
Abstract
Mesenchymal stromal/stem cells (MSCs) possess multi-lineage differentiation and self-renewal potentials. MSCs-based therapies have been widely utilized for the treatment of diverse inflammatory diseases, due to the potent immunoregulatory functions of MSCs. An increasing body of evidence indicates that MSCs exert their therapeutic effects largely through their paracrine actions. Growth factors, cytokines, chemokines, extracellular matrix components, and metabolic products were all found to be functional molecules of MSCs in various therapeutic paradigms. These secretory factors contribute to immune modulation, tissue remodeling, and cellular homeostasis during regeneration. In this review, we summarize and discuss recent advances in our understanding of the secretory behavior of MSCs and the intracellular communication that accounts for their potential in treating human diseases.
Similar content being viewed by others


The identification of MSCs
In 1970, Alexander J. Friedenstein and colleagues described an adherent and non-hematopoietic cell type present in the mouse bone marrow (BM) that could form fibroblast-like colonies in vitro, unlocking the door to the world of mesenchymal stem cells (MSCs).1 While MSCs, which are later found to reside in various organs, can generally self-renew and exhibit stromal cell-like characteristics in vitro, the lineages that contribute to MSCs in each organ in vivo and their spatiotemporal changes during development have yet to be well explored. An early study of the hierarchy of BM-derived mesenchymal progenitors showed that Sca1+ progenitors can differentiate into CD146+ and CD166+ progenitors sequentially.2 While all three types of progenitors support bone formation, only Sca1+ progenitors can home back to the BM through a chemotactic axis post-intravenous infusion. Another report showed that the niches formed by interleukin (IL)-7+ mesenchymal progenitors could functionally regulate hematopoietic stem cell maintenance and multilineage differentiation.3 These MSCs in BM highly express the intermediate filament protein nestin and are located around hematopoietic stem cells (HSCs).4 The nestin+ MSCs are proven to regulate the homing of transplanted HSCs to BM,4 as well as guiding immune cells to egress to circulation.5 In other organs, most of the mesenchymal progenitors are closely associated with capillaries and blood vessels.6,7,8 These perivascular cells display phenotypes similar to those of MSCs derived from BM and dental pulps.9 A population of stromal cells that resides among choroidal vascular endothelial cells was also recognized to display the MSC phenotype and possess the capacity for mesenchymal differentiation.10 Thus, blood vessel walls in diverse human tissues (such as BM, umbilical cord (UC), adipose, muscle, and placenta) are considered as the primary dwellings of progenitor cells that give rise to MSCs.
The first batch of MSCs during embryonic development could be traced to Sox1+ neuroepithelium partly through a neural crest intermediate stage,11 arguing for their ectodermal origin. The MSC lineages during organ development are being actively investigated and, owing to the widespread use of single-cell sequencing, imaging analysis, and tracing technologies, functionally distinct new subsets of MSCs are emerging rapidly.
MSC isolation and characterization
Well-characterized MSCs can now be isolated and propagated in vitro from multiple organs (such as BM, dental pulp, thymus, muscle, pancreas, and lung).12 According to the International Society for Cellular Therapy (ISCT)-published minimal guidelines to define human MSC identity, the isolated cells are generally positive for CD105, CD73, and CD90, and negative for CD45, CD34, CD14, or CD11b, CD79α, or CD19 and MHC class II.13 Additionally, these cells possess the potential of specific-lineage differentiation toward osteoblasts, adipocytes, or chondrocytes, as well as the capacity of plastic adherence when cultured in vitro.
Tissue specificity
MSCs isolated from different sources can vary in their gene expression patterns and differentiation potentials.14 There are several non-classical markers (such as CD36, CD163, CD271, CD200, CD273, CD274, CD146, CD248, and CD140b) that potentially distinguish MSCs of different sources.15 For instance, CD271 is a surface marker for the majority of BM-derived MSCs (MSC(BM)s),16,17 while this marker is inadequate for the isolation of MSCs from other sources(such as UC, dental pulp, or placenta).18 Lately, a population of highly proliferative multipotent progenitors marked by dipeptidyl peptidase-4 (DPP4)/CD26 has been discovered during the development of subcutaneous adipose tissue in mice through single-cell RNA sequencing analysis. These progenitor cells could produce two subpopulations, committed preadipocytes marked by intercellular adhesion molecule-1 (ICAM-1) and CD142.19 More recently, the MSCs/fibroblast atlases were constructed by integrating available single-cell transcriptomic data.20 Based on the transcription profiles across tissues, two universal subtypes were identified as the primitive lineages to generate more specialized descendants in health and disease.
Since freshly isolated MSCs comprise multiple MSC subgroups or progenitors varying in proportions depending on the source of origin, MSCs with different tissue origins may meet specific needs. For example, MSC(AD)s are more efficient in supporting hematopoiesis and angiogenesis than MSC(BM)s.21 Human UC-derived MSCs (MSC(UC)s) exhibit a relatively more stable capacity of proliferation and trilineage differentiation than MSC(BM)s.22 Compared to MSCs from BM, adipose tissue, or placenta, MSC(UC)s possess the strongest potential to suppress T lymphocyte proliferation by inducing cell-cycle arrest (G0/G1 phase) and apoptosis, along with altered expression of apoptosis-related genes.23
Cell plasticity
The phenotype and biological features of MSCs could be dynamically altered by culture conditions, leading to distinct capacities of differentiation and proliferation during their expansion in vitro. Freshly isolated MSC(BM)s from humans and mice lack the expression of CD44 but display poly directional differentiation potential.24 During in vitro expansion, freshly isolated MSC(BM)s acquire CD44 expression without compromising their proliferation efficiency or differential potential, accompanied by dramatic upregulation of hyaluronan synthases (HAS1 and HAS2), growth factors, and matrix proteins.24 On the other hand, young MSCs undergo cellular senescence in response to transforming growth factor-β (TGFβ2), while anti-TGFβ antibodies could reverse the aging phenotypes of old MSCs.25 In addition, peritoneal dialysis effluent-derived MSCs (MSC(P)s) displayed a homogeneous pattern of classical MSC markers with multipotency in vitro, which was decided by specific culture medium.26 MSC subsets with distinct phenotypic and functional properties could be furtherly identified by using markers including CD56 and MSC antigen-1 (MSCA-1).27 Nestin marks human MSC(BM)s that are more readily differentiated to insulin-producing cells (IPCs) than the nestin− cells.28 They highly express maintenance genes and favor BM homing of HSCs.4 CD271+ adult MSCs show higher clonogenic and osteogenic capacities than CD271− ones.29 The Thy-1(CD90)−/− MSCs are unable to form healthy bone tissues as the wild-type counterparts do and are more likely to differentiate into adipocytes.30 On the contrary, the inflammatory cytokine lipocalin-2 is shown to augment the transcription of osteogenic genes in MSCs, exacerbating the cascade of dysregulated cellular events in myelofibrosis.31 Revealing this high plasticity of MSCs has opened new perspectives to explain the disrupted balance of adipogenesis and osteogenesis in developmental and metabolic diseases.
Therapeutic applications of MSCs
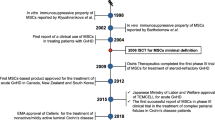
Researchers were firstly attracted by the self-renewal capacity of MSCs and their differentiation potential towards multiple lineages, afterwards the ability of MSCs to regulate immune responses was discovered. These biological properties of MSCs promoted the development of therapeutics for tissue regeneration. MSC(BM)s, as one of the main supporters for hematopoiesis, could restore defective BM microenvironment for myelopoiesis. They are also involved in lymphocyte maturation32,33 and integrate with the inordinate immune system to modulate tumor progression, such as reprogramming host macrophages to retard leukemia development.34 Both allogenic or autologous MSCs are able to traverse the circulation through the chemotactic network and migrate to specific destinies to support the growth or function of resident cells in the lesion sites. This mobility feature and the low immunogenicity endow MSCs with biological acceptability in vivo. Strikingly, MSC(BM)s can greatly inhibit the immune responses mediated by active lymphocytes in a dose-dependent manner.35 This regulatory potential of MSCs has attracted much attention and has been shown to be surprisingly effective in controlling inflammation and balancing immune response. Allogenic MSCs were shown to promote orthopaedical repair,36 skin wound healing,37 and nerve regeneration/reconnection.38 The clinical superiority of MSCs in treating inflammatory and degenerative diseases has been intensively reported. As of November 25, 2021, a total of 965 mesenchymal stromal/stem cell-based, clinical trials had been registered in the US National Institutes of Health (https://clinicaltrials.gov/), including ongoing, withdrawal, complete and unknown status studies (Table 1). Apparently, the MSC-based clinical trials are mainly applied to inflammation, wound healing, infection, organ dysfunction, as well as degenerative diseases in different organs and tissues (Fig. 1). However, several pitfalls of engrafted MSCs are encountered during practical use, such as their limited vitality,39 uncertain responsiveness, as well as the difficulty in monitoring their differentiation in situ. The massive expansion of MSCs in vitro also incur high cost, which cannot be afforded by many financially strapped patients, especially when taking the transient curative effect into consideration. A shift in focus from MSCs allografting to the effector molecules that mediate the cell-specific effects should bypass the disadvantages resulting from immune compatibility, tumorigenicity, and the unpredictable pathogen carried by living cells, in addition to the pitfalls listed above.40

MSC-based clinical trials involve a variety of diseases in different organs and tissues. MSC-based clinical trials are mainly applied to the diseases associated with inflammation, wound healing, infection, as well as degeneration in diverse organs and tissues. The figure shows the types of diseases that have completed clinical trials (reproductive diseases and aging are not listed), and the most widely applied diseases involve the bone and nervous system. MSCs possess a strong capacity in balancing immune responses, especially in autoimmune disorders, such as GvHD and Crohn’s disease. As a lot of refractory diseases are often combined with poor repairing of damaged tissues and dysfunction of diseased organs, such as bones nonunion and multiple sclerosis, the clinicians also favor the multi-directional differentiation potential and pleiotropic effects of MSCs, to promote wound healing and functional recovery. In addition, researchers have been gradually investigating the therapeutic potential of MSC-based therapy in some congenital diseases. (Created with BioRender.com)
The secretory functions of MSCs
MSCs engraftment is usually limited by the rigorous tissue structure around the injured site, where allografted cells undergo cell death or be engulfed by resident cells. How MSCs exert their plerosis and immunoregulatory effects have been intensively studied. In the skin incison, the supernatant of cultured MSCs not only enhanced the function of keratinocytes and endothelial cells, but also attracted macrophages into wound healing process.41 Considering that the paracrine function of MSCs plays a major role in tissue repair, there is a renewed interest in the components and molecular basis of MSCs secretion involved in the interaction between allogeneic cells and the tissue microenvironment.
Secretion is central to MSC-based therapy
Our early studies demonstrated an indispensable role of soluble factors in the immunosuppressive functions of MSCs.42 Of note, intrathecal injection of MSCs showed high efficacy than intravenous administration in treating multiple sclerosis, indicating that cells delivered in closer proximity to the damaged areas could bring a higher proportion of trophic factors and immunomodulatory molecules to the lesion sites in central nervous system.43 Numerous studies have indicated the paracrine actions of MSCs in treating diseases (Table 2). MSCs-generated signaling molecules can be isolated and enriched as cell-free products in clinical translation. Apart from the essential role of bioactive fractions released by MSCs in modulating the intrinsic tissue repair process, MSCs also express a wide array of chemokines and receptors to form a subtle chemotactic network in vivo for guiding circulating cells to the injury sites, or mobilizing immune cells in inflammatory tissues.44 Importantly, the tissue remodeling process mediated by MSCs cannot be attributed to a single effector, but the combined regulation of various factors to maintain homeostasis. A deeper understanding of the secretion function of MSCs in both physiological and pathological conditions is necessary for designing more effective and safe treatment strategies.
Variability of the secretion profiles
Orchestration by inflammatory signals
There are various types of inflammatory factors in the process of tissue damage, repair, and remodeling along with disease progression, these factors are indispensable for boosting the reaction of MSCs. One of the innate responses to acute injury is the formation of a relatively hypoxic microenvironment in situ, which is resulted from the increase in oxygen demand of infiltrated cells and the high metabolic rate, coupled with the vasoconstriction caused by inflammatory stimuli.45 Hypoxia rapidly upregulates the level of ICAM-1 in inflamed sites (such as the endothelium) via hypoxia-inducible factor 1α(HIF1α)46 and ICAM-1 could remarkably promote MSC migration to inflamed tissues.47 Also, the paracrine property of MSCs to release chemotactic and angiogenic factors is significantly amplified under hypoxic condition.48
Given that the MSCs stimulated by interferon-γ (IFNγ) and tumor necrosis factor-α (TNFα) or IL-1 exhibited greater immunosuppressive capacity by upregulating the expression of ICAM-1 and vascular cell adhesion molecule-1(VCAM-1) both in vitro and in vivo,49 the inflammatory environment is pivotal in shaping the regulatory role of MSCs. During inflammation, the M1 macrophages or T helper cell type 1 (Th1) lymphocytes secrete high levels of proinflammatory cytokines, which confer MSCs dramatic immunomodulatory ability.50 We found that inflammation primed-MSCs secreted a series of chemokines to attract immune cells (Fig. 2), and produced inducible nitric oxide synthase (iNOS) in rodents or indoelmine-2–3-dixoygenase (IDO) in other mammalian species to suppress T cell responsiveness.51,52 Regarding proliferation, the activated lymphocytes and MSCs are mutually inhibitory in co-culture.42 Although the differentiation capacities and immune regulatory functions of individual MSC clones are heterogeneous, priming MSCs with pro-inflammatory agents uniformly amplified their inhibitory effects on T cell response and eliminated the difference in the suppressive extent among different MSC clones.53 The inflammatory signals polarize MSCs towards an anti-inflammatory and pro-trophic phenotype for tissue recovery.54 In turn, the factors released from MSCs promote the remodeling of damaged tissue microenvironment.52

Supernatant of anti-CD3-activated splenocytes increased the gene expression of chemotactic factors in MSCs. a Fold increase of gene expression in the MSCs treated with supernatant from anti-CD3-activated splenocytes, relative to the ones treated by supernatant from naive splenocytes. b Heatmap for log value of chemotactic genes expression in MSCs. (Modified from Ren et al., Cell Stem Cell, 2008)
Hyper-inflammation endows MSCs with unique regulatory functions, while low doses of inflammatory cytokines could hardly elicit such a response or even cause an opposite effect. High levels of cytokines stimulate MSCs to inhibit immune responses, whereas MSCs activated by the weak stimulus are barely immunosuppressive but still can release chemokines for attracting immune cells.55 The MHC class II expression in MSCs requires stimulation by a low dose of IFNγ, which endows MSCs with antigen-presentation effect to enhance T cell-mediated immune response.56,57 When the IFNγ levels increase to a level higher than 25 pg/ml, MSCs become immune-suppressive with diminished antigen-presentation cell (APC) function.56 Signal transducer and activator of transcription (STAT) 1 and STAT3 are both activated by IFNγ at early stages. Inhibition of mTOR further promotes pSTAT1 nuclear translocation and strengthens the ability of MSCs to inhibit T cell vitality. However, sustained exposure to IFNγ led to inhibition of STAT3 activity and impaired the capacities of proliferation and differentiation of MSCs.58
Tumor-associated MSCs
MSCs can sense distinct signals from surrounding tissues to adapt to different pathological conditions.59 In comparison with naïve MSCs, tumor resident MSCs produce more chemokines that recruit monocytes/macrophages to the tumor tissue.60 The tumor microenvironment triggers the transformation of MSCs into cancer-associated-MSCs (MSC(CA)s), which in turn polarize monocytes to a pro-tumoral phenotype.61 Tumor cells, such as those of multiple myeloma, can deliver miR-146a-containing exosomes into MSCs. This microRNA has been shown to elevate the secretion of several cytokines and chemokines in MSCs to support tumor metastasis.62 The acute myeloid leukemia (AML) cells highly expressed macrophage migration inhibitory factor (MIF) to activate its receptor CD74 on MSC(BM)s and thereby promoted MSC(BM)s to secrete IL-8 to support tumor cells survival.63 MSC(BM)s can also express periostin to increase the C-C motif chemokine ligand (CCL)2 expression in acute lymphoblastic leukemia (ALL) cells, which conversely upregulates periostin expression in MSC(BM)s and contribute to leukemia progression.64 Thus, there is a crosstalk between MSCs and the surrounding factors in the tumor microenvironment.
