
Abstract
Background
Anterior cruciate ligament (ACL) injury increases risk for post traumatic knee osteoarthritis. ACL injury causes lack of knee stability and frequently requires ACL-reconstruction (ACLR) in order to restore functional and anatomical joint stability. Magnetic resonance imaging with T2 mapping sequence is used to quantify the amount of water content in articular cartilage hence; it is considered a better tool and more beneficial than radiographic based assessment in early detection even before being symptomatic. The aim of work is to estimate the incidence of subclinical degenerative changes that happened early in patients who underwent ACL reconstruction and to identify the correlations of T2 mapping values with patients' BMI, meniscal state/operations, ACL graft assessment and presence of ACLR related complications.
Results
The study was conducted upon 71 patients, divided into 61 anterior cruciate ligament reconstructed knees and 10 control cases using 1.5 T MRI. Assessment of cartilage sub-compartment T2 values and comparison with average normal cartilage T2 values obtained from the control group. Multiple correlations of the grade of articular cartilage degeneration within anterior cruciate ligament reconstructed knees with Body Mass Index (BMI), time of operation as well associated meniscal operations and anterior cruciate ligament graft complications.
Conclusions
Adding the T2 cartilage mapping sequence improves the ability to detect subclinical early degenerative articular cartilage changes in patients who underwent anterior cruciate ligament reconstruction, taking into consideration the relation of the patients' BMI, previous meniscal injuries/operation, ACL graft status and related graft complications with the T2 cartilage mapping values.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
The anterior cruciate ligament (ACL) is that the most ordinarily injured knee ligament accounting for half all knee injuries. Within the United States, The incidence of ACL ruptures is between 100,000 and 200,000 individuals per annum, with an annual incidence within the general population of roughly 1 in 3500, although the particular incidence could also be higher [1].
The anterior cruciate ligament is considered a primary mechanical stabilizer that stops excessive anterior tibial translation and contributes to lateral and rotational knee stability. ACL injury causes lack of knee stability and regularly requires ACL-reconstruction (ACLR) to revive functional and anatomical joint stability [2].
Divergent the knee mechanics and loading patterns are responsible for the articular cartilage disintegration, despite the knee reconstruction operations. ACLR has been shown to quicken cartilage degeneration and stimulate knee post-traumatic osteoarthritis (PTOA) [3].
Previous reports regarding the high incidence of osteoarthritis (OA) for knees with ACL reconstruction surgeries were performed for quite 15 years. Recent surgical advanced techniques could enhance the steadiness and kinematics of knees post ACL reconstruction. Therefore, the incidence of OA after modern ACL reconstruction is also under what has been reported within the literature [4].
The use of those quantitative MRI techniques, including T1ρ and T2 mapping, allows for earlier identification of knee cartilage degeneration after ACLR before the appearance of any symptoms and significant radiographic changes. T1ρ and T2 mapping sequences are related with the biochemical composition of cartilage matrix by counting the number of proteoglycans, water, and collagen inside the matrix when put next to structural changes evaluated with radiography and standard MRI [5].
There is an association exist between altered knee biomechanics and quantitative resonance imaging (QMRI) articular cartilage findings supported altered knee joint biomechanics in ACLR patients are related to abnormal changes of knee articular cartilage composition that results in premature occurrence of knee OA onset or rapid progression of the disease process [6].
The use of MR-based techniques like QMRI (i.e., T2 mapping) of knee PTOA, rather than radiographic based assessments, appears to be more beneficial and informative in understanding the potential links between knee joint mechanics after ACLR and knee joint pathologies, even before being symptomatic [6].
T1ρ mapping is indicative of proteoglycans content and more sensitive to cartilage integrity, as critical T2 mapping, which is more prone to water content and will not be able to differentiate between edema and matrix degradation so, T1p mapping can be more sensitive in detecting early cartilage damage, compared to other QMRI techniques like T2 mapping [6].
Immediate surgical intervention after anterior cruciate ligament injury is crucially important in prevention of any further cartilage degeneration. Many patients undergo surgical reconstruction of ACL to restore joint stability and prevent excessive loading. However, convincing evidence is still lacking for the superiority of ACL- reconstruction to conservative management in term of the incidence of PTOA. The development of conservative, physical, and pharmacological treatments leads to delay the onset of PTOA and optimal long-term health after ACLR [7].
Methods
Study population
A prospective study conducted over two years that included 71 patients, divided into 61 cases underwent anterior cruciate ligament reconstruction and 10 control cases. The control cases' age where relatively within the same age group of the cases and demonstrate relatively the same patients' gender.
Inclusion criteria
All included patients underwent anterior cruciate ligament reconstruction since 6 months or more, no radiographic osteoarthritic changes before surgery(detected through clinical data as well CT or x ray done prior operations to exclude associated fractures or deformities), no sex predilection and age above 20 years. The control group inclusion criteria were clinically normal individuals with no knee symptoms.
Exclusion criteria
Patients underwent anterior cruciate ligament more than 10 years, known patients with autoimmune diseases may lead to osteoarthropathy, old patients with X-ray findings of OA and patients with contraindications for MRI examinations, e.g. pacemakers and aneurysm clips.
Demographic and clinical data were obtained from the patients underwent anterior cruciate ligament reconstruction regarding the affected knee side, BMI, time of operation as well associated meniscal operations.
We used a MRI scanner (1.5 Tesla, Signa; GE Healthcare, USA). Routine MRI sequences included axial T2-weighted images (3000/87 ms, duration 2 min 19 s), sagittal T1-weighted images (435/10 ms, duration 2 min 55 s), sagittal T2–WI (repetition time/echo time, 3000/81 ms, duration 2 min 58 s), sagittal proton density-WI with fat saturation (2440/40 ms, duration 2 min 38 s) and coronal STIR weighted images (400/8 ms, duration 2 min 24 s), using a knee coil with field of view, 10 × 10 mm; matrix, 320 × 224; slice gap, 4 mm and slice thickness, 4 mm.
