
Abstract
Background
Several inflammation-based prognostic scores have a prognostic value in patients with various cancers. This study investigated the prognostic value of various inflammation-based prognostic scores in patients who underwent a surgery for adenocarcinoma of the esophagogastric junction (AEG) and upper gastric cancer (UGC).
Methods
We reviewed data of 206 patients who underwent surgery for AEG and UGC. We calculated neutrophil–lymphocyte ratio (NLR), platelet–lymphocyte ratio (PLR), Glasgow Prognostic Score (GPS), modified GPS (mGPS), C-reactive protein (CRP)/albumin (Alb) ratio, prognostic index (PI), and prognostic nutritional index (PNI) and analyzed the relationship between these biomarkers and postoperative prognosis.
Results
In multivariate analyses for overall survival, mGPS (P = 0.0337, hazard ratio [HR] = 5.211), PI (P = 0.0002, HR = 21.20), and PNI (P < 0.0001, HR = 6.907) were identified as independent predictive factors. A multivariate analysis for recurrence-free survival showed that only PI (P = 0.0006, HR = 11.89) and PNI (P = 0.0002, HR = 4.972) were independent predictive factors among the above-mentioned inflammation-based prognostic scores.
Conclusions
In various inflammation-based prognostic scores, PI and PNI were more strongly associated with poor prognosis in patients who underwent surgery for AEG and UGC.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Morbidity and mortality rates of cancers are increasing globally. Gastric cancer is the fifth most common malignant disease and the third leading cause of cancer-related deaths in the world.1 The treatment options for gastric cancer usually consist of surgical therapy, chemotherapy, and radiation therapy as the main axis, and the choice of treatment depends on the degree of tumor progression and the general condition of each patient. TNM classification is one of the indicators used for staging gastric cancers by assessing the depth of tumor, extent of lymph node metastasis, and distant metastasis.2 The TNM classification is globally used as the most reliable prognostic indicator to predict the prognosis and to determine the treatment strategy for gastric cancer.2 However, even with the same TNM stage, the prognosis of each patient with gastric cancer is different, suggesting the influence of other factors on the prognosis. There are increasing data that factors, such as malnutrition, skeletal muscle loss, and systemic inflammatory response, are associated with poor outcomes in patients with various types of cancers.3,4,5,6,7,8,9,–10
Several common inflammation-based prognostic scores, including neutrophil–lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), Glasgow Prognostic Score (GPS), modified GPS (mGPS), C-reactive protein (CRP)/albumin (Alb) ratio, prognostic index (PI), and prognostic nutritional index (PNI), have been reported to have a prognostic value in different cases of malignant, solid tumors.3,11,12,13,14,15,16,17,18,19,20,21,–22 These biomarkers can be evaluated easily by collecting blood from a peripheral vein and have great advantages, such as simplicity, minimal invasiveness, and low cost. However, it is still unclear as to which of these biomarkers is the most reliable prognostic predictor for cancer. Also, optimal cutoff values are not defined for each biomarker, and the most reliable biomarkers and cutoff values may be different according to the type of cancer.
We previously investigated the prognostic values of several inflammation-based prognostic scores, including NLR, PLR, GPS, and CRP/Alb ratio, in patients who underwent surgery for adenocarcinoma of the esophagogastric junction (AEG) and upper gastric cancer (UGC) and reported that the CRP/Alb ratio was an independent prognostic factor for overall survival (OS) 22 In the present study, we added three inflammation-based prognostic scores (mGPS, PI, and PNI) for the analyses and compared the prognostic values of these biomarkers in patients with AEG and UGC. In addition, we increased the number of patients by adding eligible cases from National Kyushu Medical Center. As a result, PI and PNI were strongly associated with the poor prognosis of AEG, and UGC and were independent prognostic factors for OS and recurrence-free survival (RFS).
