
Abstract
Objective
Neonatal neurodevelopmental follow-up clinic provides continued surveillance and assessment of high-risk premature infants. We hypothesized that attrition is associated with race and social factors.
Study design
We performed a retrospective cohort study of neonates born at 26–32 weeks gestation who were admitted to a level IV neonatal intensive care unit. Maternal and neonatal characteristics and follow-up attendance were collected. Statistical analysis was performed with significance set at p value < 0.05.
Results
In total, 237 neonates met study criteria. There was a 62% loss to follow-up over 2 years. Factors associated with loss to follow-up included older gestational age, African American race, and maternal cigarette smoking. Protective factors included older maternal age, a neonatal diagnosis of bronchopulmonary dysplasia, and longer hospital length of stay.
Conclusions
Social disparities negatively impact neonatal follow-up clinic attendance. Efforts to identify and target high-risk populations must be started during initial hospitalization before infants are lost to follow-up.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
High-risk neonatal developmental follow-up provides an important transition of care from the inpatient to the outpatient environment [1,2,3]. These clinics specialize in complex neonates, make appropriate referrals to medical subspecialists, and offer specific anticipatory guidance to parents [2, 4,5,6]. In addition, these clinics facilitate referrals to early intervention services, including speech, physical, and occupational therapy [1, 2, 4]. Early intervention services have a positive influence on both cognitive and motor outcomes during infancy, with cognitive benefits persisting into preschool age [7]. Neonatal developmental follow-up is supported by the American Academy of Pediatrics and is a recommended service that all level III and IV neonatal intensive care units (NICUs) should provide [8].
Despite the recognized benefits of neonatal follow-up clinic, attendance has historically been challenging with high rates of attrition [3, 4, 6, 9,10,11,12]. In a recent survey, many sites listed a first visit no-show rate between 10 and 30% with sustained rates of attrition between 10 and 70% on subsequent visits [4]. The reasons for loss to follow-up are multifactorial and include medical, sociodemographic, and maternal factors [4]. Infants with perceived “follow-up difficulty” have higher incidences of severe sensorimotor and cognitive disabilities, even after adjustment for perinatal and sociodemographic variables, and less access to early intervention services [13,14,15,16]. Therefore, identifying patient specific factors that increase loss to follow-up is vital for targeting sustained attendance.
It is known nationally that many urban centers are racially and socioeconomically segregated [17]. There is growing evidence that residential segregation perpetuates health disparities through restricted access to quality health care [18]. There remains a relative gap in knowledge regarding factors driving loss to follow-up in our current healthcare system [3, 10, 12, 19]. We hypothesized that clinic attendance is associated with race and specific maternal social factors, such as insurance status, cigarette smoking, and home location by zip code. The objective of this study was to assess neonatal follow-up attendance and identify maternal and neonatal characteristics associated with attrition.
Methods
Study design
We conducted a retrospective cohort study. Approval was granted through the Children’s Hospital of Wisconsin (CHW) Institutional Review Board with waiver of informed consent.
Study population
Neonates were identified who were born between 26 and 32 weeks gestation and admitted to a level IV NICU in Milwaukee, WI between Januay 1, 2015 and July 31, 2017. Neonates were excluded if they had any chromosomal anomalies, major congenital anomalies (i.e., congenital diaphragmatic hernia, gastroschisis, posterior urethral valves, etc.), if their family was a non-Wisconsin resident, or if they died during the study period.
Our standard practice is to refer all infants born <33 weeks gestation to neonatal follow-up clinic at time of discharge. Families select one of two locations for neonatal follow-up—CHW Main Campus (Milwaukee, WI) or CHW Fox Valley (Neenah, WI). The first appointment is scheduled by either the neonatal nurse practitioner, physician, or inpatient case manager at 3–6 months corrected gestational age (CGA). Families are then called by the clinic to verify timing and availability for the appointment. Prior to discharge, nursing staff reviews all appointments with the family. A neonatal nurse practitioner or physician also verbally addresses the importance of the visit in monitoring developmental progress.