Despite that MSCs are reported to promote survival of cancer cells,65,66,67 discerning the specific role of MSCs in tumorigenesis is critically needed for targeted cancer therapy. MSC(CA)s support the growth and invasion potential of cancer cells through secreting cytokine GM-CSF, providing a novel cytokine pathway for therapeutic intervention.68 During traditional ROS-inducing chemotherapies for ALL, MSC(BM)s from patients could be activated by cytarabine and rescue the stressed cancer cells through mitochondrial transfer. Thus, steroids and microtubule inhibitors can be exploited to improve the therapeutic strategies for ALL, by preventing MSC activation and disrupting microtube formation respectively.69 In another study, promyelocytic leukemia gene expression in MSCs was found to play an essential role in generating pro-inflammatory cytokines and soluble factors, which are crucial to the persistence of leukemic cells in patients with chemotherapy resistance.70 C-X-C motif chemokine ligand (CXCL)12-expressing MSC(BM)s are also important for retaining quiescence leukemic stem cells (LSCs), while MSC-specific deletion of CXCL12 makes LSCs become more sensitive to tyrosine kinase inhibitors, although at the risk of leukemic cell expansion.71 On the other hand, survival of leukemia-bearing mice could be prolonged by intra-BM transfusion of MSC(BM)s from healthy mice. The healthy MSC(BM)s functionally recovered the host MSCs and reprogrammed the host macrophages in BM to execute the tissue repair function.34 These investigations strongly suggest that targeting MSCs in tumors may overcome major obstacles of drug resistance and disease recurrence.
Context-dependent efficacy of MSC therapies
The recognition of the paracrine mode of MSCs opens a new venue for understanding the cellular mechanisms of MSC therapies for diverse diseases. It was reported that toll-like receptor 4 (TLR-4) activated MSCs increased VCAM-1 and ICAM-1 dependent binding of leukocytes, whereas TLR3 stimulated MSCs exhibit enhanced affinity to leukocytes through hyaluronic acid (HA).72 Therefore, specific stimuli are important in provoking the immunomodulatory capacities of MSCs during MSCs-based therapy. As the inflammatory signals always fluctuate with the progression of diseases, various immunosuppressive signals in the tissue microenvironment, including TGFβ and IL-10, as well as the immunosuppressant such as cyclosporin A, have been proven to abrogate MSCs-mediated immunosuppression and to sustain inflammation instead.59 Injection of MSC(AD)s at the peak of experimental autoimmune encephalomyelitis (EAE) produced more satisfactory effects than those injected during the regression phase.73 Moreover, a clinical trial of autologous MSC transplantation yielded improved clinical scores in multiple sclerosis patients with active disease progression.43 The use of steroids may complicate the therapeutic effect of MSCs. Steroids disrupt STAT1-mediated expression of IDO and iNOS and therefore may cause a dose-dependent reversion of MSCs mediated-T cell suppression without affecting the chemokines induction.74
Additionally, the secretion spectrum of MSCs is not only influenced by diverse exogenous stimuli, but also by the status of MSCs themselves. MSC(AD)s have a higher immunomodulatory capacity than MSC(BM)s at equal cell numbers, at least partly because of higher expressions of TGFβ than MSC(BM)s with their vigorous metabolic activity.75 The mitochondria of MSC(AD)s from atherosclerotic patients possess a higher level of reactive oxygen species and altered secretion profile, leading to an impaired immunosuppressive capacity.76 In the organoid model of alveolospheres, aged lung MSCs have higher levels of NADPH oxidase 4(NOX4) to produce oxidants and acquire senescence-associated secretory phenotype, so that they lose the normal 3D structure with type 2 alveolar epithelial cells.77 The senescent MSCs appeared to be less potent in tissue protection than the young ones, due to insufficient production of growth factors and chemokines.78 Therefore, senescent MSCs deploy a more blunted secreting response to the activated immune cells compared to young MSCs, but IFNγ could partly restore the immunosuppressive deficiency of senescent ones.79
Collectively, these discoveries suggest that MSCs are highly plastic in their secretion spectrum. The context of pathological status in vivo and MSCs-produced mediators vary dependently and thus result in heterogeneous immunoregulatory functions, which could partly explain why clinical trials of MSC applications have produced ambiguous outcomes.80 Thus, it is essential to tailor MSCs secretion to meet the context-specific needs.
Major factors released by MSCs
The secretory profiles of MSCs encompass a variety of biologically active ingredients. A large portion of bioactive factors is packaged by vesicles for external transmission. Most molecules are discharged outside the cell through the classical exocytosis fusion mechanism, while the other transportation involves direct membrane translocation of proteins.40 In fact, there are few reports about the mechanisms of intracellular molecule assembly and transmembrane transport process in MSCs.
Extracellular vehicles
Generation and actions
One of the most important mechanisms for MSCs to communicate with other cells is through extracellular vesicles (EVs). Exosomes are the smallest subtype of EVs that have been intensively studied. Exosomes generally originate from endosomes, as their membranes are enriched in lipids rafts, which are involved in the fusion and release cascades between intraluminal vesicles (ILV) and multivesicular bodies (MVB).81 The fusion of MVB with the plasma membrane leads to the release of exosomes. Exosomes may subsequently be taken up by other cells via membrane fusion, endocytosis or cell-type-specific phagocytosis.82 Microvesicles (MVs) are slightly larger than exosomes and are formed from plasma membrane budding and fission. TNFα upregulates Fas and Fas-associated phosphate-1(Fap-1) expression via the NF-κB pathway and facilitates the Fas/Fap-1/Caveolin-1 complex transfer to the cell membrane of MSCs derived from the gingiva, promoting membrane fusion to release small EVs in a soluble N-ethylmaleimide-sensitive factor (NSF) attachment protein receptor (SNARE)-dependent manner.83
The nanoscale exosomes can easily shuttle through tissues and biological barriers to transfer microRNAs, lipids, and proteins, thus they have been adapted as therapeutic agents.84 For example, exosomal miR-125b-5p was shown to mediate the therapeutic effects of MSCs in myocardial infarction and ischemic acute kidney injury, it directly downregulated p53 and prevent cell apoptosis through reducing autophagic flux or cell cycle arrest.85,86,87 In practice, the immunoregulatory functions of MSCs partially rely on exosomes, which mediate the MSC-immune cell crosstalk in some pathological conditions. The exosomes from MSC(AD)s inhibit T cell proliferation, differentiation, and activation as well.88 MSC-derived exosomes were shown to ameliorate the pathological changes of experimental autoimmune uveoretinitis by preventing the accumulation of inflammatory cells (CD4+T cells, neutrophils, NK cells, and macrophages) around the eyes and reducing the percentage of CD4+IFN-γ+ and CD4+IL-17+ cells in the retina, without inhibiting proliferation of IRBP-specific T cells.89 The mitochondria of donor MSCs, carried by EVs, can be transferred to neighboring macrophages to enhance oxidative phosphorylation, consequently achieving an anti-inflammatory and highly phagocytic macrophage phenotype.90 MSC(AD)s transferred the exosomes loaded with active STAT3 into macrophages and polarized them towards the anti-inflammatory M2 phenotype through the transactivation of arginase-1. These M2 macrophages reversely promoted MSC(AD) proliferation and lactate production, thus facilitating metabolic activity and resistance to obesity progression.91 Exosomal miR-182 delivery from MSCs to macrophages directly downregulates TLR-4 to confer M2 phenotype, contributing to the therapeutic effects of exosomes on myocardial ischemia/reperfusion injury.92 Moreover, MSC-derived MVs also enhanced monocyte phagocytosis of bacteria in severe pneumonia and ameliorated inflammation in injured alveolar epithelium.93 Notably, EVs can attach to the extracellular matrix (ECM), and the soluble factors released from EVs can also attach to ECM or directly act on adjacent target cells. Intravitreal injection of MSC-derived EVs significantly enhanced functional recovery, and decreased neuroinflammation and apoptosis in retinal ischemia.94 The MSC-EVs could bind to vitreous humor components and persist in the vitreous humor for a long time to provide sustainable protection.94 The therapeutic efficacy of MSC-derived exosomes in retinal degeneration models was long-lasting, as the protective effects on photoreceptors and retina could be detected even months after a single injection.95
EV-based therapeutics
EVs have emerged as a rising therapeutic paradigm for cell-free MSC-based therapies. Clinical study has shown that the use of MSC-EVs led to significant improvement in GvHD symptoms, remarkably reducing the dosage of steroids.96 MSC-EVs induced polarization of M2 macrophages to dampen inflammatory response in damaged tissue sites, thereby promoting tissue remodeling in diabetic wounds.97 The MSC-EVs were also reported to ameliorate lung injury90 and decelerate renal fibrosis via modulating the phenotype and function of infiltrated macrophages.98 MSC-EVs act as efficiently as MSCs in treating various degenerative diseases and immune dysfunctions, while EVs bypass a series of drawbacks of direct cell infusion. The therapeutic efficacy of human MSCs can be reproduced by the administration of their autologous exosomes.99 Moreover, genetic engineering modified MSC-derived exosomes can act as ‘Trojan horses’ to target the tumor microenvironment and strengthen tumor immunotherapy.100 Such exosomes are constructed to carry galectin-9 siRNA and oxaliplatin pro-drug. More importantly, in sharp contrast to native MSCs, their EVs do not cause undesired immune responses due to fewer stimulatory HLA-complex molecules and surface co-stimulators.101,102 In COVID-19 treatment, MSCs administration may potentially cause coagulopathy, which synergizes with COVID-19 pneumonia and deteriorates the patients’ condition. In comparison, low immunogenic exosome delivery can avoid this side effect.103
However, how to make EV-based therapies more practical and effective in disease treatment is an urgent issue in the clinical application of MSCs. EVs from different origins of MSCs may have conflicting effects, as the exosomes released by MSCs of Langerhans islets in non-obese diabetic (NOD) mice have been shown to be highly immunostimulatory and able to trigger autoimmune response.104 Different isolation methods determine the yield and purity of exosomes.105 Distinct culture conditions, such as oxygen concentration and culture matrix, also influence the functional properties of EVs. Exosomes derived from MSCs preconditioned with hypoxia conditions possess greater therapeutic effects on bone fracture healing. In this scenario, the activation of HIF-1α increased exosomal miR-126 abundance, consequently promoting the proliferation, angiogenesis, and migration of endothelial cells through the SPRED1/Ras/Erk signaling pathway.106 Certain biomaterials combined with EVs can reinforce stem cell-based tissue repair. MSC-derived exosomes loaded in a 3D printed cartilage ECM/gelatin methacrylate bio-scaffold have improved osteoarthritis therapeutic efficacy.107 The EV-based therapy may provide a new venue for the treatment of diseases, but the variability in the contents of EVs due to harvest procedures and cell sources may complicate their clinical applications.
Chemokines and receptors
MSCs homing
Like leukocytes, MSCs can fully transverse the vascular endothelium, a process that can be significantly enhanced by the presence of CXCL9, CXCL16, CCL20, and CCL25.108 MSCs harness the network of multiple chemotactic factors to access specific locations and further facilitate tissue remodeling in situ. In this review, we distill the recent studies about the intercellular activities mediated by the wide set of chemotaxis (Table 3). Among these chemotactic gradients, CXCL12(SDF1) is the most prominent one for accumulating stem cells in the BM. The CXCL12/ C-X-C motif chemokine receptor (CXCR)4 axis is essential for MSCs migration, homing, and engraftment in BM stroma,109 and is vital for sustaining the function and development of other precursor cells in tissues. For instance, MSCs modulate the self-renewal and the growth of cardiac cKit+ cells via the CXCL12/CXCR4 pathway.110 Intrinsic expression of CXCR4 is required for the differentiation of lymphoid precursors and their positioning adjacent to the mesenchymal progenitors in the BM, whereas CXCL12 deletion causes a decrease in natural HSCs and expansion of abnormal HSCs.3 CXCL12 is one of the target genes of HIF-1α, which is rapidly upregulated by ischemia or reduced oxygen tissue tension in the initial stage of acute injury. The mobilization of MSCs could be propagated by the hypoxic conditions through induction of the CXCL12–CXCR4 axis.111 Moreover, the chemotactic function of CXCL12 could be augmented by many priming agents such as complement components112 (C1q) and bioactive lipids113 (sphingosine-1 phosphate, or ceramide-1 phosphate). TNFα signal also stimulates MSC migration towards the inflammatory site in a dose-dependent manner.114 Therefore, the bioactive gradients released from damaged tissue amplify and shape the chemokine network of MSCs.
Actions on immune cells
The decisive roles of chemokines and receptors expressed by MSCs in cell mobilization have been extensively investigated. Additionally, they are also defined as the driving force to regulate the migration of immune cells, so that MSCs functionally foster the immune response to maintain homeostasis in the body. As illustrated earlier, MSC(BM)s secrete CCL2 in response to TLR ligands or bacterial infection to induce monocyte emigration to the circulation, thereby enhancing resistance to bacterial infections.115 The chemotaxis mediated by cues from MSCs assists in recruiting T cells for Fas ligand (FasL)-mediated apoptosis and diminishing excessive inflammatory reactions in treating autoimmune disorders, such as systemic sclerosis and colitis.116 The chemotactic gradients have a short half-live and undergo degradation by extracellular proteases. Unlike the neurotoxicity of cleaved-CXCL12 fragments,117 the proteolytic processing of CCL2 by matrix metalloproteinase (MMP) generates an antagonistic derivative that inhibits the activity of CD4+Th17 cells.118 Thus, MSC-derived CCL2 inhibits CD4+ T cell activation by suppressing STAT3 phosphorylation and reversing symptomatic neuroinflammation in experimental autoimmune EAE.118 Moreover, blockade of CXCR3 or C–C motif chemokine receptor (CCR)5 abolished the MSCs-induced immunological suppression of lymphocytes.51 The upregulated CCL5 from irradiated MSCs, as a result of the activation of the cGAS-STING signaling pathway, is responsible for increasing tumor metastasis in mice, by recruiting macrophages to the lung.119 Importantly, MSC-mediated immunosuppression in vivo is closely associated with the polarization of tissue-resident macrophages to the anti-inflammatory phenotype. Different from the direct signaling pathway mediated by other immunoregulatory factors, MSC-derived CCL2 requires heterodimerization with CXCL12 to synergistically polarize macrophages via CCR2.120 The heterodimerization occurs between members of CXC and CC subfamilies and dramatically alters responsive cell functionality other than mere chemotaxis.120,121 The studies above indicate the requirement of chemotactic gradients in MSC-mediated immunoregulatory effects, but the role of chemokines goes well beyond these effects. MSCs release C-X3-C motif chemokine ligand 1 (CX3CL1) to target the C-X3-C motif chemokine receptor 1(CX3CR1) on microglia to control their activation and phagocytosis.122 The CX3CR1+ microglia are functionally enhanced by an MSC-driven increase in intracellular calcium concentration and display enhanced phagocytotic activity in swallowing axon fragments or apoptotic cell bodies. As expected, MSCs switch microglia to a neuroprotective phenotype and provide a beneficial environment for the regeneration of nerve axons.