Methods
Patients
In this two-institute retrospective analysis, we reviewed the data of 157 patients with AEG or UGC who underwent surgical resection at the Department of Surgery and Science, Kyushu University, from January 2005 to March 2016, and 69 patients with AEG or UGC who underwent surgical resection at Department of Gastroenterological Surgery, National Kyushu Medical Center, from January 2010 to March 2019. All 226 patients were pathologically determined to have adenocarcinoma, and patients with squamous cell carcinoma or other tumors were excluded from this study.
Among the 226 patients, 13 who underwent palliative or noncurative surgery were excluded. In addition, seven patients who underwent neoadjuvant chemotherapy were excluded, leaving 206 patients with AEG and UGC eligible for analysis. We adopted the Siewert classification regarding tumor location.23 We defined Siewert type I, II, and III tumors as AEG, and tumors in which the center was located > 5 cm below the esophagogastric junction in the upper third of the stomach as UGC.10 According to this classification, 96 and 110 patients were categorized as having AEG and UGC, respectively.
Permission to perform this retrospective cohort study was provided by the Institutional Review Board of Kyushu University (2019-395) and National Kyushu Medical Center (19C066).
Inflammation-Based Prognostic Scores
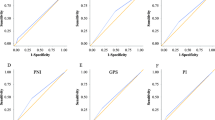
The NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI were calculated. The baseline blood data were obtained by collecting blood from the peripheral vein of each patient before surgery. The NLR and PLR were defined as absolute neutrophil count and platelet count, respectively, divided by the absolute lymphocyte count.13,18,21 The GPS and mGPS were calculated by CRP and albumin using standard thresholds (> 1.0 mg/dl for CRP and < 3.5 g/dl for albumin)16 The CRP/Alb ratio was defined as the serum CRP level divided by the serum albumin level.22 Calculation of the PI was based on the CRP level and the white blood cell count. The upper limits of reference ranges for the CRP level (0.1 mg/dL) and the white blood cell count (11,000/mm3) were used as cutoff values.11 The PI was zero if both values were < the cutoff values, and the PI was one if one of the two markers was elevated. The PNI was calculated using the following formula: 10 × serum albumin (g/dL) + 0.005 × total lymphocyte count (per mm3)19 Receiver operating characteristic (ROC) curve analysis was used to identify the optimal cutoff values of these inflammation-based prognostic scores (Supplementary Fig. 1). Time-dependent ROC curve analysis also was performed to identify prognostic factors associated with poor outcomes of AEG and UGC among various inflammation-based prognostic scores (Supplementary Fig. 2).
Statistical Analysis
Differences in characteristics between the groups were evaluated using Fisher’s exact test or unpaired t test. Survival curves were plotted according to Kaplan–Meier method, and any differences were analyzed using log-rank test. Univariate and multivariate analyses were performed with a Cox proportional hazard model to clarify the independent prognostic factors. All P values were two-sided, and a P < 0.05 was considered statistically significant. ROC curve analysis was used to determine the predictive value of the inflammation-based prognostic scores. All analyses were performed with JMP PRO 13 software (SAS Institute Inc., https://www.jmp.com/ja_jp/home.html).
Results
Characteristics of Patients and Overall Survival according to Inflammation-based Prognostic Scores
The clinicopathological characteristics of 206 patients (151 [73.3%] male, 55 [26.7%] female) and their association with overall survival (OS) are summarized in Table 1. The median patient age was 66 (range, 35–92) years. Based on the tumor location, 96 and 110 patients were categorized as having AEG and UGC, respectively. Among the 206 patients, 161 (78.2%) patients underwent total gastrectomy and remaining 45 (21.8%) underwent proximal gastrectomy. D1 + lymphadenectomy was performed for tumors clinically diagnosed as T1, while D2 lymphadenectomy was performed for tumors clinically diagnosed as T2-4 tumors. The NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI were calculated based on laboratory data obtained by sampling peripheral blood. ROC curve analysis was performed to identify the optimal cutoff values of these inflammation-based prognostic scores related to the overall survival of patients with AEG and UGC. The optimal cutoff values of the NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI were identified as 2.20, 170, 1, 1, 0.017, 1, and 44.7; the area under the curve (AUC) values were 0.60213, 0.52591, 0.60714, 0.58587, 0.65948, 0.57390, and 0.67218, respectively. The AUC of the CRP/Alb ratio and PNI tended to be higher than that of the other biomarkers (Supplementary Table 1; Supplementary Fig. 1). The patients were divided into two groups according to the cutoff values of inflammation-based prognostic scores, and the number of patients in each group is summarized in Table 1. Time-dependent ROC curve analyses for OS and RFS were performed, and each AUC value of PNI was the highest among inflammation-based prognostic scores (0.7436 [OS] and 0.6756 [RFS], respectively) (Supplementary Table 2; Supplementary Fig. 2).
