
Abstract
Background
Hospital volume is known to be a crucial factor in reducing postoperative morbidity and mortality in laparoscopic gastrectomy for gastric cancer. However, it is unclear whether surgeon’s individual experience can overcome the effect of hospital volume.
Methods
Clinicopathologic data of initial 50 laparoscopic gastrectomy cases were collected from six gastric cancer surgeons. Half of the six surgeons worked in high-volume centers, and the other half worked in low-volume hospitals. Perioperative outcomes were compared between the high-volume centers and the low-volume hospitals.
Results
Three low-volume hospitals in this study contained significantly more male and older patients with a higher American Society of Anesthesiologists score than high-volume centers. Although high- and low-volume hospitals mainly used laparoscopy-assisted and totally laparoscopic approach, respectively, there were no differences between the two groups in the extent of resection, operating time, estimated blood loss, and number of collected lymph nodes. Postoperative recovery such as duration to soft diet and hospital stay did not differ between the high- and the low-volume hospitals. No significant difference was found in postoperative morbidities by Clavien–Dindo classification. There was no mortality reported in both groups of the enrolled hospitals.
Conclusions
Hospital volume is not a decisive factor in affecting postoperative morbidity and mortality for well-trained beginners in laparoscopic surgery for gastric cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Laparoscopic surgery for gastric cancer is a complex procedure in which gastrectomy, lymph node dissection around major blood vessels, and various reconstructions are performed with the aid of laparoscopic instruments.1–3 As a result, most surgeons require considerable amount of time or show a long learning curve to become skillful laparoscopic operators for gastric cancer.4,5 Before reaching a plateau in the learning curve, postoperative outcomes for initial cases are influenced by various factors in addition to individual abilities.6 Hospital volume is often reported to be one of the most important factors in affecting the beginner’s outcomes in laparoscopic gastric cancer surgery, and surgeons working in a high-volume center tend to have better initial outcomes compared to those in a low-volume hospital.7,8
Most high-volume centers are set up with an optimized surgical unit for various laparoscopic surgeries and have a specialized surgical team composed of skillful first assistant, scopist, and scrub nurses.9 In such circumstances, a novice surgeon would more likely perform a safer and more stable laparoscopic surgery because the specialized unit or team can compensate for the novice surgeon’s shortcoming.10 However, a surgeon working in a low-volume hospital, in which laparoscopic system might not have been established, must prepare laparoscopic devices and instruct assistants alone, which could lead to relatively poor surgical outcomes.11 However, once a beginning surgeon is trained to be a fellow in a high-volume center, it is considered that the effect of hospital volume is no longer a determinant factor in the treatment of gastric cancer. In other words, individual experience or training could overcome the latent disadvantages of low-volume hospitals. To prove the hypothesis, initial experiences of surgeons who are conducting laparoscopic surgery of gastric cancer were collected from several institutions, including high-volume centers and low-volume hospitals.
Materials and Methods
Patients and Data Collection
A high-volume center and a low-volume hospital were defined by the number of gastric cancer operations performed in 1 year: in a high-volume center, more than 100 gastric cancer operations were performed 1 year, while in a low-volume hospital, fewer than 100 gastric cancer operations were performed in that time.9,12–14
Six gastric cancer surgeons were recruited in this study. Three of them worked in high-volume hospitals, while the other three surgeons worked in low-volume hospitals. Each surgeon was trained for 2–3 years in high-volume centers such as tertiary-care university hospitals before moving to current workplace. They have performed at least 180 open and laparoscopic gastrectomy cases in 1 year as operator or the first assistant during fellowship training. All teaching staffs of recruited six surgeons were specialized gastric cancer surgeons who had more than 20 years’ experience in gastric cancer operations. The details of the training of six surgeons are summarized in Table 1. The ages of the six surgeons ranged from late 30 s to mid-40 s. Approximately 50 initial laparoscopic gastrectomy cases were collected from each surgeon for the study. Eligibility criteria for enrolled surgeons and cases are described in Fig. 1.