Three sagittal data sets were obtained to get T2 mapping sequence by applying FSE with a repetition time of 1000 and eight echo times as follows (8.4 ms, 16.8 ms, 25.2 ms, 33.5 ms, 41.9 ms, 50.3 ms, 58.7 ms, and 67.1 ms). Matrix, 256 × 256; FOV 90–130 mm; slice gap, 3.5 mm; slice thickness, 3 mm.
Knee magnetic resonance examination was performed post reconstruction operation with established post-processing images were obtained; images acquired were evaluated for the color cartilage map and were analyzed within each ROI (Regions Of Interest).
The T2 mapping sequence total acquisition time was 4–7 min. By using the default software settings and functions, a processed T2 colour map was built. The default parameters of the T2 intensity are 11–89 ms, with a calculated cut-off point of 50 ms. the colour scale varies from red to blue colour scale in which green or blue colour representing high T2 values on the colour-coded scale on a minimum of two consecutive slices. The acquired MR images of T2 mapping sequence then sent to a workstation where an off-line quantification of T2 values and cartilage thickness were evaluated in every case.
An elliptical ROI was put with a margin of 0.5 to 1 mm from the bone surface to prevent sub-chondral bone inclusion. Standard knee MRI and post-processing T2 mapping images were visualized conjointly side by side, using a multi-planar localization key on the PACS.
The knee articular cartilage was fractionated into four compartments as follows: lateral femoral condyle (LFC), medial femoral condyle (MFC), lateral tibia (LT) and medial tibia (MT). Femoral cartilage regions of interest (ROIs) were partitioned into three segments. From the center circle marking the approximate circumference of each posterior femoral condyle, a line parallel to the distal femoral axis was drawn.
Segments on either side of the line parallel to the femoral axis defined as follows: the anterior segment 45° from the line (MFC1, LFC1), the middle segment 45° posterior of the line (MFC2, LFC2), and the posterior segment was oriented 45° to 90° posterior of the line (MFC3, LFC3). ROIs on the tibial cartilage behaved into anterior (MT1, LT1) and posterior compartments (MT2, LT2) (Fig. 1).

Compartmentalization according to the whole organ magnetic resonance imaging score (WORMS) of the knee in osteoarthritis. Each region of interest (ROI) was defined as follows: ROIs on the femoral articular cartilage were divided into an anterior area 45° from the line (MFC1, LFC1), a middle area 45° posterior from the line (MFC2, LFC2), and a posterior area 45° to 90° posterior from the line (MFC3, LFC3). ROIs on the tibial articular cartilage were divided into an anterior (MT1, LT1) and posterior area (MT2, LT2). Left: medial compartment. Right: lateral compartment. MFC medial femoral condyle, MT medial tibia, LFC lateral femoral condyle, LT lateral tibia (Quoted from Proffen et al. [35])
Evaluation of the cartilage degeneration based upon appearance including the MR signal and cartilage thickness within the conventional images and T2 mapping images with detection of the affected cartilage compartment and grade of cartilage injury using MRI outerbridge classification for cartilage degeneration modified by Potter et al. [8, 9].
The included studies will be independently interpreted by a musculoskeletal radiologist with 10 + years of experience and by a musculoskeletal radiologist with 5 + years experience, therefore the images will be reviewed by two different readers all blinded to the patient’s clinical history and clinical findings. Inter-reader agreement was determined using the weighted kappa (к) statistic with к value ≥ 0.8 indicating good agreement.
Statistical analyses
The clustered data was edited, encoded, tabulated and introduced to a PC using Statistical package for science (SPSS 23). Data was presented and suitable analysis was done in step with the kind of knowledge obtained for every parameter. Mean, variance (± SD) and range for parametric numerical data, while Median and Inter-quartile range (IQR) for non-parametric numerical data. Frequency and percentage of non-numerical data were additionally included.
The following tests were done: chi-square (× 2) test of significance utilized in order to match proportions between qualitative parameters, the arrogance interval was set to 95% and therefore the margin of error accepted was set to five. So, the p-value was considered significant because the following: Probability (P value): P value < 0.05 was considered significant, P value < 0.001 was considered as highly significant and P value > 0.05 was considered insignificant.
Results
The total number of patients were 71 where 10 control (8 male patients and 2 female patients) cases and 61 cases with unilateral ACL-reconstruction, 53 male patients and 8 female patients with their ages ranging from 27 to 45 year old with a mean age 33.3 ± 7.9 (mean ± SD) and mean BMI of the involved patients shows 28 ± 3.28, 12 out of 71 patients were found within the normal range of body weights and BMI, 34 out of 71 patients were overweight and 15 patients were obese (Table 1).
The cases show predominance of ACL reconstruction operation on the right side more than the left side with ratio of 63% of the cases, and the range of follow-up duration period post ACL reconstruction operation of the involved cases from 2 to 8 years. Concomitant operations such as medial meniscectomy were found within 33 cases and of SD 44.3%.
The patients mostly presented with combined symptoms: 18 cases (29.5%) presented with knee swelling (within average duration of 3 years), 55 cases (90%) presented with knee pain (within average duration of 5 years), 16 cases (26.2%) presented with recent trauma/twisting to the operated knee joint, 12 cases (19.7%) presented with limitation of the knee joint movement and joint instability (show variable duration, some patients presented 2 years following reconstruction and few presented 6 years post ACLR).
The cases with ACL reconstruction/control study of 61/10 subjects respectively showed significantly (p < 0.05) increases in T2 times values between diseased (42.0–60 ms) and control uninjured (30.1–39.8 ms) knees respectively.