Factors associated with Poor Prognosis of AEG and UGC
To identify independent prognostic factors for OS, univariate and multivariate analyses with a Cox proportional hazard model was done. The univariate analyses revealed that age ≥ 65 years (vs. < 65 years; P = 0.0030), T-stage (T3-4 vs. T1-2; P < 0.0001), N-stage (N1-3 vs. N0; P < 0.0001), postoperative complication (yes vs. no; P = 0.0386), NLR ≥ 2.20 (vs. < 2.20; P = 0.0001), PLR ≥ 170 (vs. < 170; P = 0.0129), GPS ≥ 1 (vs. < 1; P = 0.0003), mGPS ≥ 1 (vs. < 1; P = 0.0006), CRP/Alb ≥ 0.017 (vs. < 0.017; P = 0.0046), PI = 1 (vs. 0; P < 0.0001), and PNI < 44.7 (vs. ≥ 44.7; P < 0.0001) were associated with OS in patients with AEG and UGC (Supplementary Table 3). In the multivariate analyses, GPS, mGPS, and CRP/Alb ratio were analyzed individually because of their strong associations with each other; these scores are dependent on values of serum albumin and CRP in common. GPS (P = 0.0125, hazard ratio [HR] = 4.373), mGPS (P = 0.0337, HR = 5.211), PI (P < 0.0001, HR = 13.58), and PNI (P < 0.0001, HR = 8.946) were independent predictive factors of OS in patients with AEG and UGC among the above-mentioned, inflammation-based, prognostic scores (Table 2). We also performed univariate and multivariate analyses on RFS. In the univariate analysis, the same factors used in the OS analysis, except for age ≥ 65 years, were extracted (Supplementary Table 4). The multivariate analysis for RFS showed that only GPS (P = 0.0150, HR = 3.774), PI (P < 0.0001, HR = 10.33), and PNI (P < 0.0001, HR = 6.416) were independent predictive factors among the above-mentioned inflammation-based prognostic scores (Table 3).
Postoperative Prognosis Based on PI and PNI
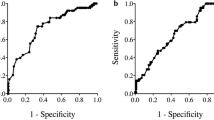
The results of multivariate analyses in this study suggest that PI and PNI may be strongly correlated with the poor prognosis of AEG and UGC among the above inflammation-based prognostic scores. Therefore, patients were divided into two groups according to the cutoff values of these two scores, and the Kaplan–Meier method was performed for comparison of 5-year RFS and OS. This revealed that poorer 5-year RFS and OS rates in patients with AEG and UGC were associated with both PI = 1 (vs. PI = 0) (RFS: 23.5% vs. 76.9%, HR = 7.048, P < 0.0001; OS: 22.8% vs. 79.7%, HR = 7.605, P < 0.0001) and PNI < 44.7 (vs ≥ 44.7) (RFS: 42.0% vs. 80.7%, HR = 4.058, P < 0.0001; OS: 41.7% vs. 84.5%, HR = 5.460, P < 0.0001; Figs. 1 and 2).