Surgeons and case selection from each institution
Clinical data of the enrolled patients including demographics and operative details, pathologic data, and short-term postoperative outcomes were collected retrospectively from the gastric cancer registry of the surgeons’ hospitals.
Preoperative clinical characteristics were classified according to the American Society of Anesthesiologists (ASA) classification. The pathologic stage was classified according to the 7th edition of the American Joint Cancer Committee tumor, node, metastasis (TNM) classification system. Postoperative morbidities were categorized with the Clavien–Dindo classification.15
This study was approved by the institutional review board of the Ethics Committee of the enrolled institutions (UC16RIMI0018). Patient records were anonymized and deidentified before analysis.
Statistical Analysis
Differences between the two groups were analyzed by Student’s t test for continuous variables and Chi square test or Fisher’s exact test for proportions. Statistical analyses were performed by SPSS 13.0 software (IBM SPSS, Chicago, IL, USA). Values of P < 0.05 were deemed to indicate statistical significance.
Results
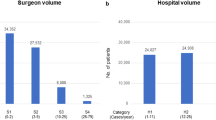
Excluding unmatched cases with enrollment criteria, a total of 284 patients were finally included in the present study: 137 patients and 147 patients belonged to the high-volume centers and the low-volume hospitals, respectively (Fig. 1). Enrolled high-volume centers have been conducting gastric cancer surgeries more than 300 cases (mean 473.7 ± 161.9, median [range] 375 [365–820]) in 1 year and low-volume hospitals have been conducting about 80 cases (mean 80.4 ± 12.0, median [range] 82 [61–99]) in 1 year. Three surgeons in high-volume centers performed their initial laparoscopic gastrectomy in 2006–2007, 2010–2011, and 2015–2016, respectively. Three surgeons in low-volume hospitals performed their initial laparoscopic gastrectomy in 2010–2012, 2012–2013, and 2013–2015, respectively. All enrolled hospitals had adopted a clinical pathway for perioperative management in these years.
The patients in high-volume centers were younger in age and were composed of more female patients. Although there was no difference in body mass index between the two groups, ASA scores of the patients in low-volume hospitals were significantly higher than those in high-volume centers (Table 2).
In high-volume centers the laparoscopy-assisted approach was commonly performed, whereas in low-volume hospitals more than 90% of the patients underwent totally laparoscopic gastrectomy (P < 0.001). In both groups, distal subtotal gastrectomy was performed most frequently. However, surgeons in high-volume centers preferred the Billroth I anastomosis followed by the Billroth II, while the surgeons in low-volume hospitals selected Billroth II anastomosis followed by Roux-en-Y reconstruction (P < 0.001). Although surgeons in low-volume hospitals conducted significantly more extended lymph node dissections compared to those in high-volume centers (P < 0.001), operating time and estimated blood loss during the operation did not differ between the two groups (Table 2).
Pathologic features of the two groups are described in Table 3. In both groups, laparoscopic gastrectomy was performed most commonly in stage I gastric cancer, and the R0 resection rate was almost the same. There were no differences between the two groups in all tumor characteristics, including the number of collected lymph node and TNM stage.
Postoperative recovery measures such as time to soft diet and discharge did not significantly differ, even though the patients in low-volume hospitals tended to stay longer than those in high-volume centers. In terms of short-term (within 30 postoperative days) morbidity according to the Clavien–Dindo classification, there was no significant difference between the two groups. No mortality was reported in either group (Table 4).
