
Abstract
Background
To develop a scoring system related to the lactate clearance (ΔLA) to predict the mortality risk (MELD-ΔLA) for critically ill cirrhotic patients.
Methods
In this retrospective cohort study, 881 critically ill cirrhotic patients from the Medical Information Mart for Intensive Care (MIMIC-III) database were included eventually. The outcomes of our study were defined as ICU death, 28-day, 90-day and 1-year mortality. Predictors were identified by multivariate Cox analysis to develop the predictive scoring system. The C-index and area under the curve (AUC) of receiver operator characteristic curve (ROC) were used to identify the predicting performance of the MELD-ΔLA, sequential organ failure assessment (SOFA), chronic liver failure-sequential organ failure assessment (CLIF-SOFA), the model for end-stage liver disease (MELD), Child–Pugh, chronic liver failure consortium acute-on-chronic liver failure (CLIF-C ACLF), chronic liver failure consortium-acute decompensation (CLIF-C AD) and MELD-Na scoring systems. Additionally, subgroup analysis was also performed based on whether critically ill cirrhotic patients underwent liver transplantation.
Results
Creatinine, bilirubin, international normalized ratio (INR), lactate first, ΔLA and vasopressors were closely associated with ICU death of liver critically ill cirrhotic patients. The C-index of the MELD-ΔLA in ICU death was 0.768 (95% CI 0.736–0.799) and the AUC for the MELD-ΔLA scoring system in predicting 28-day, 90-day, and 1-year mortality were 0.774 (95% CI 0.743–0.804), 0.765 (95% CI 0.735–0.796), and 0.757 (95% CI 0.726–0.788), suggested that MELD-ΔLA scoring system has a good predictive value than SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD) and MELD-Na scoring systems. Additionally, the study also confirmed the good predictive value of MELD-ΔLA scoring system for critically ill cirrhotic patients regardless of undergoing liver transplantation.
Conclusion
The developed MELD-ΔLA score is a simple scoring system in predicting the risk of ICU death, 28-day, 90-day and 1-year mortality for critically ill cirrhotic patients, which may have a good predictive performance.
Similar content being viewed by others


Background
Liver cirrhosis is a major health problem, causing high mortality and economic burden worldwide [1]. A large proportion of liver cirrhosis patients are prone to acute decompensation with organ failure, which need to be admitted to intensive care unit (ICU) [2]. Though liver cirrhosis patients have improved outcomes in ICU over the past decade, the prognosis for these patients still remains poor, with in-hospital mortality rates ranging from 39 to 83% [2]. Therefore, it is essential to carefully evaluate the prognosis of critically ill cirrhotic patients in clinical application, thereby reducing the risk of mortality.
Scoring systems in patients with liver cirrhosis have been widely used in assessing the prognosis of critically ill cirrhotic patients and making clinical decision, such as Child–Pugh score [3], sequential organ failure assessment (SOFA) score [4], chronic liver failure-sequential organ failure assessment (CLIF-SOFA) score [5], the model for end-stage liver disease (MELD) score [6], chronic liver failure consortium acute-on-chronic liver failure (CLIF-C ACLF) score [7], chronic liver failure consortium-acute decompensation (CLIF-C AD) score [7] and MELD-Na score [8]. At present, MELD was considered as an objective and effective system to evaluate the severity of patients than other scores, and was also a common method to quantify the mortality risk of ICU patients with cirrhosis. But some studies also purposed that only creatinine, bilirubin, and international normalized ratio (INR) were contained in the MELD scores, which might affect the assessment of the degree of cirrhosis [9, 10].
Lactate (LA) level is considered as a marker of metabolic changes caused by tissue hypoxia or stress response caused by adrenaline release [11]. A number of clinical studies have concluded that LA level has a good performance in predicting the prognosis of critically cirrhotic patients, suggesting the combination of LA level in the scoring system may improve the predicting performance of death in patients with liver cirrhosis [12, 13]. One study also confirmed that Child–Pugh-LA score, MELD-LA score, CLIF-SOFA-LA score could increase the predicting accuracy for mortality in acute chronic liver failure patients [11]. Recently, the measurements of LA dynamic changes in ICU have been found that significantly superior to static LA measurements in predicting mortality [14, 15]. A decrease in lactate clearance (ΔLA) has been reported to be closely associated with mortality in critically ill patients [16]. ΔLA seems to be more suitable for predicting death in patients with liver cirrhosis.