Growth factors
A variety of growth factors have been identified among the secretion profile of MSCs, including vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), keratinocyte growth factor (KGF), insulin-like growth factors (IGF-1 and IGF-2), and hepatocyte growth factor (HGF). These growth factors are not only important effector molecules that promote tissue repair but can also regulate the differentiation and function of MSCs themselves. VEGF-C induces the phosphorylation of VEGF receptors (VEGFR2, VEGFR3) and the activation of ERK signaling in MSCs. VEGF-C enables MSCs to acquire enhanced expressions of osteogenic marker genes such as RUNX family transcription factor 2 (RUNX2) and facilitates MSC mineralization.123 When stimulated by bFGF, the HGF expression in MSCs was upregulated through the JNK signaling pathway, contributing to the tissue repair and suppression of fibrogenesis.124
Pro-and anti-angiogenesis
The superiority of MSCs in promoting wound healing mainly results from a series of mitogenic and vascular trophic factors, including angiogenic factors to restore the blood supply in ischemia tissues.125 It has been confirmed that growth factors (VEGF, HGF, and IGF-1) are rich in MSC culture medium (MSC-CM) and provide a renal protective effect in acute kidney injury after MSCs infusion.126 We reported that MSCs treated with TNFα and IFNγ could secret a large amount of VEGF-C that accelerates wound closure through promoting angiogenesis.127 Nevertheless, the MSCs-mediated therapeutic effect does not always result from angiogenesis. We found that human MSC(AD)s could effectively inhibit neovascularization and reduce the opacification of ethanol-injured cornea via promoting the clearance of neutrophils during the granulation stage.128 Likewise, another study demonstrated that MSCs extracted from corneas and then embedded in fibrin gel for local application prevented corneal neovascularization after corneal injury in mice. These effects were significantly abrogated by knocking down the pigment epithelium-derived factor (PEDF) expression in cornea-derived MSCs (MSC(C)s). Mechanistically, the secretion of anti-angiogenic factors including soluble fms-like tyrosine kinase receptor (sFLT)-1 and PEDF in MSC(C)s attenuated the injury-triggered angiogenesis.129
Tissue remodeling
MSC-EVs improve the survival of animals with experimental lung injury in part through the secretion of KGF93 and HGF,130 which is associated with decreased endothelial permeability and protection of cell growth. Mass spectrometry analysis showed that the milk fat globule-EGF factor 8 (MFGE8) secreted by MSCs strongly inhibited hepatic stellate cells and thus prevented liver fibrosis.131 Of note, HGF is a crucial factor in MSC-mediated protective effects in chronic inflammatory disease models. HGF does not only prevent epithelial cells from apoptosis but also exhibits anti-fibrotic effects in the experimental fibrosis model.132 Moreover, HGF contributes to MSC-mediated functional recovery in the animal model of multiple sclerosis133 and Alzheimer’s disease.134 HGF inhibits hyperphosphorylation of tau protein and rescues the cytoskeleton branches of damaged neurons, suggesting that MSCs-derived HGF may be the key factor for endogenous neurogenesis and cognition improvement in Alzheimer’s patients.134 It is worth noting that some of the growth factors secreted by MSCs support their immunoregulatory ability as well. IFNγ induces MSCs to produce flt3-ligand through the JAK/STAT signaling pathway, which binds to flt3 on CD1c+ dendritic cells (DCs) to promote the survival of tolerogenic CD1c+DCs in SLE.135 IGF-2, another important growth factor, is highly expressed in MSCs exposed to low oxygen and in muscle stem cells (MuSCs) and exhibits potent anti-inflammatory properties.136 IGF-2 administered to EAE mice preprogrammed maturing macrophages to acquire an anti-inflammatory property.137 It instructed maturing macrophages to undergo oxidative phosphorylation and to highly express programmed death-ligand 1 (PD-L1).136 However, modulation of macrophages by MSCs-derived growth factors cannot achieve the desired outcome all along. As mentioned before, PEDF is a pleiotropic protein in possession of anti-angiogenic, anti-oxidant, anti-tumor, and neuroprotective properties.138 PEDF interferes with macrophage infiltration and activation in the injury site, leading to a delayed remodeling process.139 Therefore, MSCs that highly express PEDF counteract the therapeutic actions and eventually give rise to more cardiac fibroblasts with impaired angiogenesis in the myocardial infarction region.139
Inflammatory cytokines
Supporting cell differentiation and survival
MSCs are reported to produce a variety of factors to support the differentiation of CD34+ hematopoietic progenitors,140,141 including the cytokine IL-6. MSCs are critical for the maturation of human antibody-secreting cells (ASCs), and IL-6 is the crucial component to support the survival and secretory function of ASCs.142 Our previous study has shown that IL-6 derived from MSCs mediated the protective effect against the spontaneous death of splenocytes in vitro.143 Another report revealed that MSC(BM)s induced the proliferation of colitogenic CD4+ memory T cells via secreting IL-7 and played a pathogenic role in inflammatory bowel disease (IBD).144 IL-7 is an indispensable cytokine that contributes to B cell development, deprivation of IL-7 in MSC(BM)s reduced the tendency to differentiate into B cells of lymphoid progenitors.3 Moreover, LPS-triggered MSCs selectively recruit neutrophils through the secretion of IL-8 and macrophage migration inhibitory factor (MIF) to strengthen the function and survival of neutrophils.145,146 Considering the pro-survival property of MSCs for immune cells, the activated MSCs might boost immune responses in the injured site or exacerbate tissue necrosis under particular circumstances.147 Meanwhile, MSCs-derived IL-28 can trigger prostate cancer cells to undergo apoptosis, despite that IL-28 insensitive cancer cells eventually evolve in the BM.148 We recently showed that C3 produced by lung MSCs can promote the formation of neutrophil extracellular traps in establishing a pre-metastatic lung microenvironment. Interestingly, the C3 production by MSCs is stimulated by Th2 cytokines.149 Hence, the secreted factors by MSCs may serve as the essential signals to remodel the tumor microenvironment.
Immunoregulation and tissue remodeling
MSCs exert their immunomodulatory effects by interacting with both the innate and adaptive immune cells. MSCs reduce the expression of MHC II, CD40 and CD86 costimulatory molecules on mature DCs, as well as inhibiting the maturation of cultured DCs partially through an IL-6-dependent mechanism, thus inhibiting T-cell proliferation.150 Multiple cytokines are involved in the immunoregulatory functions of MSCs, including HLA-G151 and LIF.152 Splenocytes treated with MSC-CM produce large amounts of IL-10,153 which is an essential cytokine to induce MSCs to secrete soluble isoform of HLA-G5 to suppress innate immunity.154
MSCs usually perform their therapeutic function through balancing proinflammatory and anti-inflammatory responses, which are generally mediated by the suppression of excessive Th1 responses and the switch toward Th2 type. Interleukin-1 receptor antagonist (IL-1Ra) produced by MSCs is reported to alter the inflammatory and fibrotic response during chronic lung injury.155 IL-1Ra also can induce macrophage polarization from the M1 to M2 phenotype and accelerate wound healing.156,157 MSCs secreted IL-4 to polarize microglia towards the anti-inflammatory phenotype with enhanced phagocytic ability to clear extracellular α-synuclein, indicating a neuroprotective role in parkinsonian disorder.158 As to airway hypersensitivity mediated by uncontrolled Th2 response during asthma, MSCs diminish the content of Th2 cytokines (IL-4, IL-5, and IL-13) in bronchial lavage and Th2 type immunoglobulins in serum, through increased production of TGF-β in the activated STAT6 pathway.159 TGF-β in MSC-CM mediates most suppressive effects, especially for inducing regulatory T cells and inhibiting adaptive immune reactions.160 In LPS-stimulated microglia, TGF-β impedes their polarization to the M1 phenotype by inhibiting NF-κB signaling and restores their CX3CR1 expression, which endows them with enhanced phagocytosis of apoptotic debris.161 However, autocrine TGF-β in MSCs would restrict the immunosuppressive effect of MSCs via inhibiting their iNOS expression in a SMAD3-dependent manner.162
ECM components
MSCs express various components of ECM, including vimentin, galectins, integrin, and collagens.163,164,165 The ECM molecules produced by MSCs are likely to support the formation and stabilization of vessels, as well as to provide ECM-associated bioactive factors.166 Upon the osteogenic stimuli, MSC(BM)s cultivated on collagen matrices showed decreased MMP expression along with increased tissue inhibitors of metalloproteinase (TIMPs), while the expression profile became exactly the opposite when they are subjected to adipogenic conditions.167 The conversion of native collagen to denatured collagen IV by MMPs is proven to switch the lineage commitment of MSCs to adipogenic differentiation.168 Follistatin-like protein 1 (FSTL1), a glycoprotein that has been found to mediate pro-inflammatory events, is closely correlated with chondrogenesis of MSCs, which is reflected in the production of ECM proteoglycans and collagen II.169
The change of ECM expression in differentiated MSCs provides a narrow window for researchers to gain insight into the communication between ECM and immune response. During the process of tissue injury and repair, chronic inflammation is always associated with aberrant ECM deposition, and the fragments of ECM may activate immune cells and support their survival during the tissue-remodeling processes.170 The crucial role of the ECM for adhesion and migration of inflammatory cells has been well established, which involves the HA receptor CD44 expressed by the leukocytes. The TLR3-activated MSCs strongly increased the affinity of leukocytes to MSCs through the formation of cable-like HA structures, in which the immune-suppressive activity was partially mediated by prostaglandins.72 In fact, MSCs co-cultured with inflammatory cells is enriched with glycocalyx, which is mainly composed of modified HA matrix, chondroitin sulfate-proteoglycan, and versican.171 These proteoglycans are biological macromolecules that are widely present on cell membrane surfaces and in ECM and possess a highly complex structure consisting of one or more glycosaminoglycans (GAGs) side chains with covalently conjugated core proteins. In spite of the active proteolysis in injury sites and the short life-span of active gradients, the negatively charged GAGs are usually attracted by the highly basic proteins such as chemokines, thus forming a stable structure to avoid chemokine degradation.172 The interaction of chemokines and GAGs is harnessed by MSCs and gives them unique advantages in quickly traversing into the circulation and mobilizing immune cells or other progenitors. As mentioned above, MSCs secreted a multifunctional extracellular component, periostin, to form a mutually reinforcing loop between matrix and B-ALL cells derived-CCL2 and increased leukemia burden.64 Moreover, the stable matrix structure functions as a “cloak” to make MSCs escape from host rejection and survive in xenograft transplantation. High molecular weight HA, but not that with the low molecular weight, was shown to induce IL-10-producing regulatory T cells to suppress responder cell proliferation in both human and murine system.173,174 In addition, MSCs constitutively secrete galectins-1 and galectins-3 that take part in T cell suppression, which also provides convincing evidence for the ECM-dependent mechanism of immunomodulation by MSCs.164 On the other hand, treating MSCs with fibronectin, or laminin could stimulate cell proliferation and migration,175 suggesting that ECM molecules further support the biological functions of MSCs. Tissue-resident HA in the kidney promoted transfused MSCs to localize in the injured renal tissue by binding with CD44 and accelerated functional recovery in an acute renal failure model.176 Such ECM cooperativity allows more MSCs to converge in the injury site through certain chemotaxis pathways, which may enable engineered materials to preserve active chemokines and effectively facilitate tissue repair.177,178
Main pathways of MSC-mediated immunomodulation
The mechanisms that underlie the versatile immunomodulatory function of MSCs are widely described. Here, we distill some important regulatory factors that define the interface between MSCs and immune responses.
The iNOS-NO axis
iNOS can be induced by inflammatory cytokines and is a dominant enzyme mediating the immunoregulatory effects of MSCs from rodents (such as mouse, rat, hamster, and rabbit), while MSCs from other mammalian species (such as monkey, pig, dog, cattle, and human) preferentially use IDO.179 The murine MSCs express high levels of iNOS upon activation by pro-inflammatory cytokines and produce NO. While IFNγ-induced NO synthesis could diminish T cell proliferation,180 inhibition of iNOS abolishes the mouse MSC-mediated anti-proliferative effect on T cells.181 Recently, we have found that the SH2 domain-containing phosphatase-1 (SHP1) negatively modulates the iNOS expression in MSCs. SHP1-deficient MSCs have higher levels of JAK1 and STAT3 phosphorylation and produce more iNOS and cyclooxygenase 2 (COX2), which endow MSCs more immunosuppressive ability in alleviating liver injury.182 NO may coordinate with phosphorylated STAT3 to increase PD-L1 expression in IL-17-stimulated MSCs. Thus, the IL-17 pretreated MSCs acquire more potent immunosuppressive capacity, an effect likely attributed to IL-17 modulated mRNA stability through degrading ARE/poly(U)-binding/degradation factor 1 (AUF1).183 However, NO is very labile and rapidly lost through oxidation. Therefore, T cells have to be attracted in close proximity to MSCs by chemokines and be restrained by adhesion molecules such as ICAM-1 and VCAM-1.51 During the progression of tuberculosis, the pathogen recruits MSCs to the lesion site and induces the production of NO, thereby blunting T-cell responses to help mycobacterium tuberculosis to evade host immune responses.184 The therapeutic efficacy of MSCs was also shown in Coxsackievirus B3 (CVB3)-induced myocarditis, indicating an important role of MSCs in antiviral immunity to blunt the cytotoxic T cell activation in a NO-dependent manner.185 Nevertheless, the NO-mediated immunosuppression by MSCs is likely to switch to an immune-enhancing effect under inadequate stimulus or insufficient inflammation-exposure time. Administration of iNOS inhibitor or genetic ablation of iNOS expression in MSCs could even boost immune reactions because the self-produced chemokines are still attracting immune cells.186 iNOS−/− MSCs enhance immune responses in vitro and in vivo and suppress tumor growth as well.186 In addition, the antifibrotic function of MSCs-derived NO has been proposed. We have revealed that the therapeutic effect of MSCs on liver fibrosis was mediated by the expression of iNOS under inflammatory conditions. iNOS−/− MSCs secreted chemokines but not NO, without any amelioration on the pathological changes in liver fibrotic mice.74 In the experimental model of systemic sclerosis, the iNOS−/− MSCs lost the capacity of eliminating oxidative stress or exerting the anti-fibrotic effect.187
The tryptophan-IDO-kynurenine-aryl hydrocarbon axis
IDO is a rate-limiting enzyme for degrading tryptophan (Trp) to N-formylkynurenine. Apart from the cell–cell contact requirement for MSC to induce T-cell tolerance, the culture medium also inhibits the proliferation of activated T lymphocytes, a paracrine effect that partly depends on the expression of IDO.188 The IDO-mediated conversion of Trp into kynurenine (KYN) induces apoptosis and cell cycle arrest in activated conventional T-cells and promotes the differentiation of regulatory T cells.189 Given that IDO-expressing macrophages suppress T-cell proliferation in vitro by reducing tryptophan concentrations,190 rapid exhaustion of Trp causes the generation of uncharged transfer RNA that subsequently activates the general control nonderepressible 2(GCN2) kinase, which makes T-cells unresponsive and inactive.191 The tryptophan catabolites such as KYN and picolinic acid could also inhibit activated T cells and NK cells in the absence of tryptophan,192 although the addition of tryptophan could restore allogeneic T-cell proliferation.193 As reported, KYN induces FOXP3+ Tregs in an aryl hydrocarbon receptor (AhR)-dependent manner, the binding of kynurenine to the AHR could be further potentiated by TGF-β.194 In human MSCs, we have found that kynurenic acid (KYNA), which is another IDO-derived metabolite with little cytotoxicity and shares the same AhR receptor as KYN, could promote TNFα-stimulated gene-6 (TSG-6) expression due to the augmented binding of AhR to the promoter of TSG-6, thereby alleviating neutrophils infiltration in injured lungs.195 MSCs also require IDO in promoting the differentiation of monocytes into immunosuppressive macrophages to ameliorate inflammatory responses.196 However, KYNA limited IL-10 production via the increase of intracellular cAMP in BM-derived macrophages and predicted poor prognosis in atherosclerosis.197
Human MSCs primarily express IDO upon stimulation with IFNγ together with TNFα or IL-1 to exert the immunosuppressive effects. IFNγ triggers MSCs to express IDO in a STAT1-dependent manner. STAT1 overexpression enhances MSC-mediated T-cell suppression in vitro.198 In addition, the pro-inflammatory stimulation leads to a metabolic shift to glycolysis. Once the glycolytic flux of MSCs is blocked by 2-Deoxy-d-glucose (2-DG) treatment, STAT1 binding to the IFNγ-activated sequence region in the IDO1 promoter is impaired, thereby abolishing IDO upregulation and reducing the inhibition on T cell response.199 As STAT1 phosphorylation could also be inhibited by dexamethasone, the expression of IDO or iNOS by activated MSCs would be blocked by steroids without affecting the production of chemokines.74 Silencing IDO in human MSCs would result in an unexpected boost of immune responses, as the MSCs could facilitate stimulated PBMC proliferation at both low and high cell densities.186 On the contrary, aberrant activation of IDO aggravates tumor evasion and are closely associated with poor clinical prognosis.200 IDO and the downstream metabolites are considered as the important mediators of MSCs to regulate immune cells, their involvement in the aging process also should be taken into account. As mentioned before, continuous inflammatory stimulation induces IDO expression but impedes MSC proliferation and differentiation. Of note, hyperactivity of IDO-mediated tryptophan degradation may be associated with a relative reduction in another metabolic pathway to generate melatonin, which serves as an antioxidant to reverse aging phenotypes of MSCs201 and regulate the multi-lineage differentiation of MSCs.202 KYN was found to be accumulated along with age in the plasma and bone tissue, making the aged mice vulnerable to bone loss and osteoporosis.203 These findings could be related to the observation that KYN inhibited autophagy and induced senescence in MSC(BM)s via AhR signaling.204
The COX2-PGE2 axis
When MSCs were used to treat GvHD, it was found that MSCs displayed potent dose-dependent immunosuppressive effects on lymphocyte responses, an effect mediated by the expression of COX1/COX2 enzymes and the production of PGE2.205 The immunosuppressive role of MSC(BM)s to treat EAE mice was also found to rely on PGE2.206 COX2 is an inducible enzyme that mainly presents on the luminal surface of the endoplasmic reticulum and at the inner and outer membranes of the nuclear envelope.207 COX1, on the other hand, is encoded by a housekeeping gene and is constitutively expressed in most mammalian cells, playing a vital role in regulating renal function and protecting gastric mucosa. COX2/PGE2 axis has been reported as a significant mediator of MSC-mediated immune regulation, which includes programming macrophages plasticity,208 dampening NK cell acitivity,209 and suppressing Th17 differentiation.210 MSCs alleviate allergic inflammation by suppressing degranulation and pro-inflammatory factors production in mast cells in a COX2-dependent manner.211 Importantly, PGE2 preserves the immune privilege of allogeneic MSCs during therapeutic infusion.212 MSCs-derived PGE2 induces CD4+ T cell differentiation into Tregs along with TGFβ1, by means of direct cell-cell contact.160 In an experimental model of liver injury, PGE2 was found to bind to the EP prostanoid receptor 4(EP4) on CD11c+B220− DC precursors and induce their differentiation towards a regulatory phenotype in a PI3K-dependent manner.213 It should be noted that COX2 is also essential for MSC-mediated tissue remodeling, especially to bone repair. COX2 could augment osteogenesis potential and suppress chondrogenic differentiation in mouse skeletal stem cells through the canonical Wnt/β-catenin signaling pathway.214 The COX-2/PGE2 axis plays a key role in facilitating osteogenic differentiation of MSCs in the initial pro-inflammatory phase mediated by M1 macrophages.215 Meanwhile, MSCs-secreted PGE2 acts on macrophages to alter the metabolic status, skewing toward M2 polarization,208 which is more conducive to guiding MSC differentiation and bone regeneration.
