
Abstract
Background
The National Comprehensive Cancer Network guidelines recommend R0 resection and targeted therapy, a combination of cytotoxic and molecular targeted agents, such as bevacizumab, cetuximab, and panitumumab, for colorectal cancer with synchronous peritoneal metastasis (M1c). While these therapeutic strategies are drawing attention, their efficacy has not been fully examined.
Methods
The study population comprised 248 consecutive M1c patients who were treated at the National Cancer Center Hospital from 1997 to 2013. Multivariate analyses were performed to evaluate relationships between overall survival and R0 resection and targeted therapy using Cox proportional hazards regression models.
Results
The 3-year overall survival (3 yOS) was 19.5%, and median survival time (MST) was 16.2 months in 248 M1c patients. R0 resection was performed in 34 patients (14%), yielding a 3-year overall survival (OS) of 48.3% and median survival time (MST) of 29.9 months. Targeted therapy was performed in 54 patients (22%) at least once during the course of treatment, yielding a 3-yr OS of 38.2% and MST of 23.9 months. After adjusting for other key clinical factors, such as the number of organs involved with metastases, performance status, primary tumor site, and extent of peritoneal metastasis, both R0 resection and targeted therapy were independent factors associated with longer OS. Targeted therapy was associated with a significantly longer OS compared with multiple cytotoxic agent therapy [hazard ratio 0.65; 95% confidence interval (0.44–0.94); p = 0.02].
Conclusions
If achievable, R0 resection is a desirable therapeutic strategy for patients with M1c colorectal cancer. Moreover, targeted therapy might be the optimal chemotherapy in this patient population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In the eighth edition of the tumor-node-metastasis classification published in 2017, colorectal cancer with peritoneal metastasis is newly categorized as M1c (i.e., metastasis to the peritoneum with or without other organ involvement) separately from M1a (metastasis to one organ) and M1b (metastasis to more than one organ), given the poor prognosis of peritoneal metastases compared with other metastatic diseases in visceral organs.1,2 With regard to therapeutic strategies, the National Comprehensive Cancer Network (NCCN) guidelines for colon cancer recommend systemic chemotherapy as an exclusive treatment choice and do not recommend aggressive cytoreductive debulking and/or intraperitoneal chemotherapy outside the setting of a clinical trial.3 In 2016, NCCN guidelines added the following footnote (page COL-8): “If R0 resection can be achieved, surgical resection of isolated peritoneal disease may be considered at experienced centers.”3 Hence, R0 resection (i.e., resection of only the diseased portion of the peritoneum), which differs from traditional cytoreductive surgery (i.e., resection of not only the diseased portion but also the entire peritoneum, i.e., peritonectomy) with hyperthermic intraperitoneal chemotherapy (HIPEC), was newly introduced as another treatment option for M1c colorectal cancer.4,5 We recently reported the long-term outcomes of 78 M1c colorectal cancer patients who underwent R0 resection without aggressive cytoreductive surgery or HIPEC; median survival time (MST) was 33.4 months, and the 5-year overall survival (OS) was 28.7%. These findings suggested that R0 resection is an acceptable surgical treatment option in this patient population.6
The introduction of molecular targeted agents, such as vascular endothelial growth factor-targeted antibody (bevacizumab) and epidermal growth factor receptor-targeted antibodies (cetuximab, panitumumab), has improved OS of stage IV colorectal cancer patients. Median OS of patients diagnosed with unresectable stage IV colorectal cancer has improved, from approximately 1 year during the era of 5-fluorouracil (5FU) monotherapy to > 30 months with the integration of multiple cytotoxic agents and molecular targeted agents.7 Combinations of cytotoxic agents and molecular target agents (i.e., targeted therapy) are now standard treatments for unresectable stage IV patients in various settings. A nationwide population-based study in the Netherlands showed that the addition of bevacizumab was associated with a longer OS in M1c patients.8 Conversely, the Analysis and Research in Cancers of the Digestive System Database reported that patients with peritoneal-only involvement had worse survival than M1a patients and that these survival differences were more marked in patients who received systemic regimes, including targeted therapy compared with those who did not, suggesting that targeted agents are less effective for M1c than for M1a.2 The effectiveness of targeted therapy in M1c patients has not been clarified.
