
Abstract
Background
This study aimed to investigate the short-term surgical outcomes of laparoscopic gastrectomy for gastric cancer in elderly patients in order to determine the safety, feasibility, and risk factors for postoperative complications associated with this procedure.
Methods
We retrospectively investigated 208 patients who underwent laparoscopic gastrectomy for gastric cancer between January 2007 and September 2014. After excluding 15 patients with unusual medical histories or surgical treatments, 193 were selected for this cohort study. We divided the patients into two cohorts: elderly patients (≥75 years old) and non-elderly patients (<74 years old). We compared these cohorts with respect to clinicopathological characteristics and intraoperative and postoperative parameters.
Results
The overall complication rates were 11.4 % (8 of 70 patients) in the elderly cohort and 8.1 % (10 of 123 patients) in the non-elderly cohort (P = 0.449). In a univariate analysis, Charlson comorbidity index (CCI) of ≥3, American Society of Anesthesiologists (ASA) score of 3, operative time of ≥330 min, and intraoperative blood loss of ≥50 ml were found to correlate significantly with postoperative complications. In a multivariate analysis, CCI of ≥3 (P = 0.034), ASA score of 3 (P = 0.019), and intraoperative blood loss of ≥50 ml (P = 0.016) were found to be independent risk factors of postoperative complications. In contrast, age was not found to significantly affect the risk of postoperative complications.
Conclusions
Laparoscopic gastrectomy for gastric cancer can be successfully performed in elderly patients with an acceptable complication rate. This study suggested that high CCI, ASA score, and intraoperative blood loss volume were identified as independent predictors of postoperative complications after laparoscopic gastrectomy for gastric cancer.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Aging of the global population has progressed in recent years. In Japan, 23.3 % of the current population is aged ≥65 years; this percentage is predicted to reach 33 % by 2035 and approximately 40 % by 2060 [1]. The age of patients affected by gastric cancer has also increased rapidly, thus increasing the importance of cancer treatment for these patients. However, elderly patients generally have circulatory and respiratory comorbidities and often suffer from postoperative complications following laparotomy-based procedures.
Since the first report by Kitano et al. [2], laparoscopic distal gastrectomy as a minimally invasive treatment for gastric cancer has rapidly spread throughout Japan and other Eastern countries in recent years. Several multicenter studies have found that this minimally invasive procedure reduces postoperative complications compared with those in laparotomy and specifically reduces the frequency of respiratory complications [3–5]. However, only a few large-scale studies have investigated the efficacy of laparoscopic gastrectomy for gastric cancer in elderly patients. The purpose of this study was to investigate the short-term surgical outcomes of laparoscopic gastrectomy for gastric cancer in elderly patients in order to determine the safety and feasibility of this procedure. In addition, the risk factors for postoperative complications following laparoscopic gastrectomy for gastric cancer were identified.
Materials and methods
Patients
This was a retrospective analysis of a prospectively maintained gastric cancer database in the Department of Surgery at Machida Municipal Hospital, a regional referral hospital in Tokyo, Japan. Between January 2007 and September 2014, 208 patients were diagnosed with gastric cancer and underwent laparoscopic gastrectomy with regional lymph node dissection. Before July 2010, the eligibility criterion for laparoscopic surgery was cT1N0-cT2N0-stage gastric cancer. From July 2010 onward, more advanced cancers were treated via laparoscopic surgery in accordance with our increased familiarity and experience with the procedure.
All patients were subjected to a thorough preoperative assessment with an upper gastrointestinal series and multidetector-row computed tomography. Endoscopic ultrasonography was only performed for staging in patients with suspected T1 tumors. All patients had histologically verified adenocarcinoma of the stomach. Patients who underwent laparoscopic proximal gastrectomy (n = 1) or combined surgery involving another organ (n = 4) for malignant disease were excluded from the present study. Patients who had a history of gastrectomy for concomitant benign and malignant diseases (n = 5) were also excluded from the present study. In addition, patients who underwent palliative gastrectomy (n = 5) because of peritoneal dissemination were excluded from the present study. Finally, 193 patients were selected for this cohort study. We divided the patients into two cohorts: elderly patients (≥75 years old) and non-elderly patients (<74 years old). All patients were treated with gastrectomy according to the Japanese classification of gastric carcinoma (JCGC) by the Japanese Gastric Cancer Association [6].
All laparoscopic gastrectomy operations were performed or guided by two surgeons (T.S., S.K.) who had performed at least 30 laparoscopic gastrectomies for gastric cancer. This study was approved by our institutional review board and included prospective data collection and a retrospective analysis of data obtained from the patients undergoing laparoscopic gastrectomy. All patients and their families were informed of the innovative nature of this study, and written informed consent was obtained before surgery.