Interestingly, it has been found that hyperthermia increases the efficacy of MSC-driven immune-suppression that involves the COX2/PGE2 pathway, which relies on the translocation of heat shock proteins into the nucleus of MSCs.216 It should be noted that fever is a hallmark of inflammation and/or infection and can be triggered by PGE2. The COX2/PGE2 axis somehow acts to lure the inflammatory signals into cells and to activate the immunosuppressive potential of MSCs to a greater extent. For instance, when carcinoma cells-derived IL-1 increased the production of PGE2 in surrounding MSCs, PGE2 acted in concert with IL-1 to induce other cytokines, proceeding to elicit the formation of cancer stem cell niche and to promote tumorigenesis.217 The high amount of TNFα induces COX2 expression and PGE2 production in MSCs, and NO also participates in the upstream induction of COX2.218 Pro-inflammatory stimuli cause rapid expression of COX2 and abundant production of prostaglandins, which preferentially enter the nucleus to exert both stimulatory and inhibitory effects on the activity of NF-κB complexes, thereby promoting a series of inflammation-associated transcription.219 When the promoters of COX2/PTGS2 and prostaglandin E synthase (PTGES) were hypomethylated by DNA methyltransferase inhibitor, elevated production of PGE2 enhanced the immunosuppressive effects of MSCs on colitis mice.220 This COX2-based immunomodulation can also be enhanced in other ways. Phagocytosis of apoptotic cells endows human MSC(UC)s with powerful immunosuppressive capacity, the engulfment of apoptotic cells stimulates MSCs to express COX2 and produce PGE2 through NF-κB signaling so that it further potentiates the immunosuppressive effects of MSCs.221 Unlike IDO, the expression of COX2 in MSC is more variable with cell culture conditions. In vitro, the secretion of PGE2 by MSCs is affected by the content of fetal bovine serum (FBS) in the culture medium. The absence of FBS led to less production of PGE2 and compromised the immunomodulatory properties.222 Although hypoxia enabled MSCs to produce several growth factors and chemokines more efficiently, it accelerates proteasome-mediated degradation of COX2 and decreases PGE2 in MSCs, as well as loss of immune privilege.212 Meanwhile, arachidonic acid along with its other downstream metabolites of COX2, such as PGA2 and PGD2, displayed an inhibitory effect on IFNγ induced IDO expression in monocytes.223 Therefore, the interaction between PGs and the immune system cannot be generalized.
The TNFα-TSG-6 axis
TSG-6, a 277 amino acid glycoprotein secreted by many cells in response to pro-inflammatory factors, confers MSCs with prominent anti-inflammatory properties for treating myocardial infarction,224 peritonitis,225 acute lung injury,226 and corneal injury.227 Both MSCs-secreted TSG-6 and recombinant mouse TSG-6 inhibited the STAT3 signaling pathway and alleviated pathologic changes in ethanol-induced liver injury.228 Our previous study showed that the IDO metabolite, KYNA, could promote TSG-6 expression by inducing the nuclear translocation of AhR and its binding to the promoter of TSG-6.195 The secretion of TSG-6 in MSCs was enhanced by KYNA and the protein-restricted leukocytes extravasation during inflammation.195 Recently, we have found that the presence of IFNγ and TNFα upregulates the expression of 11β-hydroxysteroid dehydrogenase type 1 in MSCs, subsequently augments TSG-6 expression via the canonical NF-κB pathway.229
The anti-inflammatory property of TSG-6 is largely due to its binding with HA fragments and the subsequent diminishment of the inflammatory network. Early in the 1990s, TSG-6 and adhesion receptor CD44 were found to share significant sequence homology, suggesting its possible binding to HA.230 It was later confirmed by structural analysis that the Link module of TSG-6 defines its interaction with HA.231 Furthermore, a part of GAGs also showed affinity to the Link_domain of TSG-6.232,233 It is interesting to note that the binding of Link_TSG-6 with HA is largely dependent on PH.233 The relative hypoxic condition and active metabolic activity of immune cells in the inflammatory sites often lead to the accumulation of metabolites such as lactic acid and contribute to the establishment of an acidic environment, which makes TSG-6 more tendentious to the damaged sites. These findings provide the molecular basis for its action mode in cell-ECM interaction and in cell migration during inflammation. In the course of cell-based therapy, TSG-6 contributes to the formation of the protective glycocalyx matrix in MSCs to circumvent xenograft rejection via the interaction with HA when exposed to inflammation.171 It does not only provide shelter for MSCs from host immune surveillance but also links up HA and GAGs to support the modulatory effects of MSCs. After cell transplantation, the presence of TSG-6 enables MSCs to accurately reach the damaged tissue, most likely because the microenvironment in the injured site stimulates MSCs to release more TSG-6, which may organize the surrounding HA-contained matrix complex for MSC settlement.234 TSG-6 also performs the immunomodulatory function by acting on immune cells. It was shown that TSG-6 inhibited activation of antigen-presenting cells and T cells in a CD44 dependent manner, consequently blocking insulitis within the pancreas and delaying the onset of type 1 diabetes.235 Similarly, TSG-6 reduces the TLR2/NF-κB signaling in resident macrophages in the mouse model of peritonitis through CD44.225 In addition, cell-to-cell contact with M1 macrophages enhanced the TSG-6 paracrine production by MSCs, which become more potent in regulating immune cells.236 Therefore, MSCs rely on TSG-6 to survive in transplantation and to remodel the inflammatory environment.
The inhibitory effects of TSG-6 on leukocytes transversing across vascular endothelium have been extensively investigated.237 Studies by the Darwin Prockop group proved that intraocular injection of recombinant human TSG-6, especially the injections within the first few hours after injury, remarkably prevented neutrophils from infiltrating in injured cornea and protected cornea from opacification and neovascularization.227 In fact, the mechanisms of TSG-6-mediated inhibition of neutrophil migration are more than just binding with HA.238 TSG-6 also modulates chemokine/GAGs interactions and then inhibits leucocytes infiltration to the damaged tissues.239 TSG-6 targets the GAG-binding region of CXCL8 to antagonize its interaction with heparin and prevent CXCL8-mediated neutrophil transmigration.240 High concentrations of TSG-6 could even obstruct the interaction of CXCL8 with its receptor CXCR2, as well as the associated neutrophil chemotaxis.240 TSG-6 provides the binding sites for chemokines, and the Link module of TSG-6 shows high affinities for multiple chemokines through their GAG-binding epitopes, thus disrupting the presentation of interactive chemokines on cell surfaces or their binding to collagen.239,240
Advances in the application of MSC-secreted factors
The cellular and molecular basis of the actions of MSC-derived factors remains to be fully elucidated, while the clinical applications of MSC-based therapy have outpaced our mechanistic understanding of their multitrophic and immunomodulatory properties (Fig. 3).

Schemes of cell/molecule-based therapy in MSCs application. The designed chemokine delivery devices have emerged as a novel approach for stem cell recruitment and tissue regeneration. Another strategy to potentiate MSCs’ secretory actions, is cultivating MSCs under low oxygen or stimulating MSCs with PRP and cytokines. Importantly, MSCs possess a unique chemotactic network to orient their transmission as the cell ark and deliver specific factors on purpose. MSCs encapsulated in biomaterials such as collagen gels or fibrous protein-based gels have increased migrating capacity to converge in damaged tissues. The factors produced by MSCs support the function and development of other cell types, such as HSC in the bone marrow. MSC also serves as a prominent vehicle to carry antibiotics to the deeply infected sites and accelerate tissue repair. The genetically modified MSCs not only achieve more homing capacity to reach target sites but also recruit more immune cells in the tumor environment to elicit an anti-tumor immunity, which bypasses the side effects caused by chemotherapeutic drugs. (Created with BioRender.com)
Enhancement of secretory function
One of the most important steps for optimizing MSCs-based strategies is to stimulate MSC secretion to a greater extent. Researchers have focused on the strategy of cultivating MSCs under specific conditions of near anoxia (0.1% oxygen) to potentiate their secretory actions.48 Also, a few reports showed that combined administration of platelet-rich plasma (PRP) and MSCs was superior in tissue repair, especially for bone healing.241 Apart from the secretory organelles containing growth factors from platelets, this superiority is likely due to the transfer of mitochondria from platelets to MSCs.242 Such transfer could significantly augment the secretion of pro-angiogenic factors so that PRP-stimulated MSCs have improved capacity in accelerating wound healing.
Engineered MSCs
Considering the context of pathological conditions and MSCs secretion, another option is to design cell/molecule-specific therapeutic schemes. A variety of chemokine delivery devices have emerged as a novel approach for stem cell recruitment and tissue regeneration. The designed protease-resistant chemokine CXCL12 is proven to potentiate the recruitment of CXCR4+/c-Kit+ stem cells and protect the myocardial function.243 The delivery of engineered alginate microparticles that contain CCL2 and VEGF is adapted for therapeutic vascularization in ischemic disease.244 These elements contained in biomaterials for tissue regeneration require far lower doses than the administration of unpackaged molecules. However, single agents cannot substitute all the secretory advantages of MSCs. MSCs possess a unique chemotactic network to orient their transmission as a cell ark and build positive feedback with the cells in situ. They could tactfully avoid immune rejection triggered by artificial materials, or the drug toxicity that comes from traditional pharmacological administration, so researchers are trying to take advantage of these characteristics to maximize the therapeutic potential of MSCs. It has been proven that lentiviral transduced human MSCs could persistently deliver therapeutic enzymes in vivo without affecting their trafficking ability.245 Silencing the gene of prolyl hydroxylase 2 (PHD2) enhances the paracrine effects of MSC(BM)s so that the modified MSCs possess a stronger ability to alleviate inflammation in necrotizing enterocolitis rats.246 Furthermore, engineered MSCs could serve as a prominent vehicle to carry bioactive reagents or to arise specific cellular activity on purpose. For example, translation of genetically modified MSCs that expressed α4 integrin (CD49d) achieved more bone homing in an immunocompetent mouse model, and successfully formed osteoblasts and osteocytes. The strategy may broadly benefit targeted therapies for osteoporosis.165 The genetically modified MSCs that highly express PEDF provide a more satisfactory outcome in preventing lung carcinoma progression.247 The MSCs that deliver CXCL9 and OX40 ligand, as well as the CCL19-expressing MSCs, could increase the infiltration of CCR7+ DCs, CD8+ T cells, and NK cells in tumor sites to elicit their anti-tumor effects.248,249 Additionally, MSC(BM)s could internalize antibiotics such as ciprofloxacin (CPX) and then release CPX to inhibit bacterial activity. Combined with the migration tendency of these cells toward the injury sites, MSCs may serve as an ideal antibiotic delivery system to convey a higher amount of antibiotics to deep infection sites.250 MSCs as efficient vehicles to deliver bioactive agents to the target tissues merit further exploration.
Conclusion
MSCs are powerful bioactive agents for treating various diseases, especially for refractory immune disorders, tissue degeneration, or tissue damage, mainly through their paracrine actions. Investigations of the mediators synthesized by MSCs under various conditions should provide a better understanding of their immunoregulatory function and repair capability.
References
Phinney, D. G. Building a consensus regarding the nature and origin of mesenchymal stem cells. J. Cell. Biochem. Suppl. 38, 7–12 (2002).
Hu, X. et al. Identification of a common mesenchymal stromal progenitor for the adult haematopoietic niche. Nat. Commun. 7, 13095 (2016).
Cordeiro Gomes, A. et al. Hematopoietic stem cell niches produce lineage-instructive signals to control multipotent progenitor differentiation. Immunity 45, 1219–1231 (2016).
Méndez-Ferrer, S. et al. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature 466, 829–834 (2010).
Del Toro, R. et al. Nestin(+) cells direct inflammatory cell migration in atherosclerosis. Nat. Commun. 7, 12706 (2016).
Bianco, P., Riminucci, M., Gronthos, S. & Robey, P. G. Bone marrow stromal stem cells: nature, biology, and potential applications. Stem Cells 19, 180–192 (2001).
Fleming, J. E. Jr., Haynesworth, S. E., Cassiede, P., Baber, M. A. & Caplan, A. I. Monoclonal antibody against adult marrow-derived mesenchymal stem cells recognizes developing vasculature in embryonic human skin. Dev. Dyn. 212, 119–132 (1998).
Crisan, M. et al. A perivascular origin for mesenchymal stem cells in multiple human organs. Cell Stem Cell 3, 301–313 (2008).
Shi, S. & Gronthos, S. Perivascular niche of postnatal mesenchymal stem cells in human bone marrow and dental pulp. J. Bone Miner. Res. 18, 696–704 (2003).
Alexander, N. et al. Stromal cells cultivated from the choroid of human eyes display a mesenchymal stromal cell (MSC) phenotype and inhibit the proliferation of choroidal vascular endothelial cells in vitro. Exp. Eye Res. 200, 108201 (2020).
Takashima, Y. et al. Neuroepithelial cells supply an initial transient wave of MSC differentiation. Cell 129, 1377–1388 (2007).
da Silva Meirelles, L., Chagastelles, P. C. & Nardi, N. B. Mesenchymal stem cells reside in virtually all post-natal organs and tissues. J. Cell. Sci. 119, 2204–2213 (2006).