Postoperative survival in patients with AEG and UGC based on prognostic index (PI): (a) recurrence-free survival and (b) overall survival of all studied patients. Patients were categorized according to PI (PI = 0 or PI = 1). The 5-year recurrence-free and overall survival rates were significantly lower in patients with PI = 1 than those in patients with PI = 0 (RFS: P < 0.0001, HR = 7.048; OS: P < 0.0001, HR = 7.605). AEG adenocarcinoma of esophagogastric junction; UGC upper gastric cancer; PI prognostic index; HR hazard ratio

Postoperative survival in patients with AEG and UGC based on prognostic nutritional index (PNI): (a) recurrence-free survival and (b) overall survival of all studied patients. The optimal cutoff value of PNI was determined to be 44.7. The 5-year recurrence-free and overall survival rates were significantly lower in patients with PNI < 44.7 than in those with PNI ≥ 44.7 (RFS: P < 0.0001, HR = 4.058; OS: P < 0.0001, HR = 5.460). AEG adenocarcinoma of esophagogastric junction; UGC upper gastric cancer; PNI prognostic nutritional index; HR hazard ratio
Subgroup analyses also were performed. First, the same analyses were performed with the subjects limited to patients diagnosed with Stage II or III disease as tumor progression might affect general condition and nutritional status. ROC curve analysis was performed again to identify the optimal cutoff values of PI and PNI in patients with only Stage II and III. As a result, the optimal cutoff values of the PI and PNI were identified as 1 and 44.7, which were the same values as those of all patients; the AUC values were 0.58842 and 0.65172, respectively. Both PI = 1 (vs. PI = 0) and PNI < 44.7 (vs. ≥ 44.7) were significantly associated with poor prognosis in patients with Stage II and III disease (Fig. 3).

Postoperative survival in patients diagnosed with Stage II and III AEG and UGC based on prognostic index (PI) ((a) recurrence-free survival and (b) overall survival) or prognostic nutritional index (PNI) ((c) recurrence-free survival and (d) overall survival). Kaplan–Meier analyses were performed according to the same criteria as in Figs. 1 and 2. AEG adenocarcinoma of esophagogastric junction; UGC upper gastric cancer; PI prognostic index; PNI prognostic nutritional index
Next, patients were categorized according to tumor location as biological properties differed between AEG and UGC. The Kaplan–Meier method performed separately according to location showed that both PI = 1 (vs. PI = 0) and PNI < 44.7 (vs. ≥ 44.7) were significantly associated with poor prognosis, regardless of tumor location (Supplementary Figs. 3 and 5). Especially in AEG patients, the prognosis of the PI = 1 group was extremely poor (5-year RFS and OS: 0.0%; Supplementary Fig. 3). We also categorized patients according to Siewert classification and performed the Kaplan–Meier method separately by Siewert types I, II, and III. Because of subdivision of patients, the analyses for Siewert types I and III groups were a small sample size especially, but a similar tendency was observed in each group (Supplementary Figs. 4 and 6).
Discussion
In this study, the prognostic value of the common inflammation-based prognostic scores, including NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI, in patients who underwent surgery for AEG and UGC was compared. We found that GPS, PI, and PNI were more strongly associated with the poor prognosis of AEG and UGC than the other biomarkers and that they were independent prognostic factors for OS and RFS in patients who underwent surgical treatment of AEG and UGC.
The above-mentioned biomarkers have been reported to have prognostic value in patients with various types of cancers, including gastrointestinal tumors, such as esophageal cancer, gastric cancer, and colorectal cancer.3,11−22 However, few studies about the relationship among these biomarkers with respect to prognosis in patients with AEG have been published. In patients with AEG, pre-albumin, BMI, NLR, and CRP/Alb ratio were reported as independent prognostic factors.22,24,25 On the other hand, to the best of our knowledge, no studies compare the relationship among various inflammation-based prognostic scores and prognosis in patients with AEG who underwent surgery.