Cases were categorized according to the combined conventional MRI and post processing T2 mapping with grading of the cartilage abnormality according to International cartilage Repair Society (ICRS) grading system.
-
Out of the 61 cases, 8 (13.1%) cases were diagnosed of having no abnormality on conventional images or alteration of cartilage composition, grade 0
-
Out of the 61 cases, 10 (16.3%) cases were found having no abnormality on conventional images with increased T2 value on T2 mapping cartilage mapping image, in keeping with grade I.
-
Out of the 61 cases, 37 (60.6%) cases were diagnosed of having superficial ulceration of the articular cartilage on conventional images with increased T2 value, in keeping with grade II.
-
Out of the 61 cases, 6 (10%) cases were diagnosed of having deep ulceration of the articular cartilage on conventional images with increased T2 value, in keeping with grade III.
-
Ten over eighteen cases were misdiagnosed of being normal on conventional MR images, while having alteration of cartilage composition of early osteoarthritis, discovered by T2 mapping sequence.
Degeneration and different parameters
Severity of degeneration and duration since ACL reconstruction: this study showed a reciprocal relation between the grade of cartilage degeneration and duration since ACL reconstruction operation. Meaning that; higher grades of degeneration were reported among patients who had the operation done 5–8 years ago compared to those who had their operation done 2–5 years, 38 cases had their operations performed 2–5 years ago, the majority of which were found to have grade I degeneration (20/40: 55%), 6/40 cases were found to have grade II degeneration (15%), 8/40 were found to have grade 0 degeneration(20%), and only 4/40 cases were found to have grade III degeneration (10%) and on the other hand, 23 cases had their operations performed more than 5 years ago, 15/21 had grade II degeneration (61.9%) and only 8/21 patients had grade III degeneration (38.1%) (Fig. 2, Table 2).

Diagrammatic demonstration of the degree of cartilage degeneration and duration since ACL reconstruction
Severity of degeneration and BMI: the grade of cartilage degeneration is directly proportionate to BMI of the cases. Meaning that higher grades of cartilage degeneration were found among patients with higher BMI achieving a statistically significant correlation; p value (0.001), 12 patients were found to have normal BMI values: 8 of which had grade 0 degeneration, while 4 had grade I degeneration, 34 patients were found to have overweight BMI values. 14 of them had grade I cartilage degeneration, while 8 had grade II degeneration and only 2 had grade III degeneration. However, 15 patients had obese BMI values, 2 of them had grade I degeneration, 13 had grade II degeneration while 10 had grade III degeneration and The following table shows that more patients with grade III were found among obese patients compared to overweight and normal weight patients (Fig. 3, Table 2).

Diagrammatic demonstration of the degree of cartilage degeneration and patients' body weights
Severity of degeneration and history of meniscectomy: 33 out of the included 61 patients in our study had history of meniscectomy operation before/after or during ACL reconstruction operation. A reciprocal relation was found between grade of cartilage degeneration and history of previous medial meniscectomy. Meaning that; Grade III degeneration was more frequently reported among patients who performed meniscectomy compared to those who didn't perform it (10 compared to 2 patients respectively). Grade II degeneration was more frequently reported among patients who had previous meniscectomy compared to those who did not (15 patients compared to 6 respectively) however, Grade I degeneration was equally reported between both patient groups (10 patients each) (Fig. 4, Table 2).

Diagrammatic demonstration of the degree of cartilage degeneration and history of meniscectomy.
Severity of degeneration and conventional MR appearance of the cartilage: abnormal cartilage appearance was reported among 27 patients; however abnormal signal reported among 43 patients. A significant correlation was found between abnormal signal/appearance and grade of cartilage degeneration achieving p value of about 0.001, grade III was more frequently reported among cartilages with abnormal appearance/signal compared to normal cartilages (6 patients compared to 0 patients respectively), however, lower grades of cartilage degeneration were more frequently reported among normally appearing cartilages compared to abnormal looking ones: (8 compared to 0 patients for Grade 0, 3 compared to 7 patients for grade I and 37 compared to 0 patients for grade II respectively) and as regards abnormal cartilage signal intensity, only grades II and III were more frequently reported among cartilages with abnormal SI compared to those with normal SI: (30 compared to 7 for Grade II and 6 compared to 0 for grade III) respectively (Fig. 5, Table 3).

Diagrammatic demonstration of the degree of cartilage degeneration and conventional MR appearance of the cartilage
Severity of degeneration and post-operative complications related to ACL reconstruction: only11/61 patients in our study showed complications related to ACL reconstruction operation. While the rest of the patients didn’t show any radiological evidence of operation related complications. A statistically significant correlation was found between severity of post ACL-reconstruction complications and grade of cartilage degeneration achieving a p value of about 0.001 and patients who had cyclop lesions or altered signal denoting edema showed grade III degeneration. While those with interstitial tear of the ACL graft had grade II degeneration, and those with tibial cyst/tear of the tibial insertion had grade I degeneration (Table 2).
Discussion
Identification of early cartilage degeneration in routine magnetic resonance (MR) imaging is crucially beneficial in joints imaging. Thus, combining the morphological and functional information of the articular cartilage which adds a tremendous ability to detect early degenerative changes and help to distinguish the different degenerative stages [10].
In this study, the T2 mapping sequence was used to evaluate the early compositional changes of articular cartilage in patients post ACL reconstruction operations. Many criteria are available to assess the knee cartilage morphology with estimation of the incidence of early subclinical degenerative changes and identification the relation of differences in T2 mapping values with surgical factors and clinical outcomes (Figs. 6, 7, 8, 9, 10).