Discussion
Both hospital volume and surgeon’s experience have a strong influence on the postoperative outcomes of gastric cancer surgery.16–18 Most hospitals with numerous operating cases possess established operating unit and pre- and postoperative system for patients’ care.17 Additionally, a specialized surgical team is prepared to assist the operator’s procedure.19 In case of cancer surgery, surgeon’s experience is doubtless extremely important for postoperative complications and long-term survival.20,21 Especially in laparoscopic surgery, a well-arranged surgical unit and team along with the surgeon’s individual experience play a more crucial role compared to open surgeries.9 However, there has been no report addressing which factor is more important or more effective in determining the patients’ outcomes. To resolve this question, data from one hospital or one surgeon are clearly not enough. Therefore, the present study was designed to be multi-institutional, and surgeons from both high- and low-volume hospitals were recruited. In addition, the number of surgeons in the two groups was equally controlled, considering the number of enrolled patients. The criterion for the surgeons’ experience was defined as fellowship training of 2–3 years before beginning their own laparoscopic gastric cancer operations in their current workplace.22,23 In terms of fellowship, all recruited surgeons were trained in tertiary-care and teaching university hospitals, in which more than 400 gastric cancer surgeries are performed every year.
The composition of the patients in high-volume centers and low-volume hospitals was significantly different with respect to age, gender, and ASA score. The ASA score is one of the most important factors to influence the postoperative course.24,25 Patients in the low-volume hospitals had a higher ASA score than those in the high-volume centers; this can be explained by the significantly older age of the patients in the low-volume hospitals. The higher ASA score in low-volume hospitals can also be explained by the lower socioeconomic status of the patients and the relatively rural location of the hospitals.
In high-volume centers a laparoscopy-assisted approach was commonly used, whereas in low-volume hospitals most patients underwent gastrectomy through a totally laparoscopic approach. This phenomenon should not be attributed to the preference or the technique of the surgeons but rather to the trend of time.26 Two surgeons in high-volume centers had implemented most of their initial cases before 2010, when laparoscopy-assisted gastrectomy using extracorporeal anastomosis was popular.27 On the other hand, all surgeons in the low-volume hospitals had started their own operations after 2010, when totally laparoscopic gastrectomy with intracorporeal anastomosis was adopted and was rapidly increasing in frequency.28 The differences regarding the extent of lymph node dissection and reconstruction method may be attributed to the surgeons’ preference. Considering that the operating time and the amount of blood loss were not different between the two groups despite the different operative method and course, we think that the initial laparoscopic techniques used by the surgeons in low-volume hospitals are virtually the same as those used in high-volume centers for gastric cancer operation. Although surgeons in low-volume hospitals conducted significantly more extended lymph node dissections compared to those in high-volume centers, the number of retrieved lymph nodes did not differ between the two groups. In fact, the difference between D2 and D1+ dissection is whether to include lymph node station 11p or 12a in dissection. Inclusion of one station or two stations actually might not affect the total number of retrieved lymph node. Additionally, similar numbers of retrieved lymph nodes also reflect the similar level of laparoscopic gastric cancer surgeries in the two groups.
In addition to operative technique, surgeons’ experience related to perioperative care can affect the postoperative course of gastric cancer patients.29 As mentioned before, patients in low-volume hospitals underwent laparoscopic surgery of a similar level as that of the high-volume centers. However, they had significantly worse preoperative characteristics, such as old age and higher ASA score. In spite of such relatively unfavorable conditions, the short-term (within 30 postoperative days) outcome was not different between the two groups. These results indicate that surgeons’ overall operative skill and experience in postoperative care overcame the effect of preoperative risk of patients as well as the effect of hospital volume. The duration of hospital stay in low-volume hospitals was longer than that in high-volume centers, although there was no statistical significance between the two groups. The relatively long duration of stay in low-volume hospitals could be explained by two reasons. First, the low-volume group included two postoperative morbidity cases according to the Clavien–Dindo classification, IIIb and IVa. The IIIb and IVa cases were duodenal stump leakage and esophagojejunostomy leakage, respectively, and they required a longer-term in-hospital treatment. Second, the high-volume centers are characterized by a more aggressive application of the clinical pathway and a subsequently higher hospital room turnover rate.30,31
Our study has several limitations. In a cancer-related study, it is thought that long-term outcomes, including overall survival rate, are informative and necessary to prove a study’s validity. In this study, long-term data of patients were not obtained because of the short follow-up time of a few surgeons, although most patients of both groups had stage I gastric cancer, which has a favorable prognosis. Second, the present study had a retrospective design. Third, our results could be applied to laparoscopic surgery for cancer with high prevalence rate that facilitate surgical training through many operations, such as gastric cancer surgery in an East Asian country.