While R0 resection and targeted therapy have become the focus of attention as therapeutic strategies for M1c, few studies have examined their efficacy. Therefore, the present study was designed to evaluate the prognostic impact of R0 resection and targeted therapy in patients with M1c colorectal cancer, specifically with respect to OS. During the study period, targeted molecular agents (bevacizumab, cetuximab, and panitumumab) were introduced in Japan for use in systemic chemotherapy for stage IV colorectal cancer. Thus, the first half of our patients received no targeted therapy but underwent 5FU monotherapy or multiple cytotoxic agent therapy. This heterogeneity makes it possible to investigate the efficacy of targeted therapy in our cohort. Multivariate analyses were performed to adjust for other key clinical factors: performance status, number of organs involved with metastases, primary tumor site, and extent of peritoneal metastasis, which have been shown to be prognostic factors for stage IV colorectal cancer.2,9,10,11
Methods
Study Population
Subjects were patients with M1c colorectal adenocarcinoma who were treated at the National Cancer Center Hospital from January 1997 to December 2013. Synchronous peritoneal metastases were diagnosed by the presence of peritoneal tumors, which were resected and histologically proven to be peritoneal metastases of colorectal cancer, or by computed tomography images with multiple peritoneal nodules. Patients who received best supportive care only and those undergoing cytotoxic chemotherapy for other concomitant advanced cancer were excluded. Initial treatment decisions were typically made by a multidisciplinary team, including colorectal surgeons, medical oncologists, hepatobiliary surgeons, thoracic surgeons, and radiologists, taking into consideration disease severity and patient condition including comorbidities. Because targeted molecular agents were introduced in Japan for use in systemic chemotherapy for stage IV colorectal cancer during the study period (after 2007), the first half of the patients received no targeted therapy but underwent 5FU monotherapy or multiple cytotoxic agent therapy. This retrospective study was approved by the Institutional Review Board (IRB) of the National Cancer Center Hospital (IRB code: 2015-320).
Data Collection
The following parameters were retrospectively assessed using medical records: age, sex, type of surgery (R0 resection: primary tumor resection and metastasectomy, including dissection of the diseased portion of the peritoneum such that no macroscopic tumors remained; palliative primary tumor resection: primary tumor resection without metastasectomy; and nonresection: diverting stoma construction without resection of primary tumor, bypass surgery, or probe laparotomy), type of systemic chemotherapy (5FU monotherapy; multiple cytotoxic agent therapy, i.e., multiple cytotoxic agent therapy without molecular targeted agents, e.g., 5FU plus oxaliplatin and 5FU plus irinotecan; and targeted therapy, i.e., combination of cytotoxic agents with at least one molecular targeted agent, i.e., bevacizumab, cetuximab, or panitumumab), number of organs involved with metastases, ECOG performance status (PS), primary tumor site (right side: cecum, hepatic flexure, and transverse colon; left side: splenic flexure, sigmoid, rectosigmoid junction, and rectum), and extent of peritoneal metastasis (a few: peritoneal metastasis only to the adjacent peritoneum (P1) or a few metastases to the distant peritoneum (P2); diffuse: diffuse metastases to the distant peritoneum (P3), as defined by the Japan Society for Cancer of the Colon and Rectum (JSCCR) in the Japanese classification of colorectal carcinoma).12 A PCI score of P1 seems to range from 1 to 6.13,14 A PCI score of P2 seems to range from 4 to 20, and a PCI score of P3 seems to be higher than 10.13,14
Statistical Analysis
Pearson’s Chi square test for categorical variables and the Wilcoxon rank-sum test for continuous variables were performed to compare various factors in both groups. OS was defined as the interval between the date of stage IV colorectal cancer diagnosis and the date of death from all causes and censored for survivors at the date of data cutoff (July 2017). The Kaplan–Meier method was used to estimate OS. Differences in survival were assessed with the log-rank test. Multivariate Cox proportional hazards regression models were used to evaluate the prognostic impact of R0 resection and targeted therapy on OS, by adjusting for four key clinical factors (i.e., number of organs involved with metastases, performance status, primary tumor site, and extent of peritoneal metastasis). Results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs).