Operative technique
Laparoscopic gastrectomy with perigastric lymph node dissection and suprapancreatic lymph node dissection were introduced at our institution in 2002 and 2007, respectively. Beginning in 2007, we began performing laparoscopic gastrectomy in the same manner as open surgical procedures. From July 2010 onwards, we applied a medial approach for suprapancreatic lymph node dissection in all cases [7]. At the beginning of each operation in patients with advanced gastric cancer, the peritoneal cavity was carefully inspected, and a cytological examination via peritoneal lavage was performed to detect macroscopic or microscopic peritoneal dissemination of tumor cells. D1+ or D2 lymph node dissection was performed according to the preoperative study findings.
Until June 2010, reconstruction was performed via extracorporeal anastomosis. From July 2010 onward, all patients underwent laparoscopic gastrectomy with intracorporeal anastomosis. During intracorporeal reconstruction, Roux-en-Y gastrojejunostomy, Billroth II anastomosis with a functional side-to-side anastomosis, or delta-shaped Billroth I anastomosis was performed for patients with distal gastrectomy [8]. Esophagojejunostomy was performed using a functional end-to-end anastomosis or overlap anastomosis in patients with total gastrectomy [9]. For extracorporeal reconstruction, a 5-cm minilaparotomy incision was made in the epigastrium, and a small wound retractor (ALEXIS wound retractor S, Applied Medical, Santa Margarita, CA, USA) was applied for wound protection. Billroth I anastomosis was performed using a circular stapler (Proximate CDH 25, Endosurgery, Cincinnati, OH, USA), whereas Roux-en-Y gastrojejunostomy was conducted using a functional side-to-side anastomosis. In cases of total gastrectomy, Roux-en-Y esophagojejunostomy was performed with a circular stapler and trans-orally inserted anvil (Orvil, Covidien, Mansfield, MA, USA).
Perioperative management
Each patient received standardized pre- and postoperative management. All patients received broad-spectrum antibiotics for 48 h during their postoperative hospitalization. Routine prophylactic somatostatin or octreotide was not used. Oral feeding was initiated after the passage of flatus. Patients were discharged once they were free from complications. Clinicopathological parameters such as age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, and Charlson comorbidity index (CCI) [10], and perioperative data such as operative time, estimated blood loss, presence or absence of postoperative complications, length of postoperative hospital stay, and clinicopathological TNM stage (according to the International Union Against Cancer staging system) [11] were evaluated. Anastomotic stenosis was defined as a condition requiring endoscopic dilatation. Anastomotic leakage was radiologically evaluated using water-soluble contrast material on the third postoperative day. Pancreatic fistula was defined according to the definition proposed by the International Study Group on Pancreatic Fistula [12]. Abdominal abscess was defined as a purulent culture-positive discharge obtained from abdominal drains placed during surgery, or fluid collection requiring drainage. Hospital mortality was defined as death during hospitalization or postoperative death from any cause within 30 days.
Statistical analysis
The Chi-square test was used to compare percentages of events between dichotomous cohorts. Fisher’s exact test was used when a table had a cell with an expected frequency of <5. Patients’ demographics and operative feasibility were compared statistically using an unpaired t test to test equality between the cohorts. For the multivariate analysis, each continuous variable was correlated with the complication rate using Chi-square test to select a cutoff point that maximized statistical significance but preserved clinical utility. Next, all variables with P values < 0.1 in the univariate analysis were entered in the multivariate logistic regression analysis as categorical variables. P values of <0.05 were considered statistically significant. All statistical analyses were performed using Microsoft Excel 2011 software (Microsoft Corporation, Redmond, WA, USA).
Results
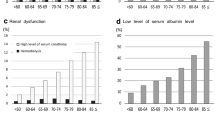
As previously mentioned, we defined elderly patients as those aged ≥75 years (termed “old–old” in Japan). The patients’ characteristics are summarized in Table 1. The mean ages of patients in the elderly and non-elderly cohorts were 80.1 ± 4.1 and 64.8 ± 7.5 years, respectively. An ASA score of 3 was observed more frequently in the elderly cohort. The distribution of tumors according to the TNM classification was similar in the two cohorts [11].
Table 2 presents surgical data of the two cohorts. All patients underwent potentially curative surgery and had resection margins free of invasion. Although the frequency of total gastrectomy was significantly higher in the elderly cohort (P = 0.045), there were no differences between the two cohorts in terms of operative time, intraoperative blood loss, and the degree of lymph node dissection. One patient in the non-elderly cohort required conversion to open surgery and blood transfusion because of an adhesion.