To sum up, regardless of preoperative patients’ characteristics and operative methods, well-trained beginner surgeons working in either low- or high-volume hospitals achieved similar short-term outcomes in laparoscopic gastric cancer surgery. These results suggest that the surgeons’ experience is the most important factor in affecting the postoperative outcomes; their experience can offset the effect of hospital volume in laparoscopic surgery. In other words, the surgeons’ experience gained through exhaustive training during their fellowship period is necessary in order to perform laparoscopic surgery without difficulty in gastric cancer.
References
Ecker BL, Datta J, McMillan MT, et al. Minimally invasive gastrectomy for gastric adenocarcinoma in the United States: utilization and short-term oncologic outcomes. J Surg Oncol. 2015;112:616–21.
Maduekwe UN, Yoon SS. An evidence-based review of the surgical treatment of gastric adenocarcinoma. J Gastrointest Surg. 2011;15:730–41.
Kim CH, Song KY, Park CH, Seo YJ, Park SM, Kim JJ. A comparison of outcomes of three reconstruction methods after laparoscopic distal gastrectomy. J Gastric Cancer. 2015;15:46–52.
Yoo CH, Kim HO, Hwang SI, Son BH, Shin JH, Kim H. Short-term outcomes of laparoscopic-assisted distal gastrectomy for gastric cancer during a surgeon’s learning curve period. Surg Endosc. 2009;23:2250–7.
Jung do H, Son SY, Park YS, et al. The learning curve associated with laparoscopic total gastrectomy. Gastric Cancer. 2016;19:264–72.
Kim MG, Kim KC, Yook JH, Kim BS, Kim TH, Kim BS. A practical way to overcome the learning period of laparoscopic gastrectomy for gastric cancer. Surg Endosc. 2011;25:3838–44.
Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–37.
Dikken JL, Verheij M, Cats A, Jansen EP, Hartgrink HH, van de Velde CJ. Extended lymph node dissection for gastric cancer from a European perspective. Gastric Cancer. 2011;14:396–8.
Kim MG, Kwon SJ. Comparison of the outcomes for laparoscopic gastrectomy performed by the same surgeon between a low-volume hospital and a high-volume center. Surg Endosc. 2014;28:1563–70.
Tokunaga M, Hiki N, Fukunaga T, et al. Learning curve of laparoscopy-assisted gastrectomy using a standardized surgical technique and an established educational system. Scand J Surg. 2011;100:86–91.
Yang SJ, Ahn EJ, Park SH, Kim JH, Park JM. The early experience of laparoscopy-assisted gastrectomy for gastric cancer at a low-volume center. J Gastric Cancer. 2010;10:241–6.
Murata A, Okamoto K, Muramatsu K, Matsuda S. Endoscopic submucosal dissection for gastric cancer: the influence of hospital volume on complications and length of stay. Surg Endosc. 2014;28:1298–306.
Ichikawa D, Komatsu S, Kubota T, et al. Effect of hospital volume on long-term outcomes of laparoscopic gastrectomy for clinical stage I gastric cancer. Anticancer Res. 2013;33:5165–70.
Kim TH, Kim JJ, Kim SH, et al. Diagnostic value of clinical T staging assessed by endoscopy and stomach protocol computed tomography in gastric cancer: the experience of a low-volume institute. J Gastric Cancer. 2012;12:223–31.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187–96.
Brisinda G, Crocco A, Tomaiuolo P, Santullo F, Mazzari A, Vanella S. Extended or limited lymph node dissection? A gastric cancer surgical dilemma. Ann Surg. 2012;256:e30–1.