However, to our knowledge, there were few studies to assess the predictive value of MELD score incorporating ΔLA among critically ill cirrhotic patients. Herein, the aims of our study were: (1) to explore the risk factors associated with the death risk of critically ill cirrhotic patients, and the relationship of ΔLA and ICU death of critically ill cirrhotic patients; (2) to develop a scoring system related to the ΔLA in predicting the mortality risk in critically ill cirrhotic patients (MELD-ΔLA); (3) to compare the predictive performance of the MELD-ΔLA with SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na scores; (4) to assess the predictive performance of MELD-ΔLA score for death in critically ill cirrhotic patients with or without undergoing liver transplantation.
Methods
Data sources
Data of this retrospective cohort study were obtained from the Medical Information Mart for Intensive Care (MIMIC-III) database (version 1.3). The MIMIC-III is a large, single-center, freely available database, which contained the comprehensive and high-quality medical records of 50,000 patients admitted to ICU at the Beth Israel Deaconess Medical Center between 2001 and 2012 [17, 18].
Study eligibility criteria
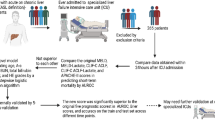
A total of 1840 patients were extracted from the MIMIC-III database 2001–2012 in this retrospective cohort study. Included criteria: ICU patients aged ≥ 18 years old with liver cirrhosis. However, participants were excluded from the study if they met one of the following criteria: (1) due to the data derived from the MIMIC-III database, we found there were some outliers in the age of the population, such as > 300 years of age; (2) patients with the history of liver transplantation; (3) patients without doing two lactate measurements who died within 48 h of ICU admission (Additional file 1: Fig. S1). Due to public availability of MIMIC-III database, with private information of all patients being anonymized, the local ethics committee’s approval was not required.
Data collection
We collected the baseline characteristics and laboratory parameters of all patients on the first day after ICU admission. The baseline characteristics were included: age (years), gender, insurance type, ICU type, marital status, race, etiology of cirrhosis, acute chronic liver failure (ACLF), characteristics of cirrhosis, therapy. Laboratory parameters included temperature (℃), heart rate (times/min), systolic blood pressure (SBP) and diastolic blood pressure (DBP), mean arterial pressure (MAP), ratio of pulse oxygen saturation to fraction of inspired oxygen (SPO2/FiO2), ratio of arterial oxygen partial pressure to fraction of inspired oxygen (PaO2/FiO2), bilirubin (mg/dL), creatinine (mg/dL), international normalized ratio (INR), prothrombin time (PT), albumin, glucose, pH, sodium (mmol/L), potassium (mmol/L), hemoglobin (g/dL), white blood cell (WBC, 109/L) count, chloride, platelet count (PLT, 109/L), lactate first (mmol/L), lactate last (mmol/L), ICU stay time (days). SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na.
Liver cirrhosis was defined as advanced liver fibrosis caused by multiple forms of liver disease, including hepatitis and chronic alcoholism [19]. In this study, we used International Classification of Disease (ICD-9) codes to identify critically ill cirrhotic patients (5712, 5715 and 5716) and critically ill cirrhotic patients who underwent liver transplantation (5051 and 5059). Lactate first: lactate of first measurement within 2 days after admission to ICU; lactate last: lactate of last measurement within 2 days after admission to ICU; ΔLA was defined as: (lactate first-lactate last)/lactate first × 100; the MELD score was calculated as following: 9.57 × loge [creatinine (mg/dL)] + 3.78 × loge [bilirubin (mg/dL)] + 11.2 × loge (INR) + 6.43 [18]; the CLIF-C ACLF score was calculated by using the following formula: 10 × (0.33 × CLIF-C organ failure score + 0.04 × Age + 0.63 × ln (WBC)-2 [7]; the CLIF-C ACLF-D score was calculated: CLIF-C ACLF-D score = [(0.03 × Age) + (0.45 × Ascites) + (0.26 × ln (WBC)] − (0.37 × Albumin) + [0.57 × ln (Bilirubin)] + [1.72 × ln (Creatinine)] + 3 × 10 [7]. The MELD-Na score was obtained: MELD-Na = MELD + 1.32 × (137-Na)- [0.033 × MELD × (137-Na)] [20]; the CLIF-SOFA, SOFA and Child–Pugh scores were calculated according to published methods, respectively [21,22,23].