Data are presented as numbers of patients, ratios (%), or HR and 95% CI as indicated. p < 0.05 was considered statistically significant. All statistical analyses were performed using the JMP12 software program (SAS Institute Japan Ltd., Tokyo, Japan).
Results
Characteristics of the Study Cohort
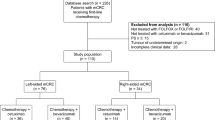
Figure 1 shows the flowchart of patient selection. Between 1997 and 2013, a total of 1067 patients with stage IV CRC were referred to the National Cancer Center. Of these, 262 (24.6% of all stage IV patients) had synchronous peritoneal metastasis (M1c). Because our analysis focused on therapeutic strategies for M1c, we excluded 12 patients who only received best supportive care, and 2 patients who were undergoing chemotherapy for other concomitant advanced cancer. The final study population thus comprised 248 consecutive patients who underwent resection surgery and/or chemotherapy.

Study cohort. After excluding patients who received best supportive care only (n = 12) and those undergoing chemotherapy for other concomitant advanced cancer (n = 2) from the initial 262 colorectal cancer patients with synchronous peritoneal metastasis (M1c), the final study population consisted of 248 patients
Patient characteristics are shown in Table 1. Because almost two-thirds of the entire cohort (63%) had not only peritoneal metastases but also nonperitoneal distant metastases, an aggressive surgical approach was not typically adopted. Thirty-four patients underwent R0 resection, 134 underwent palliative primary tumor resection, and 80 underwent systemic chemotherapy immediately after diagnosis (nonresection). For systemic chemotherapy, 51 patients received 5FU monotherapy, 116 received multiple cytotoxic agent therapy, and 54 received systemic regimes including targeted therapy. Twenty-seven patients who underwent surgery did not receive any chemotherapy. None of the patients in our series received HIPEC.
Long-term Outcomes of M1c Patients
The 3- and 5-year OS rates were 19.5 and 11.0%, respectively, with a median follow-up time for survivors of 40 (range 2–158) months. Median survival time (MST) was 16.2 months. Notably, 13 patients survived for more than 5 years (Fig. 2).

Overall survival curve for colorectal cancer patients with synchronous peritoneal metastasis (M1c) (n = 248)
Figure 3A shows OS curves for M1c patients stratified into three groups by type of surgery. Patients who underwent R0 resection (3-year OS: 48.3%, MST: 29.9 months) had better OS than those who underwent palliative primary tumor resection (3-year OS: 19.1%, MST: 16.1 months). Patients who did not undergo resection (3-year OS: 6.9%, MST: 11.2 months) had worse OS than those who underwent palliative primary tumor resection.

Overall survival curves for M1c patients stratified into three groups according to the type of surgery (R0 resection, palliative primary tumor resection, and nonresection) (a), and for M1c patients stratified into four groups according to the type of chemotherapy (none, 5FU monotherapy, multiple cytotoxic agent therapy, and systemic regimens including targeted therapy) (b)
Figure 3b shows OS curves for M1c patients stratified into four groups by type of chemotherapy. Patients who received 5FU monotherapy (3-year OS: 20.2%, MST: 8.7 months) had similar OS compared with those who did not receive any chemotherapy (3-year OS: 14.8%, MST: 7.1 months). Compared with these patients, patients who received multiple cytotoxic agent therapy (3-year OS: 16.4%, MST: 16.5 months) showed better OS, and moreover, patients who received systemic regimes, including targeted therapy (3-year OS: 38.2%, MST: 23.9 months) showed much better OS.
Factors affecting Prognosis of M1c
According to univariate analysis, good performance status (PS0 or PS1) (p < 0.0001), involvement of only one organ (peritoneal only) (p < 0.0001), primary tumor site (left side) (p = 0.045), and peritoneal metastasis (a few) (p < 0.0001) were significantly associated with better OS, whereas sex and age were not associated with prognosis (Table 2).