A few studies have compared the validity of several inflammation-based prognostic scores to predict the prognosis of gastrointestinal malignancies. Toyokawa et al. evaluated the prognostic value of CRP/Alb ratio, NLR, PLR, PNI, GPS, and PI in patients with stage II gastric cancer.26 They concluded that CRP/Alb ratio and PNI were independent prognostic factors and superior to the other biomarkers.26 Wen et al. also compared various inflammation-based prognostic scores, such as mGPS, NLR, PLR, PI, and PNI, in patients with esophageal and gastric carcinoma and concluded that only PLR and PNI were the significant predictors of patient survival.27 They also performed a subgroup analysis and indicated that mGPS was predictive of patient survival only in esophagectomies.27 In our analysis, seven prognostic scores were compared, and GPS, PI, and PNI were identified as the independent prognostic factors for both OS and RFS in patients with AEG and UGC. Although there were differences in cancer type and cutoff values for prognostic scores among these studies, all of them suggest that PNI is a significant predictive biomarker common to above studies. Therefore, PNI may be the most reliable biomarker to predict the prognosis of gastrointestinal tumors among inflammation-based prognostic scores.
The value of PNI is determined by serum albumin and total lymphocyte count. Serum albumin is used as an indicator of nutritional status, and it has been reported that hypoalbuminaemia is associated with cancer progression and poor survival outcomes in various types of cancers.28,29,30,31,32,–33 Possible mechanisms are as follows: first, chronic inflammation exhausts nutrition and energy in cancer patients, and hypoalbuminemia may occur because of the systemic inflammatory response; and second, hypoalbuminemia reflects malnutrition or cachexia, which is associated with poor outcomes.27 Moreover, decrease in the number of lymphocytes can be a factor that deteriorates the value of PNI. Ray-Coquard et al. found that lymphopenia was an independent prognostic factor for overall survival in advanced carcinomas, sarcomas, and lymphomas.34 Precise mechanisms of the relationship between lymphopenia and poor prognosis remains unclear. The possible mechanisms are as follows: first, lymphopenia reflects the presence of immunosuppression, which promotes cancer progression. This condition suggests that the host tends to have an inadequate immunological reaction. Second, the low lymphocyte count may be a consequence of lympholytic cytokines produced by lymphoma cells, and such a lymphoma may itself be resistant; and third, a combination of both or other factors.34 The mechanisms of lymphopenia in cancer patients may be multifactorial.
As described above, inflammation-based prognostic scores represented by PNI may reflect patient nutritional and immune status. Nutrition disorders result in skeletal muscle loss. Recent studies have shown that some myokines secreted by muscle cells can regulate cancer cell growth. Aoi et al. reported that a novel myokine, secreted protein acidic and rich in cysteine (SPARC), suppressed colon tumor growth via exercise by increasing apoptosis.35 Hojman et al. have reported that exercise-induced, muscle-derived cytokines inhibit mammary cancer cell growth.36 These results suggest that nutritional support and increased muscle mass may contribute to tumorigenesis prevention via myokine secretion. Therefore, enhanced perioperative nutritional support and physical exercises may improve long-term outcomes after surgery, especially in AEG and UGC patients with poor inflammation-based prognostic scores.
A limitation of our previous study was that it had a small sample size and was a single-institution retrospective study. Therefore, we increased the number of patients by adding eligible cases from National Kyushu Medical Center in this study. Although these results may not be generalizable to other patient cohorts, few studies have focused on the relationships between patients with AEG or UGC and inflammation-based prognostic scores. Accumulation of the findings obtained from retrospective studies from various institutes would be meaningful. The findings from the current study offer useful information regarding the clinical value of GPS, PI, and PNI.
Conclusions
The GPS, mGPS, PI, and PNI were strongly associated with a poor prognosis in patients who underwent surgery for AEG and UGC. These predictive scores for the prognosis of AEG and UGC were superior to the other inflammation-based prognostic scores. PNI tended to be the most relevant score for the prognosis of gastrointestinal tumors, which is consistent with that reported in previous studies. These biomarkers may be useful for evaluating high-risk patients with AEG and UGC easily and noninvasively.