Outcomes
The outcomes of our study were defined as ICU death, 28-day, 90-day and 1-year mortality. ICU death was regarded as death before ICU discharge. The 28-day, 90-day and 1-year mortality were defined as deaths within 28 days, 90 days, and 1 year after ICU discharge. The start date of follow-up was the date of the patient’s admission. The follow-up time was 1 year, and once death occurred for patients, the follow-up was terminated. The rate of loss to follow-up in this study was 0%.
Statistical analysis
The measurement data of the normal distribution were reported as Mean ± Standard Error (Mean ± SE); and the comparison between groups was performed by Student’s t-test. Median and quartile spacing [M (Q1, Q3)] was used to depict the non-normal data; and the comparison between the two groups was analyzed by Mann–Whitney U rank-sum test. The categorical data was described by the number of cases and composition ratio n (%), and were compared by Chi-square or Fisher’s exact test. These missing values were filled by using multiple imputation (Additional file 2: Table S1).
Firstly, all eligible patients were divided into ICU-survival group and ICU-death group based on the occurrence of ICU death, and conducted the difference analysis between two groups. Then we performed the univariate and multivariate COX analyses which aimed to explore the independent predictors related to ICU death for critically ill cirrhotic patients. And we used these related predictors to develop a predictive scoring system (MELD-ΔLA) in predicting the ICU mortality risk among critically ill cirrhotic patients. Next, the C-index and area under the curve (AUC) of receiver operator characteristic curve (ROC) were adopted to compare the predicting performance between developed MELD-ΔLA and other scoring systems (SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na scores) for ICU death, 28-day, 90-day and 1-year mortality among critically ill cirrhotic patients. Calibration curves were used to evaluate the calibration of the developed MELD-ΔLA score, and the more closely the two lines fit, indicates a better prediction. Finally, subgroup analysis was performed based on whether critically ill cirrhotic patients underwent liver transplantation, and hazard ratio (HR) and 95% confidence interval (CI) were calculated. The two-sided test was conducted for all statistical analyses. SAS 9.4 software was used for all statistical analyses and R 4.0.2 software was used for drawing. P < 0.05 was considered statistically significant. This study followed TRIPOD guidelines for the development of scores for outcome prediction.
Results
Baseline characteristics
After excluded patients who were over 300 years of age (n = 15), had the history of liver transplant (n = 140), and were not made two lactate measurements or died within 48 h of ICU admission (n = 804), a total of 881 eligible patients were enrolled eventually in this study, with an average age of 58.65 ± 11.57 years old. They were divided into ICU-survival group (n = 628) and ICU-death group (n = 253), respectively. As shown in Table 1, there were some variables (such as ICU type, lactate first, lactate last, ΔLA, et al.) with significant differences between two groups (P < 0.05).