The postoperative variables are shown in Table 3. Complications were classified according to the criteria proposed by Clavien and Dindo, and only those rated grade ≥2 were recorded [13]. The overall complication rates were 11.4 % (8 of 70 patients) in the elderly cohort and 8.1 % (10 of 123 patients) in the non-elderly cohort (P = 0.449). The most common surgical and non-surgical complications were anastomotic stricture (n = 4, 2.1 %) and pneumonia (n = 2, 1.0 %), respectively. There were no significant differences between the two cohorts with regard to the incidence of surgical complications. On the other hand, the number of non-surgical complications was significantly higher in the elderly cohort than that in the non-elderly cohort (P = 0.025). The most frequent non-surgical complication was pneumonia, followed by heart failure and hepatic complication, and the rates of each complication did not differ significantly between the cohorts. Although the time to postoperative oral feeding did not differ significantly between the two cohorts, the mean postoperative hospital stay duration was 2 days longer in the elderly cohort (P = 0.019). Five patients required additional surgery for diaphragmatic hernia (n = 1), abdominal bleeding (n = 1), anastomotic structure (n = 1), small bowel obstruction (n = 1), and anastomotic leakage (n = 1). The reoperation frequency also did not differ significantly between the two cohorts (P = 1.000). One patient in the elderly cohort who underwent reoperation for anastomotic leakage died of severe pneumonia on postoperative day 20.
The results of a univariate analysis to identify the risk factors for postoperative complications are summarized in Table 4. To assess differences in surgeons’ experiences, we also evaluated cases according to the year of operation (early period: January 2007–June 2010; late period: July 2010–September 2014). The incidence rates of postoperative complications in the two cohorts were comparable (11 vs. 8.3 %, P = 0.485). CCI of ≥3 (P = 0.002), ASA score of 3 (P = 0.008), operative time of ≥330 min (P = 0.004), and intraoperative blood loss volume of ≥50 ml (P = 0.006) were significantly related to the incidence of postoperative complications. A multivariate analysis that included these significant factors revealed that CCI of ≥3 (P = 0.034), ASA score of 3 (P = 0.019), and an intraoperative blood loss volume of ≥50 ml (P = 0.016) were independent risk factors for postoperative complications (Table 5).
Discussion
Several previous studies have reported the clinical advantages of laparoscopic distal gastrectomy versus open surgery in non-elderly patients [14–16]. However, the safety and feasibility of laparoscopic gastrectomy, including total gastrectomy, have not been well characterized in elderly patients. Accordingly, the present study was designed to compare the clinical outcomes of laparoscopic gastrectomy for gastric cancer in elderly and non-elderly patients, with a particular focus on postoperative morbidity and mortality. To the best of our knowledge, this is among the largest matched cohort studies to investigate this technique. In the present study, laparoscopic gastrectomy for gastric cancer was found to be safe and feasible in elderly patients. Consequently, we found that patients with CCI of ≥3, ASA score of 3, and intraoperative blood loss volume of ≥50 ml have a greater risk of postoperative complications after laparoscopic gastrectomy for gastric cancer.
Although the frequency of total gastrectomy was significantly higher among elderly patients (P = 0.045), the operative time, intraoperative blood loss volume, and degree of lymph node dissection were similar between the two cohorts, which suggested that the treatments were performed almost identically in elderly and non-elderly patients. No significant differences were observed in the incidence of postoperative complications, which occurred in eight patients (11.4 %) in the elderly cohort and 10 (8.1 %) in the non-elderly cohort (P = 0.449). Previous studies of postoperative complications in elderly patients after laparoscopic gastrectomy for gastric cancer reported incidences rates ranging from 11.5 to 16.8 % [17–20]. Although it was difficult to directly compare our results with those of the previous study, the morbidity observed in our study appeared comparable with that of previous studies from Japan and some specialized Western centers.
Recently, a Korean group reported that laparoscopic gastrectomy was a safe treatment for gastric cancer in elderly patients. The research group concluded that the presence and degree of preoperative comorbidity was an important factor associated with postoperative complications [17, 21]. In the present study, we also performed a multivariate analysis to investigate the risk factors for postoperative complications after laparoscopic gastrectomy for gastric cancer. The present study indicated that CCI of ≥3 and ASA score of 3 were independent risk factors; however, age was not found to be a risk factor. The ASA scoring system is simple and widely accepted as an indicator of a patient’s general condition. However, because of subjective judgment, different anesthesiologists will often assign different scores to the same patient [22]. On the other hand, CCI is widely used for objective quantification of comorbidities. In this index, weighted scores are assigned to 19 conditions, and the inclusion of multiple evaluation conditions renders CCI more objective than the ASA score. In recent years, CCI has been associated with postoperative complications in patients with diseases such as lung cancer and prostate cancer [23, 24]. When performing surgical procedures in elderly patients, eligibility should be determined by placing more emphasis on physical status, organ function, comorbidities, and social background rather than age. We believe that CCI is useful as a prognostic factor for postoperative complications after laparoscopic gastrectomy for gastric cancer.