Sabesan A, Petrelli NJ, Bennett JJ. Outcomes of gastric cancer resections performed in a high volume community cancer center. Surg Oncol. 2015;24:16–20.
Dikken JL, Wouters MW, Lemmens VE, et al. Influence of hospital type on outcomes after oesophageal and gastric cancer surgery. Br J Surg. 2012;99:954–63.
Murata A, Muramatsu K, Ichimiya Y, Kubo T, Fujino Y, Matsuda S. Influence of hospital volume on outcomes of laparoscopic gastrectomy for gastric cancer in patients with comorbidity in Japan. Asian J Surg. 2015;38:33–9.
Liang Y, Wu L, Wang X, Ding X, Liang H. The positive impact of surgeon specialization on survival for gastric cancer patients after surgery with curative intent. Gastric Cancer. 2015;18:859–67.
Kim CY, Nam BH, Cho GS, et al. Learning curve for gastric cancer surgery based on actual survival. Gastric Cancer. 2016;19:631–8.
You YH, Kim YM, Ahn DH. Beginner surgeon’s initial experience with distal subtotal gastrectomy for gastric cancer using a minimally invasive approach. J Gastric Cancer. 2015;15:270–7.
Nunobe S, Hiki N, Tanimura S, Nohara K, Sano T, Yamaguchi T. The clinical safety of performing laparoscopic gastrectomy for gastric cancer by trainees after sufficient experience in assisting. World J Surg. 2013;37:424–9.
Kim MC, Kim W, Kim HH, et al. Risk factors associated with complication following laparoscopy-assisted gastrectomy for gastric cancer: a large-scale Korean multicenter study. Ann Surg Oncol. 2008;15:2692–700.
Fujisaki M, Shinohara T, Hanyu N, et al. Laparoscopic gastrectomy for gastric cancer in the elderly patients. Surg Endosc. 2016;30:1380–7.
Hur H, Xuan Y, Ahn CW, Cho YK, Han SU. Trends and outcomes of minimally invasive surgery for gastric cancer: 750 consecutive cases in seven years at a single center. Am J Surg. 2013;205:45–51.
Lee SE, Kim YW, Lee JH, et al. Developing an institutional protocol guideline for laparoscopy-assisted distal gastrectomy. Ann Surg Oncol. 2009;16:2231–6.
Woo J, Lee JH, Shim KN, Jung HK, Lee HM, Lee HK. Does the difference of invasiveness between totally laparoscopic distal gastrectomy and laparoscopy-assisted distal gastrectomy lead to a difference in early surgical outcomes? A prospective randomized trial. Ann Surg Oncol. 2015;22:1836–43.
Jeong O, Ryu SY, Choi WY, Piao Z, Park YK. Risk factors and learning curve associated with postoperative morbidity of laparoscopic total gastrectomy for gastric carcinoma. Ann Surg Oncol. 2014;21:2994–3001.
Kim HS, Kim SO, Kim BS. Use of a clinical pathway in laparoscopic gastrectomy for gastric cancer. World J Gastroenterol. 2015;21:13507–17.
So JB, Lim ZL, Lin HA, Ti TK. Reduction of hospital stay and cost after the implementation of a clinical pathway for radical gastrectomy for gastric cancer. Gastric Cancer. 2008;11:81–5.
Acknowledgements
Supported in part by Grants from the National Research Foundation of Korea (2012R1A1A1043576 and 2015R1A1A1A05028000) and the Catholic Medical Center Research Foundation made in the program year of 2015.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lee, H.H., Son, SY., Lee, J.H. et al. Surgeon’s Experience Overrides the Effect of Hospital Volume for Postoperative Outcomes of Laparoscopic Surgery in Gastric Cancer: Multi-institutional Study. Ann Surg Oncol 24, 1010–1017 (2017). https://doi.org/10.1245/s10434-016-5672-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5672-7