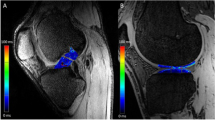
A 40-year-old male patient underwent ACL reconstruction and medial meniscectomy 4.5 years ago, the patient complained of knee pain and swelling. In assessment of the MRI knee, the conventional images shows evidence of medial meniscectomy and mild knee joint effusion with taut signal of the ACL graft. Sagittal T2 image A along the medial femoral condyle anterior segment shows partial thinning of the articular cartilage. On the post processing T2 mapping image: (C, D) the colour image along the articular cartilage of the medial femoral condyle anterior segment revealed internal areas of blue colour (yellow ROI) with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade II cartilage degeneration. Coronal (E) and focused sagittal STIR image upon the medial meniscus level (e), attenuated body and posterior horn of medial meniscus show intrasubstance heterogeneous band of increased signals reaching the articular surfaces, denoting meniscal re-tear (Thick white arrow/white dashed circle). Note the patchy bone marrow edema signal STIR signal (White arrow)

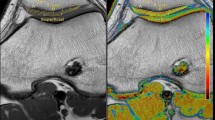
A 32-year-old male patient underwent ACL reconstruction and medial meniscectomy 6 years ago, the patient complained of knee pain and swelling. In assessment of the MRI knee, the conventional images shows evidence of medial meniscectomy and mild knee joint effusion with interstitial tearing of the ACL graft. Sagittal T2 image (A) along the medial femoral condyle posterior segment shows mild thinning of the articular cartilage. On the post processing T2 mapping image: (C, D) The colour image along the articular cartilage of the medial femoral condyle posterior segment revealed internal areas of faint blue colour within the deep layer (red arrows) with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade II cartilage degeneration. Sagittal STIR image (E) at intercondylar notch level revealed intra-substance linear streaks of bright signals within the anterior cruciate ligament graft that goes with interstitial tear (White arrows)

A 24-year-old male patient underwent ACL reconstruction 3 years ago, the patient complained of knee pain and swelling. In assessment of the MRI knee, the conventional images shows and mild knee joint effusion. Intact ACL graft showing normal position and taut signal, no evidence of tearing or related complications. Sagittal T2 image (A) along the medial femoral condyle level shows intact articular cartilage upon the posterior segment with subtle intrasubstance high signals (Arrow). On the post processing T2 mapping image; (C, D) The colour image along the articular cartilage of the medial femoral condyle posterior segment revealed internal areas of blue colour within the deep layer (white arrows) with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade I cartilage degeneration. Sagittal T2 image (A) at lateral femoro-tibial articulation level shows intact articular cartilage overlying the posterior segment of the lateral tibial condyle with intrasubstance high signal. On the post processing colour coded T2 mapping image: (C, D) The colour images along the articular cartilage of the lateral tibial condyle posterior segment revealed internal focal area of green colour (arrows) with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade I cartilage degeneration

A 34-year-old male patient underwent ACL reconstruction and medial meniscectomy 8 years ago, the patient complained of knee pain and swelling. In assessment of the MRI knee, the conventional images show ACL graft buckling and thickening, medial meniscal tear and mild knee joint effusion. Sagittal T2 image (A) at lateral femoral condyle level shows thickening of the articular cartilage upon the lateral femoral condyle anterior segment. On the post processing T2 mapping image: (C, D) The colour image along the articular cartilage of the lateral femoral condyle anterior segment revealed internal areas of blue colour (Yellow ROI) within the deep part with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade I cartilage degeneration. Sagittal STIR image (E) at the intercondylar notch level shows relative anterior position and vertical orientation of the tibial tunnel is noted. Mild thickening and buckling of the anterior cruciate ligament graft with intrinsic high signals, yet no evidence of fiber disruption. Findings suggestive of ACL graft roof impingement (White arrows). Coronal (F) and focused sagittal STIR image upon the medial meniscus level(f), the body and posterior horn of medial meniscus show intra-substance linear band of bright signals reaching the menisco-capsular attachment and abutting the inferior articular surface, corresponds to meniscal tear (White arrows). Note the patchy bone marrow edema signals surrounding the tibial tunnel, displaying high STIR signals (Yellow arrow)

A 27-year-old male patient underwent ACL reconstruction 3 years ago, the patient complained of knee pain and swelling. In assessment of the MRI knee, the conventional images shows mild knee joint effusion with intact ACL graft. Sagittal T2 image (A) at lateral femoral condyle level shows mild thinning of the articular cartilage upon the lateral femoral condyle posterior and middle segments (White arrows). On the post processing colour coded T2 mapping image: (C, D) The colour image along the articular cartilage of the lateral femoral condyle posterior and middle segments shows intrasubstance linear areas of blue colour with increased T2 value (as demonstrated within the curve image (B)) that corresponds to articular cartilage degeneration. According to the international cartilage Repair Society (ICRS) grading system, this corresponds to grade II cartilage
Regarding gender, there was no significant difference of either males or females patients T2 values post ACL reconstruction surgeries which showed an agreement with Mosher et al. [11] study at which compared the differences in T2 cartilage mapping values between uninjured cartilage in men and women groups and found no significant values differences between gender. Also, Çağlar et al. [12] study found no statistically significant difference in the cartilage T2 relaxation times in the involved subgroups whatever the patients' gender [11, 12].
Regarding age, our study showed no significant positive correlation between age and T2 values that agreed with Çağlar et al. [12] study, that revealed the consequential T2 values elevations correlated with age in ACL reconstructed patients and control groups.
Regarding BMI, our study revealed that the grade of cartilage degeneration was directly proportionate to BMI of the patients underwent ACLR. Meaning that higher grades of cartilage degeneration were found among ACLR knees with higher BMI achieving a statistically significant correlation; p value (0.001).