Neonatal follow-up occurs at 3–6, 12, 18, and 24 months CGA. Each visit lasts ~1.5–2 h. At each appointment, a physician within the clinic performs a physical exam focused on neuromotor assessment. A comprehensive team of therapists perform the Bayley Scales of Infant and Toddler Development, Third Edition. Speech, physical, and occupational therapy provide suggestions for the family for targeting developmental milestones. Referrals may be placed for continued early intervention services if a family is not already enrolled. Medical management of complex needs are taken care of by subspecialty services and/or a comprehensive special needs team at a separate visit.
If a family misses an appointment, they are notified via phone pending staff availability; a formal letter is sent to the address listed within the electronic health record.
Data collection
Maternal characteristics included multiple gestation, prenatal steroid administration (partial or complete), cesarean delivery, pre-eclampsia or hypertension, diabetes, race, age, parity, marital status, zip code, insurance type, cigarette smoking, and illegal drug use. Age was divided into four categories: <20 years, 20–29 years, 30–39 years, and >39 years old. Zip code was divided into quartiles based on median household income per year according to United States Census Bureau data collected from the American Community Survey 2017 5-year estimates (https://www.census.gov/acs/www/data/data-tables-and-tools/data-profiles/). Quartiles were defined as follows: $0–29,999; $30,000–56,999; $57,000–83,999; and >$84,000. Insurance type was divided into two categories: Medicaid and private.
Neonatal characteristics included gender, gestational age, hospital length of stay, as well as common medical diagnoses and therapies. These diagnoses or therapies included bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (grade III or IV), periventricular leukomalacia (on head ultrasound or brain magnetic resonance imaging), retinopathy of prematurity (requiring treatment with laser or Avastin), necrotizing enterocolitis, and feeding type at discharge. BPD was defined as a persistent oxygen requirement at 36 weeks CGA. Gestational age was divided into three categories: 26–28, 29–30, and 31–32 weeks. Feeding type at discharge included formula only, breastmilk only, or a combination of formula and breastmilk.
Attendance relative to zip code was plotted utilizing Microsoft Excel 2016 3D-Maps. Reasons for loss to follow-up were collected from chart review and categorized.
Outcome measure
The primary outcome was neonatal follow-up attendance. Neonatal follow-up attendance was tracked at time of discharge (for initial referral placement), at 3–6, 12, 18, and 24 months CGA. Attendance was divided into three groups: 0, 1–2, and 3–4 visits attended over a 24-month period. All infants in the study had aged to 24 months CGA at time of data collection and should have been able to attend four appointments.
We considered infants lost to neonatal follow-up if they did not attend an appointment and were never subsequently evaluated despite recommendations for continued follow-up. This included infants who: (1) were never referred upon discharge from the NICU and (2) were referred upon discharge but due to scheduling conflicts were never evaluated in clinic. If an infant was discharged from neonatal follow-up clinic by 18 months due to continued progress, then we did not consider them lost to follow-up at subsequent appointment intervals.
Statistical analysis
Categorical data were reported as numbers and percentages. Discrete data were reported as medians with 25 and 75th percentiles. The Fisher exact test or the Chi-square test was used to compare categorical variables.
Variables found to be significantly associated with attendance in univariable analysis were further evaluated in multivariable analysis to account for confounding factors. Ordered logistic regression was performed. Variables were controlled for gestational age, multiple gestation, prenatal steroid administration, cesarean delivery, maternal race, maternal age, insurance type, maternal cigarette smoking, BPD, and feeding type at discharge. Odds ratios (OR) of risk factors were given with 95% confidence intervals (CI). Hospital length of stay and follow-up attendance were analyzed with Poisson regression, and incidence rate ratios (IRR) were given with 95% CI. A p value < 0.05 was considered statistically significant.
Kaplan–Meier survival analysis was completed to demonstrate follow-up attendance over the 24-month period.
Statistics were performed in STATA15 (College Station, TX).