References
Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108.
Lu J, Zheng CH, Cao LL, et al. The effectiveness of the 8th American joint committee on cancer TNM classification in the prognosis evaluation of gastric cancer patients: a comparative study between the 7th and 8th editions. Eur J Surg Oncol. 2017;43(12):2349–56.
Jomrich G, Hollenstein M, John M, et al. The modified Glasgow prognostic score is an independent prognostic indicator in neoadjuvantly treated adenocarcinoma of the esophagogastric junction. Oncotarget. 2018;9(6):6968–76.
Park JH, Watt DG, Roxburgh CS, et al. Colorectal cancer, systemic inflammation, and outcome: Staging the tumor and staging the host. Ann Surg. 2016;263:326–36.
Roxburgh CS, McMillan DC. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010;6:149–63.
Kudou K, Saeki H, Nakashima Y, et al. Postoperative skeletal muscle loss predicts poor prognosis of adenocarcinoma of upper stomach and esophagogastric junction. World J Surg. 2018; https://doi.org/10.1007/s00268-018-4873-6.
Tamandl D, Paireder M, Asari R, et al. Markers of sarcopenia quantified by computed tomography predict adverse long-term outcome in patients with resected oesophageal or gastro-oesophageal junction cancer. Eur Radiol. 2016;26:1359–67.
Vayrynen JP, Tuomisto A, Klintrup K, et al. Detailed analysis of inflammatory cell infiltration in colorectal cancer. Br J Cancer. 2013;109:1839–47.
Miyamoto Y, Baba Y, Sakamoto Y, et al. Sarcopenia is a negative prognostic factor after curative resection of colorectal cancer. Ann Surg Oncol. 2015;22:2663–8.
Kudou K, Saeki H, Nakashima Y, et al. Prognostic significance of sarcopenia in patients with esophagogastric junction cancer or upper gastric cancer. Ann Surg Oncol. 2017;24(7):1804–10.
Kinoshita A, Onoda H, Imai N, et al. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br J Cancer. 2012;107(6):988–93.
Ignacio de Ulibarri J, Gonzalez-Madrono A, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 2005;20:38–45.
Yamanaka T, Matsumoto S, Teramukai S, et al. The baseline ratio of neutrophils to lymphocytes is associated with patient prognosis in advanced gastric cancer. Oncology. 2007;73(3–4):215–20.
Pan QX, Su ZJ, Zhang JH, et al. A comparison of the prognostic value of preoperative inflammation-based scores and TNM stage in patients with gastric cancer. Onco Targets Ther. 2015;8:1375–85.
Kuroda D, Sawayama H, Kurashige J, et al. Controlling nutritional status (CONUT) score is a prognostic marker for gastric cancer patients after curative resection. Gastric Cancer. 2017; https://doi.org/10.1007/s10120-017-0744-3.
Melling N, Gruning A, Tachezy M, et al. Glasgow Prognostic Score may be a prognostic index for overall and perioperative survival in gastric cancer without perioperative treatment. Surgery. 2016;159:1548–56.
Yu X, Wen Y, Lin Y, et al. The value of preoperative Glasgow Prognostic Score and the C-reactive protein to albumin ratio as prognostic factors for long-term survival in pathological T1N0 esophageal squamous cell carcinoma. J Cancer. 2018;9(5):807–15.
Gao GD, Sun B, Wang XB, et al. Neutrophil to lymphocyte ratio as prognostic indicator for patients with esophageal squamous cell cancer. Int J Biol Markers. 2017;32(4):e409–14.
Hirahara N, Tajima Y, Fujii Y, et al. Prognostic nutritional index as a predictor of survival in resectable gastric cancer patients with normal preoperative serum carcinoembryonic antigen levels: a propensity score matching analysis. BMC Cancer. 2018;18(1):285.