This showed an agreement with Culvenor et al. [13] revealing that the relation of the high BMI and ACL reconstruction operations may advance cartilage degeneration compared to normal BMI patients with ACL reconstruction, meaning increased BMI of the patients than normal average values was considered a strong determinant in knee joint state deterioration following ACL reconstruction. These worsening early osteoarthritic features on MRI that result into progressive disease pathway, ending with well established post-traumatic osteoarthritis.
Most of the cartilage degeneration was found in the weight-bearing regions within the medial and the lateral compartments of the ACL-reconstructed knees with overall increase in T2 values in the medial femoral condyle (MFC) and the lateral tibial condyle (LTC). Previous studies founded that escalated articular cartilage T1ρ or T2 values at up to 2 years post ACL reconstruction occurred even if the graft is intact with taut appearance on MRI sequences and clinically successful, this shows an agreement with [14,15,16,17,18,19,20].
Theologis et al. [20] found that escalated T1ρ values in ACL-reconstructed knees at the articular cartilage overlying the medial femoral condyle (MFC) and medial tibia (MT) in follow-up MRI relative to the opposite uninjured knees.
The results of our study supported the potential ability of T2 cartilage mapping in detecting subtle structural cartilage abnormalities that appear normal on conventional MRI. The high values at T2 mapping and cartilage degeneration have shown a correlation. However, no results have been reported on the threshold T2 values that indicate neither cartilage degradation nor even the degree of cartilage affection [21, 22].
We found heterogeneous increases in T2 values in the ACL reconstructed knees relative to the control uninjured knees during the follow-up. The cases with ACL reconstruction/control study of 61/10 subjects respectively showed significantly (p < 0.05) increases in T2 times values between diseased (42.0–60 ms) and control uninjured (30.1–39.8 ms) knees respectively.
These findings agreed with Liebl et al. [22] who suggested, in a case–control study using 130 subjects that knees with incident tibiofemoral osteoarthritis had significantly higher mean T2 values in each compartment compared with controls.
Van Ginkel et al. [18] showed that T2 values for the medial femoral cartilage of ACL-reconstructed knees were higher than those for normal controls with values (45 ms vs. 37 ms). Different MR acquisition methods and physiological variations between subjects may give different measurements of T2 values, so these data should only be used as a reference.
Isolated ACL injury can lead to the occurrence of knee OA regardless the patients underwent ACL reconstruction or conservative treatment. Previous established results showed that knee OA occurrence following ACL reconstruction showed a 57% incidence in contrary to an 18% incidence of knee OA occurrence in the opposite uninjured knee [23].
In a 2014 meta-analysis, with a relative risk (RR) of 3.84 (P < 0.0004), the radiograph signs revealed moderate to severe osteoarthritis with (20.3%) of ruptured ACL knees with moderate or severe radiologic changes compared to (4.9%) of uninjured knees. In ACL injured patients who choose conservative treatment had a significantly higher RR (RR, 4.98; P < 0.00001) of establishing osteoarthritic changes in contrast to those underwent ACL reconstruction surgery (RR, 3.62; P < 0.00001) [24].
In a more recent meta-analysis, the prevalence of knee osteoarthritis radiography was 11.3% (6.4–19.1%), 20.6% (14.9–27.7%), and 51.6% (29.1–73.5%), following ACL reconstruction at 5, 10, and 20 years after surgery respectively [25].
Previous kinematic reaches have reported substantially altered tibio-femoral motion, leading to abnormal shift and loading pattern upon the cartilage regions. These results suggested abnormal kinematics mainly within the medial compartments of ACL-injured knees that may lead to articular cartilage impairment. Also, it is likely that concomitant other intra-articular injury, such as meniscal tears or chondral injury, will have acted as confounders. Previous studies have suggested that intact menisci are critical and major factor to prevent articular cartilage degeneration within ACL reconstructed knees [26, 27].
Titchenal et al. [28] that reported a recent pilot study in 9 patients evaluated 1.5 years after ACLR revealed positive relation of elevated T2 relaxation times in ACL-reconstructed knees and higher knee adduction motion during walking and mechanical mal-alignment. Early repairable subsurface cartilage changes following ACL reconstruction were perceived using quantitative ultra-short echo time enhanced T2* mapping with settled OA risk such as knee adduction motion (KAM) and mechanical alignment.
According to the results of our study, it showed strong agreement with Ushio et al. [29] that found an escalation in T1ρ values in the medial compartment likely to occur with ACL reconstruction. Significant increase in T1ρ values were observed in also (LFC1, and LT1). In contrast, T1ρ values in the posterolateral femoral condyle and tibial plateau (LFC3 and LT2) goes down [18, 29, 30].
In parallel, Li et al. [17] another study upon ACL-injured knees, found raised T1ρ and T2 values in articular cartilage of medial femoral condyle and lateral tibial plateau within the central regions (MFC2 and LT2).
Regarding the grade of cartilage degeneration and history of previous medial meniscectomy, a reciprocal relation was established in our study. Meaning that high grades of cartilage degeneration were more frequently reported among patients who perform meniscectomy compared to people who did not perform. Such finding showed an agreement with a lot of clinical studies had shown that the status of the meniscus is one of the important risk factors for development of OA after ACL reconstruction [25, 31, 32]. Some studies have found higher T1ρ or T2 values in ACL-reconstructed knees with a torn meniscus relative to the healthy knees [17, 18, 20].
In the setting of ACL injury, the status of the meniscus and the cartilage plays a major role in the occurrence of knee OA. Time elapsed between injury and the reconstruction operation is considered further significant factors for development of osteoarthritis (OA). Øiestadet et al. [32] had found that 80% of patients with combined ACL and meniscus injuries developed knee osteoarthritis at 10–15 years following reconstruction operations more and faster as compared to 62% with isolated ACL injury.