Dominici, M. et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 8, 315–317 (2006).
Covas, D. T. et al. Multipotent mesenchymal stromal cells obtained from diverse human tissues share functional properties and gene-expression profile with CD146+ perivascular cells and fibroblasts. Exp. Hematol. 36, 642–654 (2008).
Camilleri, E. T. et al. Identification and validation of multiple cell surface markers of clinical-grade adipose-derived mesenchymal stromal cells as novel release criteria for good manufacturing practice-compliant production. Stem Cell Res. Ther. 7, 107 (2016).
Viswanathan, S. et al. Consensus International Council for Commonality in Blood Banking Automation-International Society for Cell & Gene Therapy statement on standard nomenclature abbreviations for the tissue of origin of mesenchymal stromal cells. Cytotherapy 23, 1060–1063 (2021).
Petters, O. et al. Single-stage preparation of human cartilage grafts generated from bone marrow-derived CD271(+) mononuclear cells. Stem Cells Dev. 27, 545–555 (2018).
Lv, F. J., Tuan, R. S., Cheung, K. M. & Leung, V. Y. Concise review: the surface markers and identity of human mesenchymal stem cells. Stem Cells 32, 1408–1419 (2014).
Merrick, D. et al. Identification of a mesenchymal progenitor cell hierarchy in adipose tissue. Science 364, eaav2501 (2019).
Buechler, M. B. et al. Cross-tissue organization of the fibroblast lineage. Nature 593, 575–579 (2021).
Strioga, M., Viswanathan, S., Darinskas, A., Slaby, O. & Michalek, J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev. 21, 2724–2752 (2012).
Baksh, D., Yao, R. & Tuan, R. S. Comparison of proliferative and multilineage differentiation potential of human mesenchymal stem cells derived from umbilical cord and bone marrow. Stem Cells 25, 1384–1392 (2007).
Li, X. et al. Umbilical cord tissue-derived mesenchymal stem cells induce T lymphocyte apoptosis and cell cycle arrest by expression of indoleamine 2, 3-dioxygenase. Stem Cells Int. 2016, 7495135 (2016).
Qian, H., Le Blanc, K. & Sigvardsson, M. Primary mesenchymal stem and progenitor cells from bone marrow lack expression of CD44 protein. J. Biol. Chem. 287, 25795–25807 (2012).
Kawamura, H. et al. TGF-β signaling accelerates senescence of human bone-derived CD271 and SSEA-4 double-positive mesenchymal stromal cells. Stem Cell Rep. 10, 920–932 (2018).
Han, B. et al. In vitro expansion and characterization of mesenchymal stromal cells from peritoneal dialysis effluent in a human protein medium. Stem Cells Int. 2018, 5868745 (2018).
Battula, V. L. et al. Isolation of functionally distinct mesenchymal stem cell subsets using antibodies against CD56, CD271, and mesenchymal stem cell antigen-1. Haematologica 94, 173–184 (2009).
Rashed, S. et al. Differentiation potential of nestin (+) and nestin (-) cells derived from human bone marrow mesenchymal stem cells into functional insulin producing cells. Int. J. Mol. Cell Med. 8, 1–13 (2019).
Barilani, M. et al. Low-affinity nerve growth factor receptor (CD271) heterogeneous expression in adult and fetal mesenchymal stromal cells. Sci. Rep. 8, 9321 (2018).
Picke, A. K. et al. Thy-1 (CD90) promotes bone formation and protects against obesity. Sci. Transl. Med. 10, eaao6806 (2018).
Lu, M. et al. Lipocalin produced by myelofibrosis cells affects the fate of both hematopoietic and marrow microenvironmental cells. Blood 126, 972–982 (2015).
Dorshkind, K. & Landreth, K. S. Regulation of B cell differentiation by bone marrow stromal cells. Int. J. Cell Cloning 10, 12–17 (1992).
Welch, P. A., Burrows, P. D., Namen, A., Gillis, S. & Cooper, M. D. Bone marrow stromal cells and interleukin-7 induce coordinate expression of the BP-1/6C3 antigen and pre-B cell growth. Int. Immunol. 2, 697–705 (1990).
Xia, C. et al. Mesenchymal stem cells suppress leukemia via macrophage-mediated functional restoration of bone marrow microenvironment. Leukemia 34, 2375–2383 (2020).
Bartholomew, A. et al. Mesenchymal stem cells suppress lymphocyte proliferation in vitro and prolong skin graft survival in vivo. Exp. Hematol. 30, 42–48 (2002).
Bruder, S. P. et al. Bone regeneration by implantation of purified, culture-expanded human mesenchymal stem cells. J. Orthop. Res. 16, 155–162 (1998).
Satoh, H. et al. Transplanted mesenchymal stem cells are effective for skin regeneration in acute cutaneous wounds. Cell Transplant. 13, 405–412 (2004).
Dezawa, M., Takahashi, I., Esaki, M., Takano, M. & Sawada, H. Sciatic nerve regeneration in rats induced by transplantation of in vitro differentiated bone-marrow stromal cells. Eur. J. Neurosci. 14, 1771–1776 (2001).
von Bahr, L. et al. Analysis of tissues following mesenchymal stromal cell therapy in humans indicates limited long-term engraftment and no ectopic tissue formation. Stem Cells 30, 1575–1578 (2012).
Tran, C. & Damaser, M. S. Stem cells as drug delivery methods: application of stem cell secretome for regeneration. Adv. Drug Deliv. Rev. 82-83, 1–11 (2015).
Chen, L., Tredget, E. E., Wu, P. Y. & Wu, Y. Paracrine factors of mesenchymal stem cells recruit macrophages and endothelial lineage cells and enhance wound healing. PLoS ONE 3, e1886 (2008).
Xu, G. et al. Immunosuppressive properties of cloned bone marrow mesenchymal stem cells. Cell Res. 17, 240–248 (2007).
Petrou, P. et al. Beneficial effects of autologous mesenchymal stem cell transplantation in active progressive multiple sclerosis. Brain 143, 3574–3588 (2020).
Andreas, K., Sittinger, M. & Ringe, J. Toward in situ tissue engineering: chemokine-guided stem cell recruitment. Trends Biotechnol. 32, 483–492 (2014).
Karhausen, J., Haase, V. H. & Colgan, S. P. Inflammatory hypoxia: role of hypoxia-inducible factor. Cell Cycle 4, 256–258 (2005).
Liang, X., Arullampalam, P., Yang, Z. & Ming, X. F. Hypoxia enhances endothelial intercellular adhesion molecule 1 protein level through upregulation of arginase type II and mitochondrial oxidative stress. Front. Physiol. 10, 1003 (2019).
Li, X. et al. Intercellular adhesion molecule-1 enhances the therapeutic effects of MSCs in a dextran sulfate sodium-induced colitis models by promoting MSCs homing to murine colons and spleens. Stem Cell Res. Ther. 10, 267 (2019).
Paquet, J. et al. Oxygen tension regulates human mesenchymal stem cell paracrine functions. Stem Cells Transl. Med. 4, 809–821 (2015).
Ren, G. et al. Inflammatory cytokine-induced intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 in mesenchymal stem cells are critical for immunosuppression. J. Immunol. 184, 2321–2328 (2010).
Cassano, J. M., Schnabel, L. V., Goodale, M. B. & Fortier, L. A. Inflammatory licensed equine MSCs are chondroprotective and exhibit enhanced immunomodulation in an inflammatory environment. Stem Cell Res. Ther. 9, 82 (2018).
Ren, G. et al. Mesenchymal stem cell-mediated immunosuppression occurs via concerted action of chemokines and nitric oxide. Cell Stem Cell 2, 141–150 (2008).
Shi, Y. et al. How mesenchymal stem cells interact with tissue immuneresponses. Trends Immunol. 33, 136–143 (2012).
Szabó, E. et al. Licensing by inflammatory cytokines abolishes heterogeneity of immunosuppressive function of mesenchymal stem cell population. Stem Cells Dev. 24, 2171–2180 (2015).
Redondo-Castro, E. et al. Interleukin-1 primes human mesenchymal stem cells towards an anti-inflammatory and pro-trophic phenotype in vitro. Stem Cell Res. Ther. 8, 79 (2017).
Renner, P. et al. Mesenchymal stem cells require a sufficient, ongoing immune response to exert their immunosuppressive function. Transplant. Proc. 41, 2607–2611 (2009).
Chan, J. L. et al. Antigen-presenting property of mesenchymal stem cells occurs during a narrow window at low levels of interferon-gamma. Blood 107, 4817–4824 (2006).
François, M. et al. Mesenchymal stromal cells cross-present soluble exogenous antigens as part of their antigen-presenting cell properties. Blood 114, 2632–2638 (2009).
Vigo, T. et al. IFN-γ orchestrates mesenchymal stem cell plasticity through the signal transducer and activator of transcription 1 and 3 and mammalian target of rapamycin pathways. J. Allergy Clin. Immunol. 139, 1667–1676 (2017).
Shi Y, Su J, Roberts AI, Shou P, Rabson AB, Ren G. How mesenchymal stem cells interactwith tissue immune responses. Trends Immunol. 33, 136–43 (2012).
Ren, G. et al. CCR2-dependent recruitment of macrophages by tumor-educated mesenchymal stromal cells promotes tumor development and is mimicked by TNFα. Cell Stem Cell 11, 812–824 (2012).
Le Naour, A. et al. Tumor cells educate mesenchymal stromal cells to release chemoprotective and immunomodulatory factors. J. Mol. Cell Biol. 12, 202–215 (2020).
De Veirman, K. et al. Induction of miR-146a by multiple myeloma cells in mesenchymal stromal cells stimulates their pro-tumoral activity. Cancer Lett. 377, 17–24 (2016).
Abdul-Aziz, A. M. et al. MIF-induced stromal PKCβ/IL8 is essential in human acute myeloid leukemia. Cancer Res. 77, 303–311 (2017).
Ma, Z. et al. Bone marrow mesenchymal stromal cell-derived periostin promotes B-ALL progression by modulating CCL2 in leukemia cells. Cell Rep. 26, 1533–1543.e4 (2019).
Amé-Thomas, P. et al. Human mesenchymal stem cells isolated from bone marrow and lymphoid organs support tumor B-cell growth: role of stromal cells in follicular lymphoma pathogenesis. Blood 109, 693–702 (2007).
Ramasamy, R. et al. Mesenchymal stem cells inhibit proliferation and apoptosis of tumor cells: impact on in vivo tumor growth. Leukemia 21, 304–310 (2007).
Zhu, W. et al. Mesenchymal stem cells derived from bone marrow favor tumor cell growth in vivo. Exp. Mol. Pathol. 80, 267–274 (2006).
Waghray, M. et al. GM-CSF mediates mesenchymal-epithelial cross-talk in pancreatic cancer. Cancer Discov. 6, 886–899 (2016).
Burt, R. et al. Activated stromal cells transfer mitochondria to rescue acute lymphoblastic leukemia cells from oxidative stress. Blood 134, 1415–1429 (2019).
Guarnerio, J. et al. A non-cell-autonomous role for Pml in the maintenance of leukemia from the niche. Nat. Commun. 9, 66 (2018).
Agarwal, P. et al. Mesenchymal niche-specific expression of Cxcl12 controls quiescence of treatment-resistant leukemia stem cells. Cell Stem Cell 24, 769–784.e6 (2019).
Kota, D. J. et al. Differential MSC activation leads to distinct mononuclear leukocyte binding mechanisms. Sci. Rep. 4, 4565 (2014).
Shalaby, S. M., Sabbah, N. A., Saber, T. & Abdel Hamid, R. A. Adipose-derived mesenchymal stem cells modulate the immune response in chronic experimental autoimmune encephalomyelitis model. IUBMB Life 68, 106–115 (2016).
Chen, X. et al. The interaction between mesenchymal stem cells and steroids during inflammation. Cell Death Dis. 5, e1009 (2014).
Melief, S. M., Zwaginga, J. J., Fibbe, W. E. & Roelofs, H. Adipose tissue-derived multipotent stromal cells have a higher immunomodulatory capacity than their bone marrow-derived counterparts. Stem Cells Transl. Med. 2, 455–463 (2013).
Kizilay Mancini, O. et al. Mitochondrial oxidative stress reduces the immunopotency of mesenchymal stromal cells in adults with coronary artery disease. Circ. Res. 122, 255–266 (2018).
Chanda, D. et al. Mesenchymal stromal cell aging impairs the self-organizing capacity of lung alveolar epithelial stem cells. eLife 10, e68049 (2021).
Bustos, M. L. et al. Aging mesenchymal stem cells fail to protect because of impaired migration and antiinflammatory response. Am. J. Respir. Crit. Care Med. 189, 787–798 (2014).
Chinnadurai, R. et al. Immune dysfunctionality of replicative senescent mesenchymal stromal cells is corrected by IFNγ priming. Blood Adv. 1, 628–643 (2017).
Sudres, M. et al. Bone marrow mesenchymal stem cells suppress lymphocyte proliferation in vitro but fail to prevent graft-versus-host disease in mice. J. Immunol. 176, 7761–7767 (2006).
Wong, L. H., Eden, E. R. & Futter, C. E. Roles for ER:endosome membrane contact sites in ligand-stimulated intraluminal vesicle formation. Biochem. Soc. Trans. 46, 1055–1062 (2018).
Rani, S., Ryan, A. E., Griffin, M. D. & Ritter, T. Mesenchymal stem cell-derived extracellular vesicles: toward cell-free therapeutic applications. Mol. Ther. 23, 812–823 (2015).
Kou, X. et al. The Fas/Fap-1/Cav-1 complex regulates IL-1RA secretion in mesenchymal stem cells to accelerate wound healing. Sci. Transl. Med. 10, eaai8524 (2018).
Yu, B., Zhang, X. & Li, X. Exosomes derived from mesenchymal stem cells. Int. J. Mol. Sci. 15, 4142–4157 (2014).
Xiao, C. et al. Transplanted mesenchymal stem cells reduce autophagic flux in infarcted hearts via the exosomal transfer of miR-125b. Circ. Res. 123, 564–578 (2018).
Zhu, L. P. et al. Hypoxia-elicited mesenchymal stem cell-derived exosomes facilitates cardiac repair through miR-125b-mediated prevention of cell death in myocardial infarction. Theranostics 8, 6163–6177 (2018).
Cao, J. Y. et al. Exosomal miR-125b-5p deriving from mesenchymal stem cells promotes tubular repair by suppression of p53 in ischemic acute kidney injury. Theranostics 11, 5248–5266 (2021).
Blazquez, R. et al. Immunomodulatory potential of human adipose mesenchymal stem cells derived exosomes on in vitro stimulated T cells. Front. Immunol. 5, 556 (2014).
Kou X, Xu X, Chen C, Sanmillan ML, Cai T, ZhouY, Giraudo C, Le A, Shi S. The Fas/Fap-1/Cav-1 complex regulates IL-1RA secretion in mesenchymal stem cells toaccelerate wound healing. Sci Transl Med. 10, eaai8524 (2018).
Morrison, T. J. et al. Mesenchymal stromal cells modulate macrophages in clinically relevant lung injury models by extracellular vesicle mitochondrial transfer. Am. J. Respir. Crit. Care Med. 196, 1275–1286 (2017).
Zhao, H. et al. Exosomes from adipose-derived stem cells attenuate adipose inflammation and obesity through polarizing M2 macrophages and beiging in white adipose tissue. Diabetes 67, 235–247 (2018).
Zhao, J. et al. Mesenchymal stromal cell-derived exosomes attenuate myocardial ischaemia-reperfusion injury through miR-182-regulated macrophage polarization. Cardiovasc. Res. 115, 1205–1216 (2019).
Monsel, A. et al. Therapeutic effects of human mesenchymal stem cell-derived microvesicles in severe pneumonia in mice. Am. J. Respir. Crit. Care Med. 192, 324–336 (2015).
Mathew, B. et al. Mesenchymal stem cell-derived extracellular vesicles and retinal ischemia-reperfusion. Biomaterials 197, 146–160 (2019).