To investigate the prognostic impact of R0 resection and targeted therapy, multivariate analyses were performed using Cox proportional hazards regression models to adjust for the above-mentioned four key clinical factors. R0 resection was associated with a significantly longer OS compared with nonresection [HR 0.28; 95% CI (0.14–0.54); p < 0.0001] and palliative primary tumor resection [HR 0.47; 95% CI (0.27–0.79); p = 0.004; Table 2). Targeted therapy also was associated with a significantly longer OS compared with 5FU monotherapy [HR 0.32; 95% CI (0.20–0.50); p < 0.0001] and multiple cytotoxic agent therapy [HR 0.65; 95% CI (0.44–0.94); p = 0.02; Table 2]. Moreover, both R0 resection and targeted therapy were found to be independent factors associated with better prognosis, after adjusting for the four key clinical factors (i.e., number of organs involved with metastases, performance status, primary tumor site, and extent of peritoneal metastasis; Table 2).
Discussion
In the present study, our patients (n = 248) had a 3-year OS of 19.5%, 5-year OS of 11.0%, and MST of 16.2 months, suggesting that patients with M1c colorectal cancer have a significantly shorter OS compared with those with metastases to other sites. We revealed both R0 resection and targeted therapy to be independent factors associated with longer OS in patients with M1c colorectal cancer, after adjusting for the four key clinical factors: performance status, primary tumor site, number of organs involved with metastases, and extent of peritoneal metastasis. For patients with metastatic colorectal cancer, well-known prognostic factors included performance status, primary tumor site, and number of organs involved with metastases.2,9,10 Extent of peritoneal metastasis is widely known as a prognostic factor for M1c colorectal cancer.11 Consistent with these reports, good performance status, tumor location on the left side, peritoneal-only metastasis, and a few peritoneal metastases were all associated with better prognosis in the present study. The results of our multivariate analyses suggest that resection of visible peritoneal metastases should be recommended as a therapeutic strategy for M1c colorectal cancer if R0 resection appears achievable, and systemic regimes, including targeted therapy, should be considered as the optimal chemotherapy.
Japan has adopted unique therapeutic strategies to address peritoneal metastasis of colorectal cancer, which differ from those of Western countries.15 Specifically, R0 resection is performed when peritoneal metastasis extends only to the adjacent peritoneum (P1) and is considered if there are a few easily resectable peritoneal metastases to the distant peritoneum (P2).15 Although R0 resection can be achieved only in selected patients due to diffuse peritoneal metastasis and/or synchronous hematogenous metastasis, the Study Group for Peritoneal Metastasis from Colorectal Cancer by the JSCCR reported that 224 (18%) of 1217 consecutive M1c patients underwent R0 resection between 1991 and 2007.16 Similarly, R0 resection was achieved in 14% of all M1c patients in the present cohort. Moreover, none of our M1c patients received HIPEC, which is consistent with data from a nationwide multicenter registry of the JSCCR covering approximately 10% of all patients with colorectal cancer in Japan.17,18 With these strategies, Japan has achieved a 5-year OS of roughly 30% after R0 resection in patients with M1c colorectal cancer without performing aggressive cytoreductive surgery or HIPEC.6,16 On the other hand, the median 5-year survival in previous studies for patients undergoing cytoreductive surgery with HIPEC was reported to be an average of 30 months for those with limited peritoneal metastases, and one study reported the 5-year OS rate as 29.7% for colon cancer and 37.9% for rectal cancer.19,20,–21 Based on these results, R0 resection seems an acceptable surgical treatment option in this particular patient population.
Interestingly, 5FU monotherapy did not show any survival benefit over palliative primary tumor resection without chemotherapy [HR 0.83; 95% CI (0.50–1.41); p = 0.49] (data not shown). Multiple cytotoxic agent therapy had a significant survival benefit over 5FU monotherapy [HR 0.49; 95% CI (0.34–0.71); p = 0.0003], whereas targeted therapy had a significant survival benefit over multiple cytotoxic agent therapy [HR 0.65; 95% CI (0.44–0.94); p = 0.02; Table 2]. These results suggest that, for peritoneal metastases, systemic regimes, including targeted therapy, are the most effective, followed by multiple cytotoxic agent therapy, whereas 5FU monotherapy was less effective.