This goes with study of Salmon et al. [31] that found patients who had undergone combined meniscectomy and ACL reconstruction had increased incidence of graft laxity on the long term with greater odds of graft complications such as rupture, possibly reflecting the impact of repetitive chronic strain upon the reconstructed graft.
On the contrary, it showed no agreement with Patterson et al. [33] who demonstrated no significant effect on cartilage degeneration was found where all patients included received partial meniscal resection during primary ACL reconstruction operation.
Also, our results showed agreement with Hirose et al. [16] reported that the T1ρ values of the medial femoral condyle, medial tibial and lateral femoral condyle increased during the first year following ACL reconstruction, regardless of the status of the meniscal being injured or not.
In the medial compartment, articular cartilage was remarkably thicker in weight-bearing regions of the femoral condyle in ACL-injured knees compared with control knees over two years. The thickest segments of cartilage occur where the cartilage-on-cartilage contact and presumably occur as a response to loading [17].
Cartilage remodelling in hypertrophy was obvious in ACLR knees, starting from 2.5 years till 4.5 years following surgery the form of tibial cartilage. This was partially relying upon meniscal state and the nature of the underlying bone and cartilage pathologies present at baseline data at time of trauma [10].
Cartilage swelling within the medial tibio-femoral compartment has also been reported in patients with minimal severity of radiographic OA. In conjunction with increased T1ρ values of the weight-bearing medial tibio-femoral cartilage, these results suggest early cartilage degeneration in the form of increase of water content, decrease of proteoglycans, and cartilage swelling [17].
The main factor for development of cartilage degeneration has no direct relation to the timing of ACL reconstruction operation but mainly influenced by time passing since the injury to ACL and time of reconstruction operation as well the presence of medial meniscal tears, medial femoral condyle chondral damage, and presence of degenerative changes at the surgery time [33].
In our study a reciprocal relation between the grade of cartilage degeneration and duration since ACL reconstruction operation was found. Meaning that; higher grades of degeneration were reported among patients who had the operation done 5–8 years compared to those who had their operation done 2–5 years ago.
This showed an agreement with the study of André et al. [34] that revealed direct relation between the grade of cartilage degeneration and duration since ACL reconstruction operation with a significant increase in cartilage degeneration at a mean 46-month duration following ACL reconstruction with occurrence of related ACL graft complications.
These findings differed from another cohort study findings established by Harris et al. [35] that showed higher proportion of tibio-femoral osteoarthritic changes occur as early ACL reconstruction changes with a ratio of (16 vs. 7%) compared to delayed ACL reconstruction changes.
ACL reconstruction operations prevent knee osteoarthritis is considered to be a common misperception. Though ACL reconstruction does not prevent the eventual development of knee osteoarthritis, Mihelic et al. [23] suggested that it can delay its onset. In contrast to other studies which have found a strong evidence of knee OA following ACL reconstruction compared to patients with chronic ACL tears treated conservatively [34].
Mihelic et al. [23] found that patients treated conservatively had unstable knee joints with more anterior translation and higher standard of severe degeneration, also the reconstruction of ACL cannot prevent OA. In addition, there was a crucial prevalence of severe OA (P < 0.5) in the reconstructed group with concomitant meniscal lesions.
Not only the ACL reconstruction operations delay the occurrence of knee osteoarthritic changes, but also decrease other associated injuries to the meniscus and knee ligaments. In reviewing a cohort study of patients with ACL injuries treated conservatively, Chalmers et al. [36] found that ACL reconstructed patients had an around twofold decrease the need for secondary operation of meniscal surgery as compared to non-operated patients.
In brief, the following chart demonstrates collectively the possible risk factors found to accelerate the degenerative changes in patients underwent anterior cruciate ligament reconstruction (Fig. 11).

Demonstrative mechanisms for development of PTOA in ACLR knees
This study had several obstacles. Our ability to characterize possible T2 mapping changes post ACLR was limited by small sample size.
Secondly, we had no preoperative or baseline data at time of trauma on the articular cartilage and presence of bone contusion or osteochondral injury. Additionally, there were no long term follow up for the included patients. We investigated the T2 values for articular cartilage at only one time point.
Thirdly, T2 mapping is vulnerable to the magic angle effect; therefore, we avert the assessment of cartilage oriented at 55° to the main magnetic field.
Lastly, the patello-femoral joint was not included in our study despite many studies reported worsening osteoarthritis post ACL reconstruction.
Conclusions
In conclusion, we observed high rates of knee articular cartilage degenerative changes on patients underwent anterior cruciate ligament reconstruction, with higher rates in patients with concomitant meniscectomy at operative time, osteochondral injury, bone contusion, or meniscal tear.
Compositional MR imaging and special cartilage T2 mapping sequence is superior to the conventional MR in early detection of cartilage degenerative changes. The capability to recognize early potentially reversible cartilage changes advance to breakdown of the articular surface is the main key factor to prevent osteoarthritis and develop methods through effective application of early treatment strategies to those with articular cartilage “at risk.” The articular cartilage has not shown a capacity to heal compromising the articular surface; while it may show ability to restore subsurface matrix changes.
Early detection of cartilage degeneration following ACL reconstruction in young patients allows timely management, hence better quality of life.
Recommendations
No available results upon the specific threshold increases in T2 values that reflect cartilage degeneration. Previous studies have found that normal controls have between 3 and 12% lower T2 values. Further studies are needed to establish the T2 values threshold.
In future studies, standardized criteria should be developed to determine whether a patient needs to receive conservative treatment or surgery reconstruction, which may reduce the financial burden on the health care system and prolong joint health.