Results
Study population
During the study period, 295 infants between 26 and 32 weeks gestation were admitted. In total, 237 infants were included in the study (gestational age-median, 30 weeks; birth weight-mean ± standard deviation, 1417 ± 396 grams). A total of 58 infants were excluded: 39 with major congenital or chromosomal anomalies, 11 with non-Wisconsin parents, and 8 who died in the NICU or within 6 months following discharge.
Sociodemographic and clinical characteristics are summarized in Table 1. Geographical distribution of study participants based upon number of visits attended is shown in Fig. 1. Families who attended no appointments were centered around both medical campuses; those who attended 3–4 appointments were distributed more diffusely across the eastern part of the state.

Top graph represents statewide heat map of patient zip codes who attended 0 appointments over a 24-month period. Bottom graph represents statewide heat map of patient zip codes who attended 3-4 appointments over a 24-month period.
Neonatal follow-up clinic attendance
Follow-up attendance over a 2-year period is shown in Fig. 2. Seven percent of infants were not referred to neonatal follow-up clinic at time of discharge. Attrition between appointments consistently decreased over time from 27 to 6%. By 24 months CGA, 62% of the cohort was lost to follow-up.

X-axis represents month of scheduled follow-up and Y-axis represents proportion of follow-up attendance.
Analysis of factors associated with loss to follow-up
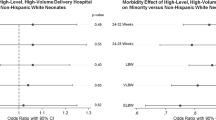
Multiple maternal and neonatal factors were associated with clinic attendance (Table 1). On multivariable analysis, factors associated with loss to neonatal follow-up were a gestational age of 31–32 weeks, maternal African American race, and maternal cigarette smoking (Table 2). Factors associated with attendance included prenatal steroid administration, maternal age between 30 and 39 years, and a neonatal diagnosis of BPD. Longer hospital length of stay was associated with increasing follow-up attendance.
Reasons for loss to follow-up were reviewed and categorized as follows: parent scheduling issues (76.2%); provider scheduling issues (18.4%); parent perception of appropriate development (3.4%); lack of insurance coverage (1.4%); and parent perception of alternate resources (0.6%). Parent scheduling issues included all no-shows and parent cancelation of appointments. Provider scheduling issues included all provider cancelations resulting in loss to neonatal follow-up as well as all situations in which no initial visit was scheduled.
Discussion
Attrition to neonatal follow-up remains a major problem within our health system. We identified a 62% loss to neonatal follow-up over a 2-year time period. This single center, retrospective cohort study highlights that key social factors, such as maternal race, age, and cigarette smoking, as well as specific neonatal factors drive follow-up attendance.
Rates of neonatal follow-up attendance have been shown to vary significantly according to population demographics, study sample, and timing and frequency of follow-up [3, 10,11,12, 20, 21]. Patra et al. evaluated very low birth weight infants and showed that only 52–62% of infants attended their first follow-up visit, with subsequent attendance falling to 27–30% by 2 years [2]. Mas et al. studied infants <33 weeks and demonstrated that only 58% of infants were consistently followed-up at 20–28 months with 27% having never been evaluated [12]. Ballantyne et al. further showcased consistent nonattendance between clinic appointments of 16–26% [3]. Our rate of attrition is in line with these previous studies, demonstrating that neonatal follow-up remains a substantial challenge in today’s landscape. Interestingly, attrition, contrary to being steady, decreased dramatically over consecutive appointments. We speculate that families who perceived consistent value in the appointment were more likely to attend over time.
We identified several potential drivers to loss to neonatal follow-up, including older gestational age, African American race, and maternal cigarette smoking, as well as multiple protective factors, including older maternal age, BPD, and longer hospital length of stay. It is well-recognized that specific social risk factors, such as young maternal age and non-white race, are associated with lower neonatal follow-up attendance [6, 9]. The racial bias we observed may have been impacted by the racial segregation within our city, with those living in certain areas having restricted access to resources [22,23,24,25]. Milwaukee is a racially subdivided city, with its historical roots being greatly driven by highway construction [26]. Most of the inner-city African American population is located to the northwest, primarily in the poorest city zip codes, while the white population resides in the newer gentrified urban developments or city suburbs. Our hospital’s location in the suburbs potentially limits access to care for our most vulnerable inner-city members due to restricted public transportation. Surprisingly, socioeconomic status as represented by insurance status was not predictive of loss to follow-up. This is consistent with Catlett et al. who also found no significant difference in socioeconomic status between attendee and nonattendee families [9]. We speculate that our sample may underrepresent families of low socioeconomic status as multiple level III NICUs in our area provide care to our inner-city population, with those in the poorest zip codes located closer geographically to another health system.