Iseki Y, Shibutani M, Maeda K, et al. Impact of the preoperative controlling nutritional status (CONUT) score on the survival after curative surgery for colorectal cancer. PLoS One. 2015;10(7):e0132488.
Lu C, Gao P, Yang Y, et al. Prognostic evaluation of platelet to lymphocyte ratio in patients with colorectal cancer. Oncotarget. 2017;8(49):86287–95.
Kudou K, Saeki H, Nakashima Y, et al. C-reactive protein/albumin ratio is a poor prognostic factor of esophagogastric junction and upper gastric cancer. J Gastroenterol Hepatol. 2018; https://doi.org/10.1111/jgh.14442.
Siewert JR, Stein HJ. Carcinoma of the cardia: Carcinoma of the gastroesophageal junction-classification, pathology and extent of resection. Dis Esophagus. 1996;9:173–82.
Han WX, Chen ZM, Wei ZJ, et al. Preoperative pre-albumin predicts prognosis of patients after gastrectomy for adenocarcinoma of esophagogastric junction. World J Surg Oncol. 2016;14(1):279.
Zhang L, Su Y, Chen Z, et al. The prognostic value of preoperative inflammation-based prognostic scores and nutritional status for overall survival in resected patients with nonmetastatic Siewert type II/III adenocarcinoma of esophagogastric junction. Medicine (Baltimore). 2017;96(30):e7647.
Toyokawa T, Muguruma K, Tamura T, et al. Comparison of the prognostic impact and combination of preoperative inflammation-based and/or nutritional markers in patients with stage II gastric cancer. Oncotarget. 2018;9(50):29351–64.
Wen J, Bedford M, Begum R, et al. The value of inflammation based prognostic scores in patients undergoing surgical resection for oesophageal and gastric carcinoma. J Surg Oncol. 2018; 117(8):1697–707.
Aggarwal BB, Gehlot P. Inflammation and cancer: how friendly is the relationship for cancer patients? Curr Opin Pharmacol. 2009;9(4):351–69.
Crumley AB, Stuart RC, McKernan M, et al. Is hypoalbuminemia an independent prognostic factor in patients with gastric cancer? World J Surg. 2010;34(10):2393–8.
Lindenmann J, Fink-Neuboeck N, Koesslbacher M, et al. The influence of elevated levels of C-reactive protein and hypoalbuminemia on survival in patients with advanced inoperable esophageal cancer undergoing palliative treatment. J Surg Oncol. 2014;110:645–50.
Espinosa E, Feliu J, Zamora P, et al. Serum albumin and other prognostic factors related to response and survival in patients with advanced non–small cell lung cancer. Lung Cancer. 1995;12(1–2):67–76.
Asher V., Lee J., Bali A. Preoperative serum albumin is an independent prognostic predictor of survival in ovarian cancer. Med Oncol. 2012;29(3):2005–9.
Borda F, Borda A, Jimenez J, et al. Predictive value of pre-treatment hypoalbuminemia in prognosis of resected colorectal cancer. Gastroenterol Hepatol. 2014;37(5):289–95.
Ray-Coquard I, Cropet C, Van Glabbeke M, et al. Lymphopenia as a prognostic factor for overall survival in advanced carcinomas, sarcomas, and lymphomas. Cancer Res. 2009;69:5383–91.
Aoi W, Naito Y, Takagi T, et al. A novel myokine, secreted protein acidic and rich in cysteine (SPARC), suppresses colon tumorigenesis via regular exercise. Gut. 2013;62(6):882–9.
Hojman P, Dethlefsen C, Brandt C, et al. Exercise-induced muscle-derived cytokines inhibit mammary cancer cell growth. Am J Phys. Endocrinol Metab. 2011;301(3):E504–10.
Acknowledgment
The authors thank Editage Group (https://www.editage.jp/) for editing the draft of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare that they have no conflict of interest.