Availability of data and materials
The data and material used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ACLR:
-
Anterior cruciate ligament reconstruction
- FOV:
-
Field of view
- RR:
-
Relative risk
- IQR:
-
Inter-quartile range
- KAM:
-
Knee adduction moment
- LFC:
-
Lateral femoral condyle
- LT:
-
Lateral tibia
- LTC:
-
Lateral tibial condyle
- MFC:
-
Medial femoral condyle
- MR:
-
Magnetic resonance
- MT:
-
Medial tibia
- OA:
-
Osteoarthritis
- PTOA:
-
Post traumatic osteoarthritis
- QMRI:
-
Quantitative magnetic resonance imaging
- ROI:
-
Region of interest
- SD:
-
Standard deviation
- STIR:
-
Short tau inversion recovery
- UTE-T2*:
-
Ultra-short echo time enhanced T2*
- WORMS:
-
Whole organ magnetic resonance imaging score
References
Musahl V, Karlsson T (2019) Anterior cruciate ligament tear. N Engl J Med 380(24):2341
Sanders TL, MaraditKremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA, Stuart MJ, Krych AJ (2016) Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med 44(6):1502–1507
Li RT, Lorenz S, Xu Y, Harner CD, Fu FH, Irrgang JJ (2011) Predictors of radiographic knee osteoarthritis after anterior cruciate ligament reconstruction. Am J Sports Med 39(12):2595–2603
Spindler KP, Huston LJ, Chagin KM, Kattan MW, Reinke EK, Amendola A, Andrish JT, Brophy RH, Cox CL, Dunn WR (2018) Ten-year outcomes and risk factors after anterior cruciate ligament reconstruction: a MOON longitudinal prospective cohort study. Am J Sports Med 46(4):815–825
Palmieri-Smith RM, Wojtys EM, Potter HG (2016) Early cartilage changes after anterior cruciate ligament injury: evaluation with imaging and serum biomarkers—a pilot study. Arthrosc J Arthrosc Relat Surg 32(7):1309–1318
Amano K, Pedoia V, Su F, Souza RB, Li X, Ma CB (2016) Persistent biomechanical alterations after ACL reconstruction are associated with early cartilage matrix changes detected by quantitative MR. Orthop J Sports Med 4(4):2325967116644421
Proffen BL, Sieker JT, Murray MM, Akelman MR, Chin KE, Perrone GS, Patel TK, Fleming BC (2016) Extracellular matrix-blood composite injection reduces post-traumatic osteoarthritis after anterior cruciate ligament injury in the rat. J Orthop Res 34(6):995–1003
Potter HG, Linklater JM, Allen AA, Hannafin JA, Haas SB (1998) Magnetic resonance imaging of articular cartilage in the knee: an evaluation with use of fast-spin-echo imaging. J Bone Joint Surg Am 80(9):1276–1284
Titchenal MR et al (2018) Cartilage subsurface changes to magnetic resonance imaging UTE-T2* 2 years after anterior cruciate ligament reconstruction correlate with walking mechanics associated with knee osteoarthritis. Am J Sports Med 46(3):565–572
Wang X, Bennell KL, Wang Y, Wrigley TV, Van Ginckel A, Fortin K, Saxby DJ, Cicuttini FM, Lloyd DG, Vertullo CJ, Feller JA (2019) Tibiofemoral joint structural change from 2.5 to 4.5 years following ACL reconstruction with and without combined meniscal pathology. BMC Musculoskelet Disord 20(1):1
Mosher TJ, Dardzinski BJ, Smith MB (2000) Human articular cartilage: influence of aging and early symptomatic degeneration on the spatial variation of T2—preliminary findings at 3 T. Radiology 214(1):259–266
Çağlar E, Şahn G, Oğur T, Aktaş E (2014) Quantitative evaluation of hyaline articular cartilage T2 maps of knee and determine the relationship of cartilage T2 values with age, gender, articular changes. Eur Rev Med Pharma Col Sci 18(22):3386–3393
Culvenor AG, Collins NJ, Guermazi A, Cook JL, Vicenzino B, Khan KM, Beck N, van Leeuwen J, Crossley KM (2015) Early knee osteoarthritis is evident one year following anterior cruciate ligament reconstruction: a magnetic resonance imaging evaluation. Arthr Rheumatol 67(4):946–955
Haughom B, Schairer W, Souza RB, Carpenter D, Ma CB, Li X (2012) Abnormal tibiofemoral kinematics following ACL reconstruction are associated with early cartilage matrix degeneration measured by MRI T1rho. Knee 19:482–487
Potter HG, Jain SK, Ma Y, Black BR, Fung S, Lyman S (2012) Cartilage injury after acute, isolated anterior cruciate ligament tear: immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med 40:276–285
Hirose J, Nishioka H, Okamoto N, Oniki Y, Nakamura E, Yamashita Y, Usuku K, Mizuta H (2013) Articular cartilage lesions increase early cartilage degeneration in knees treated by anterior cruciate ligament reconstruction: T1ρ mapping evaluation and 1-year follow-up. Am J Sports Med 41(10):2353–2361
Li X, Kuo D, Theologis A, Carballido-Gamio J, Stehling C, Link TM, Ma CB, Majumdar S (2011) Cartilage in anterior cruciate ligament–reconstructed knees: MR imaging T1ρ and T2-initial experience with 1-year follow-up. Radiology 258(2):505
Su F, Hilton JF, Nardo L, Wu S, Liang F, Link TM, Ma CB, Li X (2013) Cartilage morphology and T1ρ and T2 quantification in ACL-reconstructed knees: a 2-year follow-up. Osteoarthr Cartil 21(8):1058–1067
Van Ginckel A, Verdonk P, Victor J, Witvrouw E (2013) Cartilage status in relation to return to sports after anterior cruciate ligament reconstruction. Am J Sports Med 41(3):550–559
Theologis AA, Haughom B, Liang F, Zhang Y, Majumdar S, Link TM, Ma CB, Li X (2014) Comparison of T1rho relaxation times between ACL-reconstructed knees and contralateral uninjured knees. Knee Surg Sports Traumatol Arthrosc 22(2):298–307