Deng, C. L. et al. Photoreceptor protection by mesenchymal stem cell transplantation identifies exosomal MiR-21 as a therapeutic for retinal degeneration. Cell Death Differ. 28, 1041–1061 (2021).
Kordelas, L. et al. MSC-derived exosomes: a novel tool to treat therapy-refractory graft-versus-host disease. Leukemia 28, 970–973 (2014).
Liu, W. et al. Melatonin-stimulated MSC-derived exosomes improve diabetic wound healing through regulating macrophage M1 and M2 polarization by targeting the PTEN/AKT pathway. Stem Cell. Res. Ther. 11, 259 (2020).
Zou, X. et al. Microvesicles derived from human Wharton’s Jelly mesenchymal stromal cells ameliorate renal ischemia-reperfusion injury in rats by suppressing CX3CL1. Stem Cell Res. Ther. 5, 40 (2014).
Riazifar, M. et al. Stem cell-derived exosomes as nanotherapeutics for autoimmune and neurodegenerative disorders. ACS Nano 13, 6670–6688 (2019).
Zhou, W. et al. Pancreatic cancer-targeting exosomes for enhancing immunotherapy and reprogramming tumor microenvironment. Biomaterials 268, 120546 (2021).
Monguió-Tortajada, M. et al. Nanosized UCMSC-derived extracellular vesicles but not conditioned medium exclusively inhibit the inflammatory response of stimulated T cells: implications for nanomedicine. Theranostics 7, 270–284 (2017).
Saeedi, P., Halabian, R. & Imani Fooladi, A. A. A revealing review of mesenchymal stem cells therapy, clinical perspectives and modification strategies. Stem Cell Investig. 6, 34 (2019).
Askenase, P. W. COVID-19 therapy with mesenchymal stromal cells (MSC) and convalescent plasma must consider exosome involvement: Do the exosomes in convalescent plasma antagonize the weak immune antibodies? J. Extracell. Vesicles 10, e12004 (2020).
Rahman, M. J., Regn, D., Bashratyan, R. & Dai, Y. D. Exosomes released by islet-derived mesenchymal stem cells trigger autoimmune responses in NOD mice. Diabetes 63, 1008–1020 (2014).
Kim, J. Y. et al. Defined MSC exosome with high yield and purity to improve regenerative activity. J. Tissue Eng. 12, 20417314211008626 (2021).
Liu, W. et al. Hypoxic mesenchymal stem cell-derived exosomes promote bone fracture healing by the transfer of miR-126. Acta Biomater. 103, 196–212 (2020).
Chen, P. et al. Desktop-stereolithography 3D printing of a radially oriented extracellular matrix/mesenchymal stem cell exosome bioink for osteochondral defect regeneration. Theranostics 9, 2439–2459 (2019).
Chamberlain, G., Smith, H., Rainger, G. E. & Middleton, J. Mesenchymal stem cells exhibit firm adhesion, crawling, spreading and transmigration across aortic endothelial cells: effects of chemokines and shear. PLoS ONE 6, e25663 (2011).
Wynn, R. F. et al. A small proportion of mesenchymal stem cells strongly expresses functionally active CXCR4 receptor capable of promoting migration to bone marrow. Blood 104, 2643–2645 (2004).
Hatzistergos, K. E. et al. Stimulatory effects of mesenchymal stem cells on cKit+ cardiac stem cells are mediated by SDF1/CXCR4 and SCF/cKit signaling pathways. Circ. Res. 119, 921–930 (2016).
Liu, L. et al. Hypoxia-inducible factor-1α is essential for hypoxia-induced mesenchymal stem cell mobilization into the peripheral blood. Stem Cells Dev. 20, 1961–1971 (2011).
Jalili, A. et al. Complement C1q enhances homing-related responses of hematopoietic stem/progenitor cells. Transfusion 50, 2002–2010 (2010).
Ratajczak, M. Z., Suszynska, M., Borkowska, S., Ratajczak, J. & Schneider, G. The role of sphingosine-1 phosphate and ceramide-1 phosphate in trafficking of normal stem cells and cancer cells. Expert Opin. Ther. Targets 18, 95–107 (2014).
Ponte, A. L. et al. The in vitro migration capacity of human bone marrow mesenchymal stem cells: comparison of chemokine and growth factor chemotactic activities. Stem Cells 25, 1737–1745 (2007).
Shi, C. et al. Bone marrow mesenchymal stem and progenitor cells induce monocyte emigration in response to circulating toll-like receptor ligands. Immunity 34, 590–601 (2011).
Akiyama, K. et al. Mesenchymal-stem-cell-induced immunoregulation involves FAS-ligand-/FAS-mediated T cell apoptosis. Cell Stem Cell 10, 544–555 (2012).
Abdul-Muneer, P. M. et al. Traumatic brain injury induced matrix metalloproteinase2 cleaves CXCL12α (stromal cell derived factor 1α) and causes neurodegeneration. Brain Behav. Immun. 59, 190–199 (2017).
Rafei, M. et al. Mesenchymal stromal cells ameliorate experimental autoimmune encephalomyelitis by inhibiting CD4 Th17 T cells in a CC chemokine ligand 2-dependent manner. J. Immunol. 182, 5994–6002 (2009).
Zheng, Z., Jia, S., Shao, C. & Shi, Y. Irradiation induces cancer lung metastasis through activation of the cGAS-STING-CCL5 pathway in mesenchymal stromal cells. Cell Death Dis. 11, 326 (2020).
Galipeau, J. Macrophages at the nexus of mesenchymal stromal cell potency: the emerging role of chemokine cooperativity. Stem Cells 39, 1145–1154 (2021).
Kraemer, S., Alampour-Rajabi, S., El Bounkari, O. & Bernhagen, J. Hetero-oligomerization of chemokine receptors: diversity and relevance for function. Curr. Med. Chem. 20, 2524–2536 (2013).
Huang, L. et al. Mesenchymal stem cells modulate light-induced activation of retinal microglia through CX3CL1/CX3CR1 signaling. Ocul. Immunol. Inflamm. 24, 684–692 (2016).
Murakami, J. et al. Vascular endothelial growth factor-C induces osteogenic differentiation of human mesenchymal stem cells through the ERK and RUNX2 pathway. Biochem. Biophys. Res. Commun. 484, 710–718 (2017).
Suga, H. et al. IFATS collection: fibroblast growth factor-2-induced hepatocyte growth factor secretion by adipose-derived stromal cells inhibits postinjury fibrogenesis through a c-Jun N-terminal kinase-dependent mechanism. Stem Cells 27, 238–249 (2009).
Kinnaird, T. et al. Local delivery of marrow-derived stromal cells augments collateral perfusion through paracrine mechanisms. Circulation 109, 1543–1549 (2004).
Tögel, F. et al. Vasculotropic, paracrine actions of infused mesenchymal stem cells are important to the recovery from acute kidney injury. Am. J. Physiol. Ren. Physiol. 292, F1626–F1635 (2007).
Zhu, M. et al. Mesenchymal stromal cells pretreated with pro-inflammatory cytokines promote skin wound healing through VEGFC-mediated angiogenesis. Stem Cells Transl. Med. 9, 1218–1232 (2020).
Shang, Q. et al. Adipose-derived mesenchymal stromal cells promote corneal wound healing by accelerating the clearance of neutrophils in cornea. Cell Death Dis. 11, 707 (2020).
Medi, E. et al. Corneal mesenchymal stromal cells are directly antiangiogenic via PEDF and sFLT-1. Invest. Ophthalmol. Vis. Sci. 58, 5507–5517 (2017).
Wang, H. et al. Mesenchymal stem cells microvesicles stabilize endothelial barrier function partly mediated by hepatocyte growth factor (HGF). Stem Cell Res. Ther. 8, 211 (2017).
An, S. Y. et al. Milk fat globule-EGF factor 8, secreted by mesenchymal stem cells, protects against liver fibrosis in mice. Gastroenterology 152, 1174–1186 (2017).
Cahill, E. F., Kennelly, H., Carty, F., Mahon, B. P. & English, K. Hepatocyte growth factor is required for mesenchymal stromal cell protection against bleomycin-induced pulmonary fibrosis. Stem Cells Transl. Med. 5, 1307–1318 (2016).
Bai, L. et al. Hepatocyte growth factor mediates mesenchymal stem cell–induced recovery in multiple sclerosis models. Nat. Neurosci. 15, 862–870 (2012).
Jia, Y. et al. HGF mediates clinical-grade human umbilical cord-derived mesenchymal stem cells improved functional recovery in a senescence-accelerated mouse model of Alzheimer’s disease. Adv. Sci. 7, 1903809 (2020).
Yuan, X. et al. Mesenchymal stem cell therapy induces FLT3L and CD1c(+) dendritic cells in systemic lupus erythematosus patients. Nat. Commun. 10, 2498 (2019).
Fang, J. et al. Skeletal muscle stem cells confer maturing macrophages anti-inflammatory properties through insulin-like growth factor-2. Stem Cells Transl. Med. 9, 773–785 (2020).
Du, L. et al. IGF-2 preprograms maturing macrophages to acquire oxidative phosphorylation-dependent anti-inflammatory properties. Cell Metab. 29, 1363–1375.e8 (2019).
Rychli, K., Huber, K. & Wojta, J. Pigment epithelium-derived factor (PEDF) as a therapeutic target in cardiovascular disease. Expert Opin. Ther. Targets 13, 1295–1302 (2009).
Liang, H. et al. Increased expression of pigment epithelium-derived factor in aged mesenchymal stem cells impairs their therapeutic efficacy for attenuating myocardial infarction injury. Eur. Heart J. 34, 1681–1690 (2013).
Haynesworth, S. E., Baber, M. A. & Caplan, A. I. Cytokine expression by human marrow-derived mesenchymal progenitor cells in vitro: effects of dexamethasone and IL-1 alpha. J. Cell. Physiol. 166, 585–592 (1996).
Majumdar, M. K., Thiede, M. A., Mosca, J. D., Moorman, M. & Gerson, S. L. Phenotypic and functional comparison of cultures of marrow-derived mesenchymal stem cells (MSCs) and stromal cells. J. Cell. Physiol. 176, 57–66 (1998).
Nguyen, D. C. et al. Factors of the bone marrow microniche that support human plasma cell survival and immunoglobulin secretion. Nat. Commun. 9, 3698 (2018).
Xu, G., Zhang, Y., Zhang, L., Ren, G. & Shi, Y. The role of IL-6 in inhibition of lymphocyte apoptosis by mesenchymal stem cells. Biochem. Biophys. Res. Commun. 361, 745–750 (2007).
Nemoto, Y. et al. Bone marrow-mesenchymal stem cells are a major source of interleukin-7 and sustain colitis by forming the niche for colitogenic CD4 memory T cells. Gut 62, 1142–1152 (2013).
Brandau, S. et al. Tissue-resident mesenchymal stem cells attract peripheral blood neutrophils and enhance their inflammatory activity in response to microbial challenge. J. Leukoc. Biol. 88, 1005–1015 (2010).
Le Blanc, K. & Mougiakakos, D. Multipotent mesenchymal stromal cells and the innate immune system. Nat. Rev. Immunol. 12, 383–396 (2012).
Xie, X. et al. Rat BMSC infusion was unable to ameliorate inflammatory injuries in tissues of mice with LPS-induced endotoxemia. Biomed. Mater. Eng. 28, S129–s138 (2017).
McGuire, J. J. et al. Mesenchymal stem cell-derived interleukin-28 drives the selection of apoptosis resistant bone metastatic prostate cancer. Nat. Commun. 12, 723 (2021).
Zheng, Z. et al. Lung mesenchymal stromal cells influenced by Th2 cytokines mobilize neutrophils and facilitate metastasis by producing complement C3. Nat. Commun. 12, 6202 (2021).
Djouad, F. et al. Mesenchymal stem cells inhibit the differentiation of dendritic cells through an interleukin-6-dependent mechanism. Stem Cells 25, 2025–2032 (2007).
Nasef, A. et al. Immunosuppressive effects of mesenchymal stem cells: involvement of HLA-G. Transplantation 84, 231–237 (2007).
Nasef, A. et al. Leukemia inhibitory factor: role in human mesenchymal stem cells mediated immunosuppression. Cell Immunol. 253, 16–22 (2008).
Yang, S. H. et al. Soluble mediators from mesenchymal stem cells suppress T cell proliferation by inducing IL-10. Exp. Mol. Med. 41, 315–324 (2009).
Selmani, Z. et al. Human leukocyte antigen-G5 secretion by human mesenchymal stem cells is required to suppress T lymphocyte and natural killer function and to induce CD4+CD25highFOXP3+ regulatory T cells. Stem Cells 26, 212–222 (2008).
Ortiz, L. A. et al. Interleukin 1 receptor antagonist mediates the antiinflammatory and antifibrotic effect of mesenchymal stem cells during lung injury. Proc. Natl Acad. Sci. USA. 104, 11002–11007 (2007).
Zhang, Q. Z. et al. Human gingiva-derived mesenchymal stem cells elicit polarization of m2 macrophages and enhance cutaneous wound healing. Stem Cells 28, 1856–1868 (2010).
Luz-Crawford, P. et al. Mesenchymal Stem Cell-Derived Interleukin 1 Receptor Antagonist Promotes Macrophage Polarization and Inhibits B Cell Differentiation. Stem Cells 34, 483–492 (2016).
Park, H. J., Oh, S. H., Kim, H. N., Jung, Y. J. & Lee, P. H. Mesenchymal stem cells enhance α-synuclein clearance via M2 microglia polarization in experimental and human parkinsonian disorder. Acta Neuropathol. 132, 685–701 (2016).
Nemeth, K. et al. Bone marrow stromal cells use TGF-beta to suppress allergic responses in a mouse model of ragweed-induced asthma. Proc. Natl Acad. Sci. U. S. A. 107, 5652–5657 (2010).
English, K. et al. Cell contact, prostaglandin E(2) and transforming growth factor beta 1 play non-redundant roles in human mesenchymal stem cell induction of CD4+CD25(High) forkhead box P3+ regulatory T cells. Clin. Exp. Immunol. 156, 149–160 (2009).
Noh, M. Y. et al. Mesenchymal Stem Cells Modulate the Functional Properties of Microglia via TGF-β Secretion. Stem Cells Transl. Med. 5, 1538–1549 (2016).
Xu, C. et al. TGF-β promotes immune responses in the presence of mesenchymal stem cells. J. Immunol. 192, 103–109 (2014).
Sharma, P., Bolten, Z. T., Wagner, D. R. & Hsieh, A. H. Deformability of Human Mesenchymal Stem Cells Is Dependent on Vimentin Intermediate Filaments. Ann. Biomed. Eng. 45, 1365–1374 (2017).
Sioud, M., Mobergslien, A., Boudabous, A. & Fløisand, Y. Mesenchymal stem cell-mediated T cell suppression occurs through secreted galectins. Int. J. Oncol. 38, 385–390 (2011).
Kumar, S. & Ponnazhagan, S. Bone homing of mesenchymal stem cells by ectopic alpha 4 integrin expression. FASEB J. 21, 3917–3927 (2007).
Sorrell, J. M., Baber, M. A. & Caplan, A. I. Influence of adult mesenchymal stem cells on in vitro vascular formation. Tissue Eng. Part A 15, 1751–1761 (2009).
Mauney, J. & Volloch, V. Adult human bone marrow stromal cells regulate expression of their MMPs and TIMPs in differentiation type-specific manner. Matrix Biol. 29, 3–8 (2010).
Mauney, J. & Volloch, V. Human bone marrow-derived stromal cells show highly efficient stress-resistant adipogenesis on denatured collagen IV matrix but not on its native counterpart: implications for obesity. Matrix Biol. 29, 9–14 (2010).
Chaly, Y. et al. Follistatin-like protein 1 regulates chondrocyte proliferation and chondrogenic differentiation of mesenchymal stem cells. Ann. Rheum. Dis. 74, 1467–1473 (2015).
Sorokin, L. The impact of the extracellular matrix on inflammation. Nat. Rev. Immunol. 10, 712–723 (2010).
Coulson-Thomas, V. J., Gesteira, T. F., Hascall, V. & Kao, W. Umbilical cord mesenchymal stem cells suppress host rejection: the role of the glycocalyx. J. Biol. Chem. 289, 23465–23481 (2014).