Predictor selection of ICU death in critically ill cirrhotic patients
Table 2 suggests that the effects of ACLF, RRT, vasopressors, transplant, temperature, SBP, DBP, MAP, PaO2/FiO2, PaO2/FiO2, bilirubin, creatinine, INR, PT, albumin, pH, sodium, potassium, WBC, chloride, lactate first, lactate last and ΔLA on ICU death among patients with critically ill cirrhotic had significant differences (P < 0.05). The variables with significant differences in univariate COX analysis were incorporated into multivariate COX analysis and screened step by step. As illustrated in Table 3, creatinine, bilirubin, INR, lactate first, ΔLA and vasopressors were closely associated with ICU death for critically ill cirrhotic patients. For each 1 mg/dL increase in creatinine, bilirubin, INR and lactate first, the risk of ICU death increased 0.075-fold (HR = 1.075, 95% CI 1.004–1.151), 0.022-fold (HR = 1.022, 95% CI 1.008–1.035), 0.102-fold (HR = 1.102, 95% CI 1.011–1.201) and 0.142-fold (HR = 1.142, 95% CI 1.098–1.187), separately among liver cirrhosis patients. Similarly, the risk of ICU death in critically ill cirrhotic patients with vasopressors was 2.560 times higher than those without the using history of vasopressors (HR = 2.560, 95% CI 1.959–3.345). Additionally, it should be noticed that ΔLA (per 1% increase) reduced the risk of ICU death in critically ill cirrhotic patients by 0.341-fold (HR = 0.659, 95% CI 0.610–0.712). Additional file 3: Fig. S3 shows the survival curves dependent on the ΔLA. We took the median of Lactate changes as a cut-off. Compared with the ΔLA < 16.22%, the survival rate of ΔLA ≥ 16.12% was better.
Establishment and performance of the MELD-ΔLA scoring system
MELD-ΔLA score was generated by the optimal cutoff point for each factor determined via the Youden index. MELD-ΔLA score was composed of creatinine, bilirubin, INR, lactate first, ΔLA and the using history of vasopressors, and detailed information was given in Table 4. Furthermore, we also calculated a combined formula based on the formula of a regression model with metric variables as following: (Combined formula = h0(t) × e (Creatinine × 0.072+ Bilirubin × 0.021 + INR × 0.097+ Lactate first × 0.132 − ΔLA × 0.417 + Vasopressors (Yes) × 0.940). And we compared the predicting performance of combined formula and MELD-ΔLA score (Table 5). Although the C-indexes of the combined formula in ICU death was 0.789 (95% CI 0.756–0.823), and the AUC for the combined formula in predicting 28-day, 90-day, and 1-year mortality were 0.800 (95% CI 0.771–0.830), 0.785 (95% CI 0.755–0.814), and 0.762 (95% CI 0.731–0.793), respectively, which were higher than MELD-ΔLA score, there was no significant difference for combined formula, thus we cannot obtain a conclusion that the predicting performance of combined formula was higher than MELD-ΔLA score. Additionally, MELD-ΔLA score was a more simple and convenient scoring system for clinical application than the combined formula. Figure 1 also indicated that the relation of MELD-ΔLA score and ICU death, 28-day, 90-day and 1-year mortality among critically ill cirrhotic patients, with a positive correlation. Additionally, Additional file 4: Fig. S4 presents a survival figure of using the MELD-ΔLA score, and the result indicated that the higher the MELD-ΔLA score, the worse the survival probability.

The association of MELD-ΔLA score and ICU death, 28-day, 90-day and 1-year mortality in liver cirrhosis patients
Importantly, we compared the predicting performance of MELD-ΔLA and SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na scoring systems for ICU death, 28-day, 90-day and 1-year mortality among all critically ill cirrhotic patients (Table 5). The C-indexes of the MELD-ΔLA, SOFA, CLIF-SOFA, MELD, Child–Pugh, and MELD-Na in ICU death were 0.768 (95% CI 0.736–0.799), 0.715 (95% CI 0.675–0.755), 0.722 (95% CI 0.685–0.758), 0.671 (95% CI 0.634–0.708), 0.617 (95% CI 0.580–0.654) and 0.708 (95% CI 0.671–0.746), separately; the AUC for the MELD-ΔLA scores in predicting 28-day, 90-day, and 1-year mortality were 0.774 (95% CI 0.743–0.804), 0.765 (95% CI 0.735–0.796), and 0.757 (95% CI 0.726–0.788), respectively, which were obviously higher than SOFA, CLIF-SOFA, MELD, Child–Pugh and MELD-Na scoring systems (Fig. 2). Also, for patients with ACLF, the C-indexes of the MELD-ΔLA score and CLIF-C ACLF score in ICU death were 0.725 (95% CI 0.686–0.764) and 0.652 (95% CI 0.608–0.696), respectively; and the AUC for the CLIF-C ACLF score in predicting 28-day, 90-day, and 1-year mortality were 0.696 (95% CI 0.652–0.739), 0.691 (95% CI 0.647–0.736), and 0.684 (95% CI 0.637–0.730), separately, which were lower than MELD-ΔLA score. Similarly, for patients without ACLF, the C-indexes of the MELD-ΔLA score and CLIF-C AD score in ICU death were 0.861 (95% CI 0.812–0.910) and 0.717 (95% CI 0.619–0.816), respectively; and the AUC for the CLIF-C AD score in predicting 28-day, 90-day, and 1-year mortality were 0.705 (95% CI 0.635–0.775), 0.688 (95% CI 0.625–0.751), and 0.700 (95% CI 0.642–0.759), respectively, which were also lower than MELD-ΔLA score. In short, these results indicated that the predicting performance of developed MELD-ΔLA score was higher SOFA score, CLIF-SOFA score, MELD score, Child–Pugh score, MELD-Na score, the CLIF-C ACLF score in patients with ACLF, and the CLIF-C AD score in patients without ACLF.