Joseph GB, Baum T, Alizai H, Carballido-Gamio J, Nardo L, Virayavanich W, Lynch JA, Nevitt MC, McCulloch CE, Majumdar S, Link TM (2012) Baseline mean and heterogeneity of MR cartilage T2 are associated with morphologic degeneration of cartilage, meniscus, and bone marrow over 3 years–data from the Osteoarthritis Initiative. Osteoarthr Cartil 20(7):727–735
Liebl H, Joseph G, Nevitt MC, Singh N, Heilmeier U, Subburaj K, Jungmann PM, McCulloch CE, Lynch JA, Lane NE, Link TM (2015) Early T2 changes predict onset of radiographic knee osteoarthritis: data from the osteoarthritis initiative. Ann Rheum Dis 74(7):1353–1359
Mihelic R, Jurdana H, Jotanovic Z, Madjarevic T, Tudor A (2011) Long-term results of anterior cruciate ligament reconstruction: a comparison with non-operative treatment with a follow-up of 17–20 years. Int Orthop 35(7):1093–1097
Ajuied A, Wong F, Smith C, Norris M, Earnshaw P, Back D, Davies A (2014) Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med 42(9):2242–2252
Cinque ME, Dornan GJ, Chahla J, Moatshe G, LaPrade RF (2018) High rates of osteoarthritis develop after anterior cruciate ligament surgery: an analysis of 4108 patients. Am J Sports Med 46(3):2011–2019
McNicholas MJ, Pengas IP, Assiotis A, Nash W, Hatcher J, Banks J (2012) Total meniscectomy in adolescents: a 40-year follow-up. J Bone Joint Surg Br 94(12):1649–1654
Papalia R, Del Buono A, Osti L, Denaro V, Maffulli N (2011) Meniscectomy as a risk factor for knee osteoarthritis: a systematic review. Br Med Bull 99:89–106
Titchenal MR, Chu CR, Erhart-HledikJC ATP (2017) Early changes in knee center of rotation during walking after anterior cruciate ligament reconstruction correlate with later changes in patient-reported outcomes. Am J Sports Med 45(4):915–921
Ushio T, Okazaki K, Osaki K, Takayama Y, Sagiyama K, Mizu-Uchi H, Hamai S, Akasaki Y, Honda H, Nakashima Y (2019) Degenerative changes in cartilage likely occur in the medial compartment after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 27(11):3567–3574
Russell C, Pedoia V, Amano K, Potter H, Majumdar S, Koff MF, Goldring SR, Goldring M, Hannafin JA, Marx RG, Nawabi DH, Otero M, Rodeo SA, Shah P, Warren RF, Amrami KK, Felmlee JP, Frick MA, Krych AJ, Stuart MJ, Williams SL, Kretzchmar M, Lansdown DA, Li A, Li X, Link TM, Benjamin Ma C, Okazaki N, Savic D, Schwaiger B, Su F, Wyatt C, Hardin JA (2017) Baseline cartilage quality is associated with voxel-based T1ρ and T2 following ACL reconstruction: a multicenter pilot study. J Orthop Res 35:688–698
Salmon LJ, Russell VJ, Refshauge K, Kader D, Connolly C, Linklater J, Pinczewski LA (2006) Long-term outcome of endoscopic anterior cruciate ligament reconstruction with patellar tendon autograft: minimum 13-year review. Am J Sports Med 34(5):721–732
Øiestadet BE, Engebretsen L, Storheim K, Risberg MA (2009) Winner of the 2008 systematic review competition: knee osteoarthritis after anterior cruciate ligament injury. Am J Sports Med 37(7):1434–1443
Patterson BE, Culvenor AG, Barton CJ, Guermazi A, Stefanik JJ, Morris HG, Whitehead TS, Crossley KM (2018) Worsening knee osteoarthritis features on magnetic resonance imaging 1 to 5 years after anterior cruciate ligament reconstruction. Am J Sports Med 46(12):2873–2883
André K, Prill R, Kayaalp E, Irlenbusch L, Liesaus E, Trommer T, Ullmann P, Becker R (2021) Increase in cartilage degeneration in all knee compartments after failed ACL reconstruction at 4 years of follow-up. J Orthop Traumatol 22(1):1–7
Harris K, Driban JB, Sitler MR, Cattano NM, Hootman JM (2015) Five-year clinical outcomes of a randomized trial of anterior cruciate ligament treatment strategies: an evidence-based practice paper. J Athl Train 50(1):110–112
Chalmers PN, Mall NA, Moric M, Sherman SL, Paletta GP, Cole BJ, Bach BR Jr (2014) Does ACL reconstruction alter natural history? A systematic literature review of long-term outcomes. JBJS 96(4):292–300
Acknowledgements
The author thanks all the study participants for their patience and support.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
NM was responsible for the conception/design of the work, data collection, writing the manuscript, statistical analysis, and accountability for the contents. AM was the supervisor for the work and revised the manuscript. AO revised and edited the manuscript and helped in figure and table editing. HY helped in data collection, writing the manuscript, and statistical analysis. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written consent was obtained from all patients before the procedure. This study was approved by the Research Ethics Committee of the Faculty of Medicine at Ain Shams University in Egypt in March 2020; Reference number of approval: MD87/2020.
Consent for publication
All patients included in this research gave written consent to publish the data contained within this study.
Competing interests
No financial or non-financial competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mabrouk, A.M., Abd El Raaof, M.M., Hemaida, T.W. et al. Degenerative changes through MR cartilage mapping in anterior cruciate ligament-reconstructed knees. Egypt J Radiol Nucl Med 54, 38 (2023). https://doi.org/10.1186/s43055-022-00952-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00952-4