Salanga, C. L. & Handel, T. M. Chemokine oligomerization and interactions with receptors and glycosaminoglycans: the role of structural dynamics in function. Exp. Cell Res. 317, 590–601 (2011).
Bollyky, P. L. et al. Cutting edge: high molecular weight hyaluronan promotes the suppressive effects of CD4+CD25+ regulatory T cells. J. Immunol. 179, 744–747 (2007).
Bollyky, P. L. et al. ECM components guide IL-10 producing regulatory T-cell (TR1) induction from effector memory T-cell precursors. Proc. Natl Acad. Sci. USA 108, 7938–7943 (2011).
Yun, S. P., Lee, S. J., Jung, Y. H. & Han, H. J. Galectin-1 stimulates motility of human umbilical cord blood-derived mesenchymal stem cells by downregulation of smad2/3-dependent collagen 3/5 and upregulation of NF-κB-dependent fibronectin/laminin 5 expression. Cell Death Dis. 5, e1049 (2014).
Herrera, M. B. et al. Exogenous mesenchymal stem cells localize to the kidney by means of CD44 following acute tubular injury. Kidney Int. 72, 430–441 (2007).
MacArthur, J. W. Jr. et al. Sustained release of engineered stromal cell-derived factor 1-α from injectable hydrogels effectively recruits endothelial progenitor cells and preserves ventricular function after myocardial infarction. Circulation 128, S79–S86 (2013).
Lim, T. C. et al. Chemotactic recruitment of adult neural progenitor cells into multifunctional hydrogels providing sustained SDF-1α release and compatible structural support. FASEB J. 27, 1023–1033 (2013).
Su, J. et al. Phylogenetic distinction of iNOS and IDO function in mesenchymal stem cell-mediated immunosuppression in mammalian species. Cell Death Differ. 21, 388–396 (2014).
Hoffman, R. A. et al. Differential modulation of CD4 and CD8 T-cell proliferation by induction of nitric oxide synthesis in antigen presenting cells. Transplantation 74, 836–845 (2002).
Sato, K. et al. Nitric oxide plays a critical role in suppression of T-cell proliferation by mesenchymal stem cells. Blood 109, 228–234 (2007).
Jiang, M. et al. Phosphatase SHP1 impedes mesenchymal stromal cell immunosuppressive capacity modulated by JAK1/STAT3 and P38 signals. Cell Biosci. 10, 65 (2020).
Han, X. et al. Interleukin-17 enhances immunosuppression by mesenchymal stem cells. Cell Death Differ. 21, 1758–1768 (2014).
Raghuvanshi, S., Sharma, P., Singh, S., Van Kaer, L. & Das, G. Mycobacterium tuberculosis evades host immunity by recruiting mesenchymal stem cells. Proc. Natl Acad. Sci. USA 107, 21653–21658 (2010).
Van Linthout, S. et al. Mesenchymal stem cells improve murine acute coxsackievirus B3-induced myocarditis. Eur. Heart J. 32, 2168–2178 (2011).
Li, W. et al. Mesenchymal stem cells: a double-edged sword in regulating immune responses. Cell Death Differ. 19, 1505–1513 (2012).
Maria, A. T. J. et al. iNOS activity is required for the therapeutic effect of mesenchymal stem cells in experimental systemic sclerosis. Front. Immunol. 9, 3056 (2018).
Nasef, A. et al. Identification of IL-10 and TGF-beta transcripts involved in the inhibition of T-lymphocyte proliferation during cell contact with human mesenchymal stem cells. Gene Expr. 13, 217–226 (2007).
Munn, D. H. & Mellor, A. L. IDO in the tumor microenvironment: inflammation, counter-regulation, and tolerance. Trends Immunol. 37, 193–207 (2016).
Mellor, A. L. & Munn, D. H. Tryptophan catabolism and T-cell tolerance: immunosuppression by starvation? Immunol. Today 20, 469–473 (1999).
Munn, D. H. et al. GCN2 kinase in T cells mediates proliferative arrest and anergy induction in response to indoleamine 2,3-dioxygenase. Immunity 22, 633–642 (2005).
Frumento, G. et al. Tryptophan-derived catabolites are responsible for inhibition of T and natural killer cell proliferation induced by indoleamine 2,3-dioxygenase. J. Exp. Med. 196, 459–468 (2002).
Meisel, R. et al. Human bone marrow stromal cells inhibit allogeneic T-cell responses by indoleamine 2,3-dioxygenase-mediated tryptophan degradation. Blood 103, 4619–4621 (2004).
Mezrich, J. D. et al. An interaction between kynurenine and the aryl hydrocarbon receptor can generate regulatory T cells. J. Immunol. 185, 3190–3198 (2010).
Wang, G. et al. Kynurenic acid, an IDO metabolite, controls TSG-6-mediated immunosuppression of human mesenchymal stem cells. Cell Death Differ. 25, 1209–1223 (2018).
François, M., Romieu-Mourez, R., Li, M. & Galipeau, J. Human MSC suppression correlates with cytokine induction of indoleamine 2,3-dioxygenase and bystander M2 macrophage differentiation. Mol. Ther. 20, 187–195 (2012).
Metghalchi, S. et al. Indoleamine 2,3-dioxygenase fine-tunes immune homeostasis in atherosclerosis and colitis through repression of interleukin-10 production. Cell Metab. 22, 460–471 (2015).
Mounayar, M. et al. PI3kα and STAT1 interplay regulates human mesenchymal stem cell immune polarization. Stem Cells 33, 1892–1901 (2015).
Jitschin, R. et al. Inflammation-induced glycolytic switch controls suppressivity of mesenchymal stem cells via STAT1 glycosylation. Leukemia 33, 1783–1796 (2019).
Okamoto, A. et al. Indoleamine 2,3-dioxygenase serves as a marker of poor prognosis in gene expression profiles of serous ovarian cancer cells. Clin. Cancer Res. 11, 6030–6039 (2005).
Zhou, L. et al. Melatonin reverses H2 O2 -induced premature senescence in mesenchymal stem cells via the SIRT1-dependent pathway. J. Pineal Res. 59, 190–205 (2015).
Luchetti, F. et al. Melatonin regulates mesenchymal stem cell differentiation: a review. J. Pineal Res. 56, 382–397 (2014).
Patel, D. et al. Kynurenine induces an age-related phenotype in bone marrow stromal cells. Mech. Ageing Dev. 195, 111464 (2021).
Kondrikov, D. et al. Kynurenine inhibits autophagy and promotes senescence in aged bone marrow mesenchymal stem cells through the aryl hydrocarbon receptor pathway. Exp. Gerontol. 130, 110805 (2020).
Najar, M. et al. Mesenchymal stromal cells use PGE2 to modulate activation and proliferation of lymphocyte subsets: combined comparison of adipose tissue, Wharton’s Jelly and bone marrow sources. Cell. Immunol. 264, 171–179 (2010).
Matysiak, M., Orlowski, W., Fortak-Michalska, M., Jurewicz, A. & Selmaj, K. Immunoregulatory function of bone marrow mesenchymal stem cells in EAE depends on their differentiation state and secretion of PGE2. J. Neuroimmunol. 233, 106–111 (2011).
Alexanian, A. & Sorokin, A. Cyclooxygenase 2: protein-protein interactions and posttranslational modifications. Physiol. Genomics 49, 667–681 (2017).
Vasandan, A. B. et al. Human mesenchymal stem cells program macrophage plasticity by altering their metabolic status via a PGE2-dependent mechanism. Sci. Rep. 6, 38308 (2016).
Galland, S. et al. Tumor-derived mesenchymal stem cells use distinct mechanisms to block the activity of natural killer cell subsets. Cell Rep. 20, 2891–2905 (2017).
Tatara, R. et al. Mesenchymal stromal cells inhibit Th17 but not regulatory T-cell differentiation. Cytotherapy 13, 686–694 (2011).
Brown, J. M., Nemeth, K., Kushnir-Sukhov, N. M., Metcalfe, D. D. & Mezey, E. Bone marrow stromal cells inhibit mast cell function via a COX2-dependent mechanism. Clin. Exp. Allergy 41, 526–534 (2011).
Sareen, N. et al. Hypoxia-induced downregulation of cyclooxygenase 2 leads to the loss of immunoprivilege of allogeneic mesenchymal stem cells. FASEB J. 34, 15236–15251 (2020).
Zhang, Y. et al. Mesenchymal stem cells alleviate bacteria-induced liver injury in mice by inducing regulatory dendritic cells. Hepatology 59, 671–682 (2014).
Wasnik, S. et al. Cyclooxygenase 2 augments osteoblastic but suppresses chondrocytic differentiation of CD90(+) skeletal stem cells in fracture sites. Sci. Adv. 5, eaaw2108 (2019).
Lu, L. Y. et al. Pro-inflammatory M1 macrophages promote osteogenesis by mesenchymal stem cells via the COX-2-prostaglandin E2 pathway. J. Orthop. Res. 35, 2378–2385 (2017).
McClain-Caldwell, I. et al. Immunogenic potential of human bone marrow mesenchymal stromal cells is enhanced by hyperthermia. Cytotherapy 20, 1437–1444 (2018).
Li, H. J., Reinhardt, F., Herschman, H. R. & Weinberg, R. A. Cancer-stimulated mesenchymal stem cells create a carcinoma stem cell niche via prostaglandin E2 signaling. Cancer Discov. 2, 840–855 (2012).
Hegyi, B., Kudlik, G., Monostori, E. & Uher, F. Activated T-cells and pro-inflammatory cytokines differentially regulate prostaglandin E2 secretion by mesenchymal stem cells. Biochem. Biophys. Res. Commun. 419, 215–220 (2012).
Poligone, B. & Baldwin, A. S. Positive and negative regulation of NF-kappaB by COX-2: roles of different prostaglandins. J. Biol. Chem. 276, 38658–38664 (2001).
Lee, S. et al. DNA methyltransferase inhibition accelerates the immunomodulation and migration of human mesenchymal stem cells. Sci. Rep. 5, 8020 (2015).
Zhang, Z. et al. Clearance of apoptotic cells by mesenchymal stem cells contributes to immunosuppression via PGE2. EBioMedicine 45, 341–350 (2019).
Clark, K. C. et al. Canine and equine mesenchymal stem cells grown in serum free media have altered immunophenotype. Stem Cell Rev. Rep. 12, 245–256 (2016).
Bassal, N. K., Hughes, B. P. & Costabile, M. Arachidonic acid and its COX1/2 metabolites inhibit interferon-γ mediated induction of indoleamine-2,3 dioxygenase in THP-1 cells and human monocytes. Prostaglandins Leukot. Essent. Fat. Acids 87, 119–126 (2012).
Lee, R. H. et al. Intravenous hMSCs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein TSG-6. Cell Stem Cell 5, 54–63 (2009).
Choi, H., Lee, R. H., Bazhanov, N., Oh, J. Y. & Prockop, D. J. Anti-inflammatory protein TSG-6 secreted by activated MSCs attenuates zymosan-induced mouse peritonitis by decreasing TLR2/NF-κB signaling in resident macrophages. Blood 118, 330–338 (2011).
Danchuk, S. et al. Human multipotent stromal cells attenuate lipopolysaccharide-induced acute lung injury in mice via secretion of tumor necrosis factor-α-induced protein 6. Stem Cell Res. Ther. 2, 27 (2011).
Oh, J. Y. et al. Anti-inflammatory protein TSG-6 reduces inflammatory damage to the cornea following chemical and mechanical injury. Proc. Natl Acad. Sci. USA 107, 16875–16880 (2010).
Wan, Y. M. et al. Mesenchymal stem cells alleviate liver injury induced by chronic-binge ethanol feeding in mice via release of TSG6 and suppression of STAT3 activation. Stem Cell Res. Ther. 11, 24 (2020).
Huang, P. et al. HSD11B1 is upregulated synergistically by IFNγ and TNFα and mediates TSG-6 expression in human UC-MSCs. Cell Death Discov. 6, 24 (2020).
Lee, T. H., Wisniewski, H. G. & Vilcek, J. A novel secretory tumor necrosis factor-inducible protein (TSG-6) is a member of the family of hyaluronate binding proteins, closely related to the adhesion receptor CD44. J. Cell Biol. 116, 545–557 (1992).
Kohda, D. et al. Solution structure of the link module: a hyaluronan-binding domain involved in extracellular matrix stability and cell migration. Cell 86, 767–775 (1996).
Parkar, A. A. & Day, A. J. Overlapping sites on the Link module of human TSG-6 mediate binding to hyaluronan and chrondroitin-4-sulphate. FEBS Lett. 410, 413–417 (1997).
Parkar, A. A., Kahmann, J. D., Howat, S. L., Bayliss, M. T. & Day, A. J. TSG-6 interacts with hyaluronan and aggrecan in a pH-dependent manner via a common functional element: implications for its regulation in inflamed cartilage. FEBS Lett. 428, 171–176 (1998).
Torihashi, S. et al. Acute and temporal expression of tumor necrosis factor (TNF)-α-stimulated gene 6 product, TSG6, in mesenchymal stem cells creates microenvironments required for their successful transplantation into muscle tissue. J. Biol. Chem. 290, 22771–22781 (2015).
Kota, D. J., Wiggins, L. L., Yoon, N. & Lee, R. H. TSG-6 produced by hMSCs delays the onset of autoimmune diabetes by suppressing Th1 development and enhancing tolerogenicity. Diabetes 62, 2048–2058 (2013).
Li, Y. et al. Cell-cell contact with proinflammatory macrophages enhances the immunotherapeutic effect of mesenchymal stem cells in two abortion models. Cell Mol. Immunol. 16, 908–920 (2019).
Cao, T. V., La, M., Getting, S. J., Day, A. J. & Perretti, M. Inhibitory effects of TSG-6 Link module on leukocyte-endothelial cell interactions in vitro and in vivo. Microcirculation 11, 615–624 (2004).
Getting, S. J. et al. The link module from human TSG-6 inhibits neutrophil migration in a hyaluronan- and inter-alpha -inhibitor-independent manner. J. Biol. Chem. 277, 51068–51076 (2002).
Dyer, D. P. et al. The anti-inflammatory protein TSG-6 regulates chemokine function by inhibiting chemokine/glycosaminoglycan interactions. J. Biol. Chem. 291, 12627–12640 (2016).
Dyer, D. P. et al. TSG-6 inhibits neutrophil migration via direct interaction with the chemokine CXCL8. J. Immunol. 192, 2177–2185 (2014).
Liebig, B. E., Kisiday, J. D., Bahney, C. S., Ehrhart, N. P. & Goodrich, L. R. The platelet-rich plasma and mesenchymal stem cell milieu: a review of therapeutic effects on bone healing. J. Orthop. Res. 38, 2539–2550 (2020).
Levoux, J. et al. Platelets facilitate the wound-healing capability of mesenchymal stem cells by mitochondrial transfer and metabolic reprogramming. Cell Metab. 33, 283–299.e9 (2021).
Segers, V. F. et al. Local delivery of protease-resistant stromal cell derived factor-1 for stem cell recruitment after myocardial infarction. Circulation 116, 1683–1692 (2007).
Jay, S. M. et al. Dual delivery of VEGF and MCP-1 to support endothelial cell transplantation for therapeutic vascularization. Biomaterials 31, 3054–3062 (2010).
Meyerrose, T. E. et al. Lentiviral-transduced human mesenchymal stem cells persistently express therapeutic levels of enzyme in a xenotransplantation model of human disease. Stem Cells 26, 1713–1722 (2008).
Chen, H. et al. Prolyl hydroxylase 2 silencing enhances the paracrine effects of mesenchymal stem cells on necrotizing enterocolitis in an NF-κB-dependent mechanism. Cell Death Dis. 11, 188 (2020).
Chen, Q. et al. Therapeutic potential of bone marrow-derived mesenchymal stem cells producing pigment epithelium-derived factor in lung carcinoma. Int. J. Mol. Med. 30, 527–534 (2012).
Iida, Y. et al. Local injection of CCL19-expressing mesenchymal stem cells augments the therapeutic efficacy of anti-PD-L1 antibody by promoting infiltration of immune cells. J. Immunother. Cancer 8, e000582 (2020).