Ethical Standards
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Informed Consent
Informed consent to be included in the study, or the equivalent, was obtained from all patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
10434_2020_8821_MOESM1_ESM.tif
Supplementary Fig. 1. Comparison of the predictive ability of seven inflammation-based prognostic scores—NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI—by receiver operating characteristic (ROC) curve analyses. NLR neutrophil–lymphocyte ratio; PLR platelet-lymphocyte ratio; GPS Glasgow prognostic score; mGPS modified Glasgow prognostic score; CRP C-reactive protein; Alb albumin; PI prognostic index; PNI prognostic nutritional index (TIFF 29297 kb)
10434_2020_8821_MOESM2_ESM.tif
Supplementary Fig. 2 Comparison of the predictive ability of seven inflammation-based prognostic scores—NLR, PLR, GPS, mGPS, CRP/Alb ratio, PI, and PNI—by time-dependent receiver operating characteristic (ROC) curve analyses for (a) recurrence-free survival and (b) overall survival. NLR neutrophil–lymphocyte ratio; PLR platelet-lymphocyte ratio; GPS Glasgow prognostic score; mGPS modified Glasgow prognostic score; CRP C-reactive protein; Alb albumin; PI prognostic index; PNI prognostic nutritional index (TIFF 29297 kb)
10434_2020_8821_MOESM3_ESM.tif
Supplementary Fig. 3 Postoperative survival in patients with AEG and UGC based on prognostic index (PI). The Kaplan–Meier method was performed separately by tumor location. (a) Recurrence-free and (b) overall survival in patients with AEG. (c) Recurrence-free and (d) overall survival in patients with UGC. Kaplan–Meier analyses were performed according to the same criteria as in Fig. 1. AEG adenocarcinoma of esophagogastric junction; UGC upper gastric cancer; PI prognostic index(TIFF 29297 kb)
10434_2020_8821_MOESM4_ESM.tif
Supplementary Fig. 4 Postoperative survival in patients with AEG based on prognostic index (PI). The Kaplan–Meier method was performed separately by tumor location according to Siewert classification. (a) Recurrence-free and (b) overall survival in patients with Siewert type I. (c) Recurrence-free and (d) overall survival in patients with Siewert type II. (e) Recurrence-free and (f) overall survival in patients with Siewert type III. Kaplan–Meier analyses were performed according to the same criteria as in Fig. 1. AEG adenocarcinoma of esophagogastric junction; PI prognostic index (TIFF 29297 kb)
10434_2020_8821_MOESM5_ESM.tif
Supplementary Fig. 5 Postoperative survival in patients with AEG and UGC based on prognostic nutritional index (PNI). The Kaplan–Meier method was performed separately by tumor location. (a) Recurrence-free and (b) overall survival in patients with AEG. (c) Recurrence-free and (d) overall survival in patients with UGC. Kaplan–Meier analyses were performed according to the same criteria as in Fig. 2. AEG adenocarcinoma of esophagogastric junction; UGC upper gastric cancer; PNI prognostic nutritional index (TIFF 29297 kb)
10434_2020_8821_MOESM6_ESM.tif
Supplementary Fig. 6 Postoperative survival in patients with AEG based on prognostic nutritional index (PNI). The Kaplan–Meier method was performed separately by tumor location according to Siewert classification. (a) Recurrence-free and (b) overall survival in patients with Siewert type I. (c) Recurrence-free and (d) overall survival in patients with Siewert type II. (e) Recurrence-free and (f) overall survival in patients with Siewert type III. Kaplan–Meier analyses were performed according to the same criteria as in Fig. 2. AEG adenocarcinoma of esophagogastric junction; PNI prognostic nutritional index (TIFF 29297 kb)
Rights and permissions
About this article

Cite this article
Kudou, K., Nakashima, Y., Haruta, Y. et al. Comparison of Inflammation-Based Prognostic Scores Associated with the Prognostic Impact of Adenocarcinoma of Esophagogastric Junction and Upper Gastric Cancer. Ann Surg Oncol 28, 2059–2067 (2021). https://doi.org/10.1245/s10434-020-08821-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08821-y