ROC curves of (a) 28-day, (b) 90-day, and (c) 1-year death for MELD-ΔLA score
Furthermore, the calibration curves also revealed a relatively high degree of agreement between the prediction results of MELD-ΔLA scoring system and the actual results (Additional file 5: Fig. S5). These results implied that MELD-ΔLA score has a good discrimination in predicting the risk of ICU death, 28-day, 90-day and 1-year mortality for critically ill cirrhotic patients.
Validation for the performance of scoring system in different subgroups based on whether patients with critically ill cirrhotic underwent liver transplant
In this study, we also carried out a subgroup analysis based on whether critically ill cirrhotic patients underwent liver transplantation (Table 5). As shown in Table 5, the C-indexes of the MELD-ΔLA scoring system were 0.887 (95% CI 0.749–0.999) in critically ill cirrhotic patients underwent liver transplantation and 0.758 (95% CI 0.726–0.790) in critically ill cirrhotic patients without liver transplantation. In addition, the AUC for the MELD-ΔLA scoring system at predicting 28-day, 90-day, and 1-year mortality were higher than other scoring systems (SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na), regardless of whether critically ill cirrhotic patients had undergone liver transplantation. These results confirmed a good predictive value of MELD-ΔLA score regardless of undergoing liver transplantation for critically ill cirrhotic patients.
Discussion
In this retrospective cohort study, we reported several key factors regarding the risk of ICU death among critically ill cirrhotic patients and expounded the negative correlation between ΔLA and the risk of ICU death among critically ill cirrhotic patients. More importantly, our study developed an objective and simpler prediction score (MELD-ΔLA) to assess the risk of ICU death, 28-day, 90-day and 1-year mortality among critically ill cirrhotic patients, and there was a significantly positive association between MELD-ΔLA score and ICU death, 28-day, 90-day and 1-year mortality in critically ill cirrhotic patients. Additionally, the findings illustrated that MELD-ΔLA score has a better predictive value than other scores (SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na) among critically ill cirrhotic patients. Not only that, the MELD-ΔLA score also showed the good predictive value for critically ill cirrhotic patients who had or had not undergone liver transplantation.
MELD-ΔLA score mainly contained six predictors of creatinine, bilirubin, INR, lactate first, ΔLA and the using history of vasopressors. The levels of creatinine, bilirubin, INR were closely associated with the risk of ICU death among critically ill cirrhotic patients, which were consistent with previous studies [6, 24, 25]. It’s worth paying attention to ΔLA plays a vital role in the MELD-ΔLA scoring system among critically ill cirrhotic patients. Recently, lactate level has been proved to assess the severity of disease, which has become an effective biomarker in clinical diagnosis [10]. There was a high lactate level for most patients with chronic liver disease, which the reason may be tissue hypoperfusion of critically ill patients and decreased ΔLA in advanced liver disease [26]. One study has showed that lactate level not only reflected the severity of organ failure, but was also an independently risk factor for short-term mortality of critically ill cirrhotic patients [12]. Several studies have incorporated lactate level into scoring systems to better predict death in patients with liver cirrhosis [27, 28]. Sarmast et al. developed a MELD-Lactate model and reported that MELD-Lactate model could be used to identify patients with chronic liver disease for the risk of ICU mortality [9]. Nevertheless, simply measuring lactate level at one time may be not accurately reflect the dynamic oxygenation status of tissues and the severity of disease, thereby, more attention should be paid to the role of ΔLA [29, 30]. To date, most researches only focused on the development of lactate level in liver cirrhosis patients [12, 27], there was few studies to investigate the influence of ΔLA in the scoring system for the ICU mortality. To our knowledge, this is the first study conducted to develop a MELD-ΔLA score to predict the risk of ICU death and 28-day, 90-day and 1-year death among critically ill cirrhotic patients; the decreased of ΔLA was distinctly related to higher risk of ICU mortality among critically ill cirrhotic patients.
