
Muthén LK, Muthén BO (1998–2010) Mplus User’s Guide, 6th Edn. Muthén & Muthén, Los Angeles
Nagin DS (2005) Group-based modeling of development. Havard University Press, Cambridge
Paul KI, Moser K (2009) Unemployment impairs mental health: meta-analyses. J Vocat Behav 74(3):264–282. doi:10.1016/j.jvb.2009.01.001
Poortinga W (2007) The prevalence and clustering of four major lifestyle risk factors in an English adult population. Prev Med 44(2):124–128. doi:10.1016/j.ypmed.2006.10.006
Reboussin BA, Song EY, Shrestha A, Lohman KK, Wolfson M (2006) A latent class analysis of underage problem drinking: evidence from a community sample of 16–20 year olds. Drug Alcohol Depend 83(3):199–209. doi:10.1016/j.drugalcdep.2005.11.013
Reinert DF, Allen JP (2007) The alcohol use disorders identification test: an update of research findings. Alcohol Clin Exp Res 31(2):185–199. doi:10.1111/j.1530-0277.2006.00295.x
Schuit AJ, van Loon AJ, Tijhuis M, Ocke M (2002) Clustering of lifestyle risk factors in a general adult population. Prev Med 35(3):219–224
Sclove SL (1987) Application of model-selection criteria to some problems in multivariate-analysis. Psychometrika 52(3):333–343. doi:10.1007/Bf02294360
Spring B, Moller AC, Coons MJ (2012) Multiple health behaviours: overview and implications. J Public Health (Oxf) 34(Suppl 1):i3–i10. doi:10.1093/pubmed/fdr111
StataCorp (2011) Stata statistical software: release 12. College Station, TX: Stata Corp LP
Wang J, Wang X (2012) Structural equation modeling: applications using Mplus. Wiley, West Sussex
WHO report obesity (1998) Preventing and managing the global epidemic. WHO, Genf
Acknowledgments
The conduction of the research project was funded by the German Research Foundation (grant number FR2661/1-1, FR2661/1-2). Work on this paper was also supported by the German Cancer Aid (110676, 110543), the German Centre for Cardiovascular Research (DZHK), and the program “Young scientists create new sex/gender-sensitive knowledge” within the project Epi goes Gender (01FP1229/30).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Schnuerer, I., Baumann, S., Haberecht, K. et al. Patterns of health risk behaviors among job-seekers: a latent class analysis. Int J Public Health 60, 111–119 (2015). https://doi.org/10.1007/s00038-014-0623-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-014-0623-1