In the present study, despite the lack of differences in postoperative overall complications between elderly and non-elderly patients, non-surgical complications were more frequent in elderly patients (P = 0.025). This significant difference is thought to result from a difference in the rate of non-surgical complications such as pneumonia and heart failure, which were associated with patient-related factors. The significantly higher ASA score observed in the elderly cohort suggests that decreased physiological organ functioning and physical activity led to the increase in non-surgical complications.
Some reports have indicated an association between surgical experience and postoperative complications following laparoscopic gastrectomy [21, 25]. The advent of new technologies and increasing surgical experience throughout the study period may have influenced the clinical results. Accordingly, we divided the patients into two cohorts according to the year of surgery: early (until 2010 June) and late periods (from 2010 July), to evaluate the relationship between differences in the surgeon’s experience and the incidence of postoperative complications. However, no difference was observed between the cohorts in terms of postoperative complications (11 vs. 8.3 %, P = 0.485). The discrepancy between the results of this and previous studies may have resulted from the following: (1) two surgeons in our study had already performed many laparoscopic gastrectomy operations for gastric cancer and had thus cleared the learning curve, and (2) the same surgical team performed all surgical procedures following the same oncologic and clinical protocols in both cohorts.
In the present study, an intraoperative blood loss volume ≥50 ml was also found to be an independent risk factor associated with postoperative complications, in agreement with a previous study [26]. Moreover, this factor has been reported to associate with the prognosis of many malignant tumors, including gastric cancer [27–29]. Therefore, intraoperative blood loss should be minimized through careful operative technique.
The present study has limitations inherent to its retrospective nature. However, this study demonstrates that elderly patients are not subjected to an increased surgical risk following laparoscopic gastrectomy when compared to non-elderly patients. Further research involving randomized prospective studies is required to establish the safety of laparoscopic gastrectomy for gastric cancer in elderly patients.
References
Okada Y (2013) Emergency medical services in a hyper-aged society. Nihon Rinsho 71:953–963
Kitano S, Iso Y, Moriyama M, Sugimachi K (1994) Laparoscopy-assisted Billroth I gastrectomy. Surg Laparosc Endosc 4:146–148
Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N, Japanese Laparoscopic Surgery Study Group (2007) A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg 245:68–72
Lee JH, Han HS, Lee JH (2005) A prospective randomized study comparing open vs laparoscopy-assisted distal gastrectomy in early gastric cancer: early results. Surg Endosc 19:168–173
Hayashi H, Ochiai T, Shimada H, Gunji Y (2005) Prospective randomized study of open versus laparoscopy-assisted distal gastrectomy with extraperigastric lymph node dissection for early gastric cancer. Surg Endosc 19:1172–1176
Japanese Gastric Cancer Association (2011) Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 14:113–123
Kanaya S, Haruta S, Kawamura Y, Yoshimura F, Inaba K, Hiramatsu Y, Ishida Y, Taniguchi K, Isogaki J, Uyama I (2011) Laparoscopy distinctive technique for suprapancreatic lymph node dissection: medial approach for laparoscopic gastric cancer surgery. Surg Endosc 25:3928–3929
Kanaya S, Gomi T, Momoi H, Tamaki N, Isobe H, Katayama T, Wada Y, Ohtoshi M (2002) Delta-shaped anastomosis in totally laparoscopic Billroth I gastrectomy: new technique of intraabdominal gastroduodenostomy. J Am Coll Surg 195:284–287
Inaba K, Satoh S, Ishida Y, Taniguchi K, Isogaki J, Kanaya S, Uyama I (2010) Overlap method: novel intracorporeal esophagojejunostomy after laparoscopic total gastrectomy. J Am Coll Surg 211:e25–e29
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Sobin LH, Gospodarowicz MK, Wittekind C, International Union against Cancer (2010) TNM classification of malignant tumours, 7th edn. Wiley-Blackwell, Chichester
Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M (2005) Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 138:8–13
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Pugliese R, Maggioni D, Sansonna F, Ferrari GC, Forgione A, Costanzi A, Magistro C, Pauna J, Di Lernia S, Citterio D, Brambilla C (2009) Outcomes and survival after laparoscopic gastrectomy for adenocarcinoma. Analysis on 65 patients operated on by conventional or robot-assisted minimal access procedures. Eur J Surg Oncol 35:28–288
Hwang SI, Kim HO, Yoo CH, Shin JH, Son BH (2009) Laparoscopic-assisted distal gastrectomy versus open distal gastrectomy for advanced gastric cancer. Surg Endosc 23:1252–1258
Francescutti V, Choy I, Biertho L, Goldsmith CH, Anvari M (2009) Gastrectomy and esophagogastrectomy for proximal and distal gastric lesions: a comparison of open and laparoscopic procedures. Surg Innov 16:134–139
Cho GS, Kim W, Kim HH, Ryu SW, Kim MC, Ryu SY (2009) Multicentre study of the safety of laparoscopic subtotal gastrectomy for gastric cancer in the elderly. Br J Surg 96:1437–1442
Kunisaki C, Makino H, Takagawa R, Oshima T, Nagano Y, Ono HA, Akiyama H, Shimada H (2009) Efficacy of laparoscopy-assisted distal gastrectomy for gastric cancer in the elderly. Surg Endosc 23:377–383
Mochiki E, Ohno T, Kamiyama Y, Aihara R, Nakabayashi T, Asao T, Kuwano H (2005) Laparoscopy-assisted gastrectomy for early gastric cancer in young and elderly patients. World J Surg 29:1585–1591
Li H, Han X, Su L, Zhu W, Xu W, Li K, Zhao Q, Yang H, Liu H (2014) Laparoscopic radical gastrectomy versus traditional open surgery in elderly patients with gastric cancer: benefits and complications. Mol Clin Oncol 2:530–534
Kim MC, Kim W, Kim HH, Ryu SW, Ryu SY, Song KY, Lee HJ, Cho GS, Han SU, Hyung WJ, Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) Group (2008) Risk factors associated with complication following laparoscopy-assisted gastrectomy for gastric cancer: a large-scale korean multicenter study. Ann Surg Oncol 15:2692–2700
Haynes SR, Lawler PG (1995) An assessment of the consistency of ASA physical status classification allocation. Anaesthesia 50:195–199
Birim O, Maat AP, Kappetein AP, van Meerbeeck JP, Damhuis RA, Bogers AJ (2003) Validation of the Charlson comorbidity index in patients with operated primary non-small cell lung cancer. Eur J Cardiothorac Surg 23:30–34
Alibhai SM, Leach M, Tomlinson G, Krahn MD, Fleshner N, Holowaty E, Naglie G (2005) 30-day mortality and major complications after radical prostatectomy: influence of age and comorbidity. J Natl Cancer Inst 97:1525–1532
Ryu KW, Kim YW, Lee JH, Nam BH, Kook MC, Choi IJ, Bae JM (2008) Surgical complications and the risk factors of laparoscopy-assisted distal gastrectomy in early gastric cancer. Ann Surg Oncol 15:1625–1631
Jeong O, Ryu SY, Zhao XF, Jung MR, Kim KY, Park YK (2012) Short-term surgical outcomes and operative risks of laparoscopic total gastrectomy (LTG) for gastric carcinoma: experience at a large-volume center. Surg Endosc 26:3418–3425
Mörner ME, Gunnarsson U, Jestin P, Svanfeldt M (2012) The importance of blood loss during colon cancer surgery for long-term survival: an epidemiological study based on a population based register. Ann Surg 255:1126–1128
Nagai S, Fujii T, Kodera Y, Kanda M, Sahin TT, Kanzaki A, Yamada S, Sugimoto H, Nomoto S, Takeda S, Morita S, Nakao A (2011) Impact of operative blood loss on survival in invasive ductal adenocarcinoma of the pancreas. Pancreas 40:3–9
Liang YX, Guo HH, Deng JY, Wang BG, Ding XW, Wang XN, Zhang L, Liang H (2013) Impact of intraoperative blood loss on survival after curative resection for gastric cancer. World J Gastroenterol 19:5542–5550
Disclosures
M. Fujisaki, T. Shinohara, N. Hanyu, S. Kawano, Y. Tanaka, A. Watanabe, and K. Yanaga have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s00464-016-5334-7.
Rights and permissions
About this article

Cite this article
Fujisaki, M., Shinohara, T., Hanyu, N. et al. Laparoscopic gastrectomy for gastric cancer in the elderly patients. Surg Endosc 30, 1380–1387 (2016). https://doi.org/10.1007/s00464-015-4340-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4340-5