Yin, P. et al. Targeted delivery of CXCL9 and OX40L by mesenchymal stem cells elicits potent antitumor immunity. Mol. Ther. 28, 2553–2563 (2020).
Sisto, F. et al. Human mesenchymal stromal cells can uptake and release ciprofloxacin, acquiring in vitro anti-bacterial activity. Cytotherapy 16, 181–190 (2014).
Won, C. H. et al. The basic mechanism of hair growth stimulation by adipose-derived stem cells and their secretory factors. Curr. Stem Cell Res. Ther. 12, 535–543 (2017).
Seetharaman, R., Mahmood, A., Kshatriya, P., Patel, D. & Srivastava, A. Mesenchymal stem cell conditioned media ameliorate Psoriasis vulgaris: a case study. Case Rep. Dermatol. Med. 2019, 8309103 (2019).
Walter, M. N., Wright, K. T., Fuller, H. R., MacNeil, S. & Johnson, W. E. Mesenchymal stem cell-conditioned medium accelerates skin wound healing: an in vitro study of fibroblast and keratinocyte scratch assays. Exp. Cell Res. 316, 1271–1281 (2010).
Saheli, M. et al. Human mesenchymal stem cells-conditioned medium improves diabetic wound healing mainly through modulating fibroblast behaviors. Arch. Dermatol. Res. 312, 325–336 (2020).
Park, I. S., Kim, J. H., Bae, J. S., Kim, D. K. & Mo, J. H. The supernatant of tonsil-derived mesenchymal stem cell has antiallergic effects in allergic rhinitis mouse model. Mediators Inflamm. 2020, 6982438 (2020).
Navas, A. et al. Anti-inflammatory and anti-fibrotic effects of human amniotic membrane mesenchymal stem cells and their potential in corneal repair. Stem Cells Transl. Med. 7, 906–917 (2018).
Jha, K. A. et al. TSG-6 in conditioned media from adipose mesenchymal stem cells protects against visual deficits in mild traumatic brain injury model through neurovascular modulation. Stem Cell. Res. Ther. 10, 318 (2019).
Su, W. et al. Culture medium from TNF-α-stimulated mesenchymal stem cells attenuates allergic conjunctivitis through multiple antiallergic mechanisms. J. Allergy Clin. Immunol. 136, 423–432.e8 (2015).
Daltro, P. S. et al. Therapy with mesenchymal stromal cells or conditioned medium reverse cardiac alterations in a high-fat diet-induced obesity model. Cytotherapy 19, 1176–1188 (2017).
Angoulvant, D. et al. Mesenchymal stem cell conditioned media attenuates in vitro and ex vivo myocardial reperfusion injury. J. Heart Lung Transplant. 30, 95–102 (2011).
Chen, Z. Y., Hu, Y. Y., Hu, X. F. & Cheng, L. X. The conditioned medium of human mesenchymal stromal cells reduces irradiation-induced damage in cardiac fibroblast cells. J. Radiat. Res. 59, 555–564 (2018).
Pouya, S. et al. Study the effects of mesenchymal stem cell conditioned medium injection in mouse model of acute colitis. Int. Immunopharmacol. 54, 86–94 (2018).
Tan, C. Y. et al. Mesenchymal stem cell-derived exosomes promote hepatic regeneration in drug-induced liver injury models. Stem Cell Res. Ther. 5, 76 (2014).
Zheng, J. et al. MSCs ameliorate hepatocellular apoptosis mediated by PINK1-dependent mitophagy in liver ischemia/reperfusion injury through AMPKα activation. Cell Death Dis. 11, 256 (2020).
Chaubey, S. et al. Early gestational mesenchymal stem cell secretome attenuates experimental bronchopulmonary dysplasia in part via exosome-associated factor TSG-6. Stem Cell Res. Ther. 9, 173 (2018).
Krasnodembskaya, A. et al. Antibacterial effect of human mesenchymal stem cells is mediated in part from secretion of the antimicrobial peptide LL-37. Stem Cells 28, 2229–2238 (2010).
Kim, S. Y. et al. Mesenchymal stem cell-conditioned media recovers lung fibroblasts from cigarette smoke-induced damage. Am. J. Physiol. Lung Cell Mol. Physiol. 302, L891–L908 (2012).
Obendorf, J., Fabian, C., Thome, U. H. & Laube, M. Paracrine stimulation of perinatal lung functional and structural maturation by mesenchymal stem cells. Stem Cell Res. Ther. 11, 525 (2020).
Liu, B. et al. Human umbilical cord mesenchymal stem cell conditioned medium attenuates renal fibrosis by reducing inflammation and epithelial-to-mesenchymal transition via the TLR4/NF-κB signaling pathway in vivo and in vitro. Stem Cell Res. Ther. 9, 7 (2018).
Islam, M. N. et al. Human mesenchymal stromal cells broadly modulate high glucose-induced inflammatory responses of renal proximal tubular cell monolayers. Stem Cell Res. Ther. 10, 329 (2019).
Zheng, J., Wang, Q., Leng, W., Sun, X. & Peng, J. Bone marrow‑derived mesenchymal stem cell‑conditioned medium attenuates tubulointerstitial fibrosis by inhibiting monocyte mobilization in an irreversible model of unilateral ureteral obstruction. Mol. Med. Rep. 17, 7701–7707 (2018).
Shen, B. et al. CCR2 positive exosome released by mesenchymal stem cells suppresses macrophage functions and alleviates ischemia/reperfusion-induced renal injury. Stem Cells Int. 2016, 1240301 (2016).
Evangelista, A. F. et al. Bone marrow-derived mesenchymal stem/stromal cells reverse the sensorial diabetic neuropathy via modulation of spinal neuroinflammatory cascades. J. Neuroinflammation 15, 189 (2018).
De Gregorio, C. et al. Human adipose-derived mesenchymal stem cell-conditioned medium ameliorates polyneuropathy and foot ulceration in diabetic BKS db/db mice. Stem Cell Res. Ther. 11, 168 (2020).
Song, P. et al. The role of hepatocyte growth factor in mesenchymal stem cell-induced recovery in spinal cord injured rats. Stem Cell Res. Ther. 11, 178 (2020).
Katagiri, W. et al. Clinical study of bone regeneration by conditioned medium from mesenchymal stem cells after maxillary sinus floor elevation. Implant Dent. 26, 607–612 (2017).
Furuta, T. et al. Mesenchymal stem cell-derived exosomes promote fracture healing in a mouse model. Stem Cells Transl. Med. 5, 1620–1630 (2016).
Simental-Mendía, M. et al. Anti‑inflammatory and anti‑catabolic effect of non‑animal stabilized hyaluronic acid and mesenchymal stem cell‑conditioned medium in an osteoarthritis coculture model. Mol. Med. Rep. 21, 2243–2250 (2020).
Nazemian, V., Manaheji, H., Sharifi, A. M. & Zaringhalam, J. Long term treatment by mesenchymal stem cells conditioned medium modulates cellular, molecular and behavioral aspects of adjuvant-induced arthritis. Cell. Mol. Biol. 64, 19–26 (2018).
Chen, W. et al. Conditioned medium of mesenchymal stem cells delays osteoarthritis progression in a rat model by protecting subchondral bone, maintaining matrix homeostasis, and enhancing autophagy. J. Tissue Eng. Regen. Med. 13, 1618–1628 (2019).
Mitchell, R. et al. Secretome of adipose-derived mesenchymal stem cells promotes skeletal muscle regeneration through synergistic action of extracellular vesicle cargo and soluble proteins. Stem Cell Res. Ther. 10, 116 (2019).
Park, C. M. et al. Umbilical cord mesenchymal stem cell-conditioned media prevent muscle atrophy by suppressing muscle atrophy-related proteins and ROS generation. Vitr. Cell. Dev. Biol. Anim. 52, 68–76 (2016).
Cai, Y. T. et al. Mesenchymal stem cell-secreted factors delayed spermatogenesis injuries induced by busulfan involving intercellular adhesion molecule regulation. Andrologia 51, e13285 (2019).
Ling, L. et al. Human amnion-derived mesenchymal stem cell (hAD-MSC) transplantation improves ovarian function in rats with premature ovarian insufficiency (POI) at least partly through a paracrine mechanism. Stem Cell Res. Ther. 10, 46 (2019).
Hashemi, S. M., Hassan, Z. M., Hossein-Khannazer, N., Pourfathollah, A. A. & Soudi, S. Investigating the route of administration and efficacy of adipose tissue-derived mesenchymal stem cells and conditioned medium in type 1 diabetic mice. Inflammopharmacology 28, 585–601 (2020).
Nagaishi, K., Ataka, K., Echizen, E., Arimura, Y. & Fujimiya, M. Mesenchymal stem cell therapy ameliorates diabetic hepatocyte damage in mice by inhibiting infiltration of bone marrow-derived cells. Hepatology 59, 1816–1829 (2014).
Kim, Y. H. et al. Conditioned medium from tonsil‑derived mesenchymal stem cells promotes adiponectin production. Mol. Med. Rep. 16, 6170–6177 (2017).
Takafuji, Y., Hori, M., Mizuno, T. & Harada-Shiba, M. Humoral factors secreted from adipose tissue-derived mesenchymal stem cells ameliorate atherosclerosis in Ldlr-/- mice. Cardiovasc. Res. 115, 1041–1051 (2019).
Cho, K. A. et al. Conditioned medium from human palatine tonsil mesenchymal stem cells attenuates acute graft‑vs.‑host disease in mice. Mol. Med. Rep. 19, 609–616 (2019).
Tian, J. et al. Mesenchymal stem cell enhances the function of MDSCs in experimental Sjögren syndrome. Front. Immunol. 11, 604607 (2020).
Giri, J., Das, R., Nylen, E., Chinnadurai, R. & Galipeau, J. CCL2 and CXCL12 derived from mesenchymal stromal cells cooperatively polarize IL-10+ tissue macrophages to mitigate gut injury. Cell Rep. 30, 1923–1934.e4 (2020).
Nishikawa, G. et al. Bone marrow-derived mesenchymal stem cells promote colorectal cancer progression via CCR5. Cell Death Dis. 10, 264 (2019).
Karnoub, A. E. et al. Mesenchymal stem cells within tumour stroma promote breast cancer metastasis. Nature 449, 557–563 (2007).
Chen, K. et al. Human MSCs promotes colorectal cancer epithelial-mesenchymal transition and progression via CCL5/β-catenin/Slug pathway. Cell Death Dis. 8, e2819 (2017).
Russell, T. et al. IL-17A and TNF modulate normal human spinal entheseal bone and soft tissue mesenchymal stem cell osteogenesis, adipogenesis, and stromal function. Cells 10, 341 (2021).
Hsieh, C. C., Hsu, S. C., Yao, M. & Huang, D. M. CD9 upregulation-decreased CCL21 secretion in mesenchymal stem cells reduces cancer cell migration. Int. J. Mol. Sci. 22, 1738 (2021).
Halpern, J. L., Kilbarger, A. & Lynch, C. C. Mesenchymal stem cells promote mammary cancer cell migration in vitro via the CXCR2 receptor. Cancer Lett. 308, 91–99 (2011).
Cen, S. et al. Autophagy enhances mesenchymal stem cell-mediated CD4(+) T cell migration and differentiation through CXCL8 and TGF-β1. Stem Cell Res. Ther. 10, 265 (2019).
Dong, F. et al. Myocardial CXCR4 expression is required for mesenchymal stem cell mediated repair following acute myocardial infarction. Circulation 126, 314–324 (2012).
Ikeda, T. et al. Mesenchymal stem cell-derived CXCL16 promotes progression of gastric cancer cells by STAT3-mediated expression of Ror1. Cancer Sci. 111, 1254–1265 (2020).
Giunti, D. et al. Mesenchymal stem cells shape microglia effector functions through the release of CX3CL1. Stem Cells 30, 2044–2053 (2012).
Li, A. et al. Delivery of exogenous proteins by mesenchymal stem cells attenuates early memory deficits in a murine model of Alzheimer’s disease. Neurobiol. Aging 86, 81–91 (2020).
Wang, M. et al. Calcium phosphate altered the cytokine secretion of macrophages and influenced the homing of mesenchymal stem cells. J. Mater. Chem. B 6, 4765–4774 (2018).
Lejmi, E. et al. Inflammatory Chemokines MIP-1δ and MIP-3α Are Involved in the Migration of Multipotent Mesenchymal Stromal Cells Induced by Hepatoma Cells. Stem Cells Dev. 24, 1223–1235 (2015).
Smith, H., Whittall, C., Weksler, B. & Middleton, J. Chemokines stimulate bidirectional migration of human mesenchymal stem cells across bone marrow endothelial cells. Stem Cells Dev. 21, 476–486 (2012).
Sasaki, M. et al. Mesenchymal stem cells are recruited into wounded skin and contribute to wound repair by transdifferentiation into multiple skin cell type. J. Immunol. 180, 2581–2587 (2008).
Ullah, M., Eucker, J., Sittinger, M. & Ringe, J. Mesenchymal stem cells and their chondrogenic differentiated and dedifferentiated progeny express chemokine receptor CCR9 and chemotactically migrate toward CCL25 or serum. Stem Cell Res. Ther. 4, 99 (2013).
Xu, S. et al. Bone marrow-derived mesenchymal stromal cells are attracted by multiple myeloma cell-produced chemokine CCL25 and favor myeloma cell growth in vitro and in vivo. Stem Cells 30, 266–279 (2012).
Alexeev, V., Donahue, A., Uitto, J. & Igoucheva, O. Analysis of chemotactic molecules in bone marrow-derived mesenchymal stem cells and the skin: Ccl27-Ccr10 axis as a basis for targeting to cutaneous tissues. Cytotherapy 15, 171–184.e1 (2013).
Shen, Z. et al. Genetic modification to induce CXCR2 overexpression in mesenchymal stem cells enhances treatment benefits in radiation-induced oral mucositis. Cell Death Dis. 9, 229 (2018).
Almeida, C. R., Caires, H. R., Vasconcelos, D. P. & Barbosa, M. A. NAP-2 Secreted by Human NK Cells Can Stimulate Mesenchymal Stem/Stromal Cell Recruitment. Stem Cell Rep. 6, 466–473 (2016).
Zhang, X. et al. CXCR5-overexpressing mesenchymal stromal cells exhibit enhanced homing and can decrease contact hypersensitivity. Mol. Ther. 25, 1434–1447 (2017).
Acknowledgements
This study was supported by grants from the National Key R&D Program of China (2018YFA0107500, 2021YFA1100600), National Natural Science Foundation of China (81930085, 32150710523 and 31961133024), Jiangsu Province International Science and Technology Cooperation Program (BZ2019017), National Center for International Research-Cambridge-Su Genomic Research Center (2017B01012) and the State Key Laboratory of Radiation Medicine and Protection, Soochow University (GZN1201804 and GZN1201903), Ministry of Health (IDI-IRCCS) & MAECI Italy-China Science and Technology Cooperation (#PGR00961) to E.C.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Han, Y., Yang, J., Fang, J. et al. The secretion profile of mesenchymal stem cells and potential applications in treating human diseases. Sig Transduct Target Ther 7, 92 (2022). https://doi.org/10.1038/s41392-022-00932-0
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41392-022-00932-0
- Springer Nature Limited
This article is cited by
-
Stem cell therapies for neurological disorders: current progress, challenges, and future perspectives
European Journal of Medical Research (2024)
-
The extracts of osteoblast developed from adipose-derived stem cell and its role in osteogenesis
Journal of Orthopaedic Surgery and Research (2024)
-
Modified mesenchymal stromal cells by in vitro transcribed mRNA: a therapeutic strategy for hepatocellular carcinoma
Stem Cell Research & Therapy (2024)
-
Autophagy modulation effect on homotypic transfer of intracellular components via tunneling nanotubes in mesenchymal stem cells
Stem Cell Research & Therapy (2024)
-
Proteomic analysis of cerebrospinal fluid of amyotrophic lateral sclerosis patients in the presence of autologous bone marrow derived mesenchymal stem cells
Stem Cell Research & Therapy (2024)