In this study, we stratified the entire cohort into three groups according to the type of surgery (i.e., R0 resection, palliative primary tumor resection, and nonresection). We distinguished between palliative primary tumor resection and nonresection for the following reason: for unresectable stage IV colorectal cancer, several studies using propensity analyses reported that palliative primary tumor resection was associated with longer OS.22,23 Unlike other types of stage IV colorectal cancer, the survival benefit of palliative primary tumor resection has not been clarified for M1c. In the present multivariate analyses, palliative primary tumor resection showed a significant survival benefit over chemotherapy alone (nonresection) for unresectable M1c colorectal cancer [HR 0.59; 95% CI (0.41–0.84); p = 0.004; Table 2]. Thus, in this patient population, palliative primary tumor resection might be more beneficial than chemotherapy alone in terms of survival. Given the heterogeneity and potential selection bias between the two groups, further studies will be needed to confirm these results.
During the study period, recurrence after R0 resection (n = 34) was observed in 21 patients (62%), with the peritoneum as the most frequent recurrence site (n = 10). Hematogenous recurrence in the liver (n = 9), lungs (n = 6) as well as local recurrence (n = 2) also were observed (data not shown). Because of the high recurrence rate, adjuvant chemotherapy (i.e., chemotherapy just after resection) was performed for some of these patients. Of the 34 patients who underwent R0 resection, 14 patients (41%) received adjuvant chemotherapy (i.e., chemotherapy just after resection) for 6 months; 8 were treated with 5-FU monotherapy, 4 were treated with multiple cytotoxic agent therapy (5-FU plus oxaliplatin), and 2 were treated with systemic regimes, including targeted therapy (data not shown). Two patients who were treated with targeted therapy had several metastases to the distant peritoneum (P2), although macroscopic R0 resection was achieved. Whereas both anti-VEGF and anti-EGFR therapy drugs have failed in postresection setting in stage III disease, efficacy of these agents for M1c colorectal cancer in post R0 resection setting, not at the time of recurrence, remains unknown.24,25,–26
There are some limitations to this study. First, because the study was retrospective in design, biases may exist. Second, although consecutive patients were enrolled, the study period was from 1997 to 2013. During this long period, treatment strategies, including chemotherapy, have changed significantly, as well as the perioperative awareness of peritoneal metastasis; therefore, our data may not be comparable to other studies with novel approaches. Third, the sample size was relatively small, which could affect the results. Nonetheless, the present findings warrant further consideration and validation in a larger patient series of colorectal cancer with synchronous peritoneal metastases.
In conclusion, our results suggest both R0 resection and targeted therapy are independent factors associated with better prognosis in patients with M1c colorectal cancer, after adjusting for four key clinical factors (i.e., number of organs involved with metastases, performance status, primary tumor site, and extent of peritoneal metastasis). Thus, resection of visible peritoneal metastases should be recommended as a therapeutic strategy for colorectal cancer with synchronous peritoneal metastasis, if R0 resection appears achievable, and systemic regimes, including targeted therapy should be considered as the optimal chemotherapy for M1c.
References
UICC. TNM classification of malignant tumours eighth edition. New York: John Wiley & Sons, Ltd; 2017.
Franko J, Shi Q, Meyers JP, et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. Lancet Oncol. 2016;17(12):1709–19.
Benson AB, 3rd, Venook AP, Cederquist L, et al. Colon Cancer, Version 1.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15(3):370–98.
Mulsow J, Merkel S, Agaimy A, Hohenberger W. Outcomes following surgery for colorectal cancer with synchronous peritoneal metastases. Br J Surg. 2011;98(12):1785–91.
Sugarbaker PH, Ryan DP. Cytoreductive surgery plus hyperthermic perioperative chemotherapy to treat peritoneal metastases from colorectal cancer: standard of care or an experimental approach? Lancet Oncol. 2012;13(8):e362–9.
Shida D, Tsukamoto S, Ochiai H, Kanemitsu Y. Long-term outcomes after R0 resection of synchronous peritoneal metastasis from colorectal cancer without cytoreductive surgery or hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2018;25(1):173–8.
Fakih MG. Metastatic colorectal cancer: current state and future directions. J Clin Oncol. 2015;33(16):1809–24.
Razenberg LG, van Gestel YR, Lemmens VE, de Hingh IH, Creemers GJ. Bevacizumab in addition to palliative chemotherapy for patients with peritoneal carcinomatosis of colorectal origin: a nationwide population-based study. Clin Colorectal Cancer. 2016;15(2):e41–6.