The predictive factors of the developing MELD-ΔLA scoring system could be easily obtained in critically ill cirrhotic patients, which suggested the scoring system would be simpler and more convenient for the clinical practice. Besides, the study also found that MELD-ΔLA scoring system expressed an advanced diagnostic discrimination than other scoring systems (SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na) in ICU death and 28-day, 90-day and 1-year mortality for critically ill cirrhotic patients. Likewise, the MELD-ΔLA scoring system has also been demonstrated a good predictive ability for critically ill cirrhotic patients who were with or without undergoing liver transplantation. In general, the developed MELD-ΔLA score is a simple, intuitive, and objective scoring system to help clinician in better predicting the risk of ICU death and 28-day, 90-day and 1-year mortality for critically ill cirrhotic patients than other scoring systems.
The major strength of our study is the development of MELD-ΔLA scoring system which makes it easier for clinicians to assess the risk of death among critically ill cirrhotic patients. However, this study also has some limitations. Firstly, the sample size was not large enough with a retrospective cohort study, which might have bias for the result of our study. Secondly, because of all data of this study derived from the MIMIC-III database, we could not get the specific time of lactate measurement for all patients. Thirdly, the developed MELD-ΔLA score has a better predictive value than other scoring systems, which was only applicable to critically ill cirrhotic patients. We cannot be sure if MELD-ΔLA score has similar predictive power among other populations. Finally, there was a lack of external validation to assess the predictive ability of this scoring system. These should be cautious in interpreting the results. Hence, further studies should be required to validate the results of the present study, promoting the introduction of this scoring system into clinical practice.
Conclusion
In summary, the developed MELD-ΔLA score is a simple scoring system to assess the risk of ICU death, 28-day, 90-day and 1-year death among critically ill cirrhotic patients, which might have a better predictive value compared to SOFA, CLIF-SOFA, MELD, Child–Pugh, CLIF-C ACLF, CLIF-C AD and MELD-Na scores.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available in the MIMIC-III repository, https://mimic.mit.edu/.
Abbreviations
- ICU:
-
Intensive care unit
- SOFA:
-
Sequential organ failure assessment
- MELD:
-
Model for end-stage liver disease
- INR:
-
International normalized ratio
- ΔLA:
-
Decrease in lactate clearance
- MELD-ΔLA:
-
Mortality risk in critically ill cirrhotic patients
- MIMIC-III:
-
Medical Information Mart for Intensive Care
- ACLF:
-
Acute chronic liver failure
- SBP:
-
Systolic blood pressure
- CLIF-C ACLF:
-
Chronic liver failure consortium acute-on-chronic liver failure
- CLIF-C AD:
-
Chronic liver failure consortium-acute decompensation
- DBP:
-
Diastolic blood pressure
- MAP:
-
Mean arterial pressure
- INR:
-
International normalized ratio
- PT:
-
Prothrombin time
- WBC:
-
White blood cell count
- PLT:
-
Platelet count
- Mean ± SE:
-
Mean ± standard error
- M (Q1, Q3):
-
Median and quartile spacing
- ROC:
-
Receiver operator characteristic curve
- HR:
-
Hazard ratio
- CI:
-
Confidence interval
References
Moon AM, Singal AG, Tapper EB. Contemporary epidemiology of chronic liver disease and cirrhosis. Clin Gastroenterol Hepatol. 2020;18(12):2650–66.