Stillwell AP, Ho YH, Veitch C. Systematic review of prognostic factors related to overall survival in patients with stage IV colorectal cancer and unresectable metastases. World J Surg. 2011;35(3):684–92.
Arnold D, Lueza B, Douillard JY, et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann Oncol. 2017;28(8):1713–29.
Vallicelli C, Cavaliere D, Catena F, et al. Management of peritoneal carcinomatosis from colorectal cancer: review of the literature. Int J Colorectal Dis. 2014;29(8):895–8.
Japanese Society for Cancer of the Colon and Rectum. Japanese classification of colorectal carcinoma (8th edn). Tokyo: Kanehara & Co., Ltd; 2013.
Kobayashi H, Kotake K, Sugihara K, Study Group for Peritoneal Metastasis from Colorectal Cancer by the Japanese Society for Cancer of the C, Rectum. Enhancing the objectivity of the Japanese classification of peritoneal metastases from colorectal cancer. Jpn J Clin Oncol. 2014;44(10):898–902.
Shida D, Tsukamoto S, Ochiai H, Kanemitsu Y. Long-term outcomes after R0 resection of synchronous peritoneal metastasis from colorectal cancer without cytoreductive surgery or hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2017;25(1):173–178.
Watanabe T, Muro K, Ajioka Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. Int J Clin Oncol. 2017;23(1):1–34.
Sato H, Maeda K, Kotake K, Sugihara K, Takahashi H. Factors affecting recurrence and prognosis after R0 resection for colorectal cancer with peritoneal metastasis. J Gastroenterol. 2016;51(5):465–72.
Noura S, Ohue M, Ito Y, et al. New staging system for colorectal cancer patients with synchronous peritoneal metastasis in accordance with the Japanese classification of colorectal carcinoma: a multi-institutional study. Dig Surg. 2016;33(1):66–73.
Kobayashi H, Kotake K, Sugihara K. Outcomes of surgery without HIPEC for synchronous peritoneal metastasis from colorectal cancer: data from a multi-center registry. Int J Clin Oncol. 2014;19(1):98–105.
Elias D, Gilly F, Boutitie F, et al. Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol. 2010;28(1):63–8.
Ihemelandu C, Sugarbaker PH. Management for peritoneal metastasis of colonic origin: role of cytoreductive surgery and perioperative intraperitoneal chemotherapy: a single institution’s experience during two decades. Ann Surg Oncol. 2017;24(4):898–905.
Elias D, Glehen O, Pocard M, et al. A comparative study of complete cytoreductive surgery plus intraperitoneal chemotherapy to treat peritoneal dissemination from colon, rectum, small bowel, and nonpseudomyxoma appendix. Ann Surg. 2010;251(5):896–901.
Shida D, Hamaguchi T, Ochiai H, et al. Prognostic impact of palliative primary tumor resection for unresectable stage 4 colorectal cancer: using a propensity score analysis. Ann Surg Oncol. 2016;23(11):3602–8.
Tarantino I, Warschkow R, Worni M, et al. Prognostic relevance of palliative primary tumor removal in 37,793 metastatic colorectal cancer patients: a population-based, propensity score-adjusted trend analysis. Ann Surg. 2015;262(1):112–20.
Allegra CJ, Yothers G, O’Connell MJ, et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J Clin Oncol. 2011;29(1):11–6.
Alberts SR, Sargent DJ, Nair S, et al. Effect of oxaliplatin, fluorouracil, and leucovorin with or without cetuximab on survival among patients with resected stage III colon cancer: a randomized trial. JAMA. 2012;307(13):1383–93.
Taieb J, Tabernero J, Mini E, et al. Oxaliplatin, fluorouracil, and leucovorin with or without cetuximab in patients with resected stage III colon cancer (PETACC-8): an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(8):862–73.
Disclosure
None to report.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Shida, D., Yoshida, T., Tanabe, T. et al. Prognostic Impact of R0 Resection and Targeted Therapy for Colorectal Cancer with Synchronous Peritoneal Metastasis. Ann Surg Oncol 25, 1646–1653 (2018). https://doi.org/10.1245/s10434-018-6436-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-018-6436-3