Weil D, Levesque E, McPhail M, Cavallazzi R, Theocharidou E, Cholongitas E, et al. Prognosis of cirrhotic patients admitted to intensive care unit: a meta-analysis. Ann Intensive Care. 2017;7(1):33.
Wan SZ, Nie Y, Zhang Y, Liu C, Zhu X. Assessing the prognostic performance of the child-pugh, model for end-stage liver disease, and albumin-bilirubin scores in patients with decompensated cirrhosis: a large asian cohort from gastroenterology department. Dis Markers. 2020;2020:5193028.
McPhail MJ, Shawcross DL, Abeles RD, Chang A, Patel V, Lee GH, et al. Increased survival for patients with cirrhosis and organ failure in liver intensive care and validation of the chronic liver failure-sequential organ failure scoring system. Clin Gastroenterol Hepatol. 2015;13(7):1353-60.e8.
Pan HC, Jenq CC, Tsai MH, Fan PC, Chang CH, Chang MY, et al. Scoring systems for 6-month mortality in critically ill cirrhotic patients: a prospective analysis of chronic liver failure—sequential organ failure assessment score (CLIF-SOFA). Aliment Pharmacol Ther. 2014;40(9):1056–65.
Francoz C, Belghiti J, Castaing D, Chazouillères O, Duclos-Vallée JC, Duvoux C, et al. Model for end-stage liver disease exceptions in the context of the French model for end-stage liver disease score-based liver allocation system. Liver Transpl. 2011;17(10):1137–51.
Kuo CC, Huang CH, Chang C, Chen PC, Chen BH, Chen WT, Ho YP. Comparing CLIF-C ACLF, CLIF-C ACLFlactate, and CLIF-C ACLF-D prognostic scores in acute-on-chronic liver failure patients by a single-center ICU experience. J Pers Med. 2021;11(2):79.
Goudsmit BFJ, Putter H, Tushuizen ME, de Boer J, Vogelaar S, Alwayn IPJ, et al. Validation of the model for end-stage liver disease sodium (MELD-Na) score in the Eurotransplant region. Am J Transplant. 2021;21(1):229–40.
Sarmast N, Ogola GO, Kouznetsova M, Leise MD, Bahirwani R, Maiwall R, et al. Model for end-stage liver disease-lactate and prediction of inpatient mortality in patients with chronic liver disease. Hepatology. 2020;72(5):1747–57.
Mahmud N, Asrani SK, Kaplan DE, Ogola GO, Taddei TH, Kamath PS, et al. The predictive role of model for end-stage liver disease-lactate and lactate clearance for in-hospital mortality among a national cirrhosis cohort. Liver Transpl. 2021;27(2):177–89.
Nie Y, Zhang Y, Liu LX, Zhu X. Serum lactate level predicts short-term and long-term mortality of HBV-ACLF patients: a prospective study. Ther Clin Risk Manag. 2020;16:849–60.
Drolz A, Horvatits T, Rutter K, Landahl F, Roedl K, Meersseman P, et al. Lactate improves prediction of short-term mortality in critically Ill patients with cirrhosis: a multinational study. Hepatology. 2019;69(1):258–69.
Tas A, Akbal E, Beyazit Y, Kocak E. Serum lactate level predict mortality in elderly patients with cirrhosis. Wien Klin Wochenschr. 2012;124(15–16):520–5.
Vincent JL, Quintairos ESA, Couto L Jr, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20(1):257.
Zhang Z, Xu X. Lactate clearance is a useful biomarker for the prediction of all-cause mortality in critically ill patients: a systematic review and meta-analysis. Crit Care Med. 2014;42(9):2118–25.
Gao F, Huang XL, Cai MX, Lin MT, Wang BF, Wu W, et al. Prognostic value of serum lactate kinetics in critically ill patients with cirrhosis and acute-on-chronic liver failure: a multicenter study. Aging (Albany NY). 2019;11(13):4446–62.
Johnson AE, Pollard TJ, Shen L, Lehman LW, Feng M, Ghassemi M, et al. MIMIC-III, a freely accessible critical care database. Sci Data. 2016;3: 160035.
Zhou XD, Chen QF, Zhang MC, Van Poucke S, Liu WY, Lu Y, et al. Scoring model to predict outcome in critically ill cirrhotic patients with acute respiratory failure: comparison with MELD scoring models and CLIF-SOFA score. Expert Rev Gastroenterol Hepatol. 2017;11(9):857–64.
Lee NY, Suk KT. The role of the gut microbiome in liver cirrhosis treatment. Int J Mol Sci. 2020;22(1):199.
https://aasldpubs.onlinelibrary.wiley.com/doi/epdf/https://doi.org/10.1002/cld.464.
Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144(7):1426–37. https://doi.org/10.1053/j.gastro.2013.02.042.
Boone MD, Celi LA, Ho BG, Pencina M, Curry MP, Lior Y, et al. Model for end-stage liver disease score predicts mortality in critically ill cirrhotic patients. J Crit Care. 2014;29(5):881.e7-13.
Kok B, Abraldes JG. Child-pugh classification: time to abandon? Semin Liver Dis. 2019;39(1):96–103.
Allegretti AS, Solà E, Ginès P. Clinical application of kidney biomarkers in cirrhosis. Am J Kidney Dis. 2020;76(5):710–9.
Dunn W, Jamil LH, Brown LS, Wiesner RH, Kim WR, Menon KV, et al. MELD accurately predicts mortality in patients with alcoholic hepatitis. Hepatology. 2005;41(2):353–8.
Cheng CY, Kung CT, Wu KH, Chen FC, Cheng HH, Cheng FJ, et al. Liver cirrhosis affects serum lactate level measurement while assessing disease severity in patients with sepsis. Eur J Gastroenterol Hepatol. 2021;33(9):1201–8.
Kim S, Zerillo J, Tabrizian P, Wax D, Lin HM, Evans A, et al. Postoperative meld-lactate and isolated lactate values as outcome predictors following orthotopic liver transplantation. Shock. 2017;48(1):36–42.
Warren A, Soulsby CR, Puxty A, Campbell J, Shaw M, Quasim T, et al. Long-term outcome of patients with liver cirrhosis admitted to a general intensive care unit. Ann Intensive Care. 2017;7(1):37.
Perilli V, Aceto P, Sacco T, Ciocchetti P, Papanice D, Lai C, et al. Usefulness of postreperfusion lactate clearance for predicting early graft recovery in liver transplant patients: a single center study. Minerva Anestesiol. 2018;84(10):1142–9.
Masyuk M, Wernly B, Lichtenauer M, Franz M, Kabisch B, Muessig JM, et al. Prognostic relevance of serum lactate kinetics in critically ill patients. Intensive Care Med. 2019;45(1):55–61.
Acknowledgements
Not applicable.
Funding
This study is supported by the National Thirteen Five-year Science and Technology Major Project of China (No. 2018ZX10725506-002) and National Twelve Five-year Science and Technology Major Project of China (No. 2012ZX10005-005).
Author information
Authors and Affiliations
Contributions
XL and SW designed the study. XL wrote the manuscript. MG, SF and JZ collected, analyzed and interpreted the data. SW critically reviewed, edited and approved the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Due to public availability of MIMIC-III database, with private information of all patients being anonymized, the local ethics committee’s approval was not required. All experiments were performed in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional
file 1. Supplemental Figure 1. The consort figure of extracted patient.
Additional
file 2. Supplemental Table 1. The sensitivity analysis of missing data before and after interpolation.
Additional
file 3. Supplemental Figure 2. The survival curves dependent on the lactate changes.
Additional
file 4. Supplemental Figure 3. A survival figure related to the MELD-ΔLA score.
Additional
file 5. Supplemental Figure 4. The calibration curves of MELD-ΔLA score.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, X., Gong, M., Fu, S. et al. Establishment of MELD-lactate clearance scoring system in predicting death risk of critically ill cirrhotic patients. BMC Gastroenterol 22, 280 (2022). https://doi.org/10.1186/s12876-022-02351-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12876-022-02351-5