We also demonstrated that older gestational age is associated with loss to neonatal follow-up. Older gestational age infants often have shorter lengths of stay and less complications related to prematurity. Families may perceive these infants as healthy and question their need for developmental follow-up, leading to poor attendance. This was consistent with our review of outpatient documentation, in which families canceled appointments if they perceived appropriate infant development. In addition, this is supported by our findings that infants with greater medical complexity, as inferred by a neonatal diagnosis of BPD and longer length of stay, were more likely to attend clinic. Other common neonatal comorbidities, such as intraventricular hemorrhage and necrotizing enterocolitis were not significant in our study likely due to only a small number of infants being affected. Multiple other studies have demonstrated similar results to ours, emphasizing that infants with longer NICU stays [1], multiple neonatal comorbidities [10, 12, 19], and those whose parents perceive them as “sick” [27, 28] are more likely to attend neonatal follow-up.
Historically, greater distance from the clinic or hospital has been associated with loss to neonatal follow-up [1, 28]. We, in contrast, found that families who attended multiple appointments were geographically located across the state. This suggests that social factors may have played a greater role compared with distance from clinic in our study. Underlying patient characteristics as well as the location of our clinics may account for these differences.
Our reasons for loss to follow-up aligned with and expanded upon categories determined in previous studies [2, 3]. Most infants were lost to neonatal follow-up at ≤12 months CGA due to parent scheduling issues. This brings to question whether parents are truly recognizing the value of neonatal follow-up or if other subspecialty services are taking priority. Efforts should be made to educate families while they are still inpatient on the benefits of and importance of neonatal follow-up clinic. Other interventions can then be undertaken from a clinic perspective to increase attendance.
One of the main strengths of our study was our sample which included infants born from 26 to 32 weeks gestation who were followed longitudinally. Many of the previous studies reporting loss to neonatal follow-up focused only on the extremely premature or extremely low birth weight. The limitations of this study included its retrospective nature which resulted in missing information, such as maternal education or a comprehensive maternal history, as we only had access to the infant’s chart. Reasons for loss to follow-up were also unavailable unless there was specific telephone documentation in the chart, which limits our understanding of why families did not show to appointments. Finally, families that moved to other health systems during the duration of the study were also lost to follow-up due to inability to share medical records, which may have led to incomplete information regarding follow-up attendance.
Since identification of our high rate of attrition, our institution has taken measures to boost neonatal follow-up attendance. All families are now enrolled in MyChart® at time of discharge from the NICU. MyChart® is a secure on-line access portal that sends appointment reminders. Reminder phone calls are also provided within 48 h of all scheduled appointments. Furthermore, we are routing pediatricians our developmental notes as well as sending them electronic messages for all families who do not show. The goal is for the pediatrician to meet with the family to assess development and rerefer to our clinic as needed. Finally, we will provide a developmental brochure to all families prior to discharge that introduces our clinic staff, reviews aspects of the neonatal follow-up visit, and explores the benefits of attendance.
In conclusion, our study confirms that loss to neonatal follow-up continues to be a substantial problem. We identified several potential drivers to loss to follow-up and categorized reasons for nonattendance. Future studies need to be undertaken to see how to best improve follow-up attendance and care for our most vulnerable population.
References
Harmon SL, Conaway M, Sinkin RA, Blackman JA. Factors associated with neonatal intensive care follow-up appointment compliance. Clin Pediatr. 2013;52:389–96.
Patra K, Greene M, Perez B, Silvestri JM. Neonatal high-risk follow-up clinics: how to improve attendance in very low birth weight infants. E- J Neonatol Res. 2014;4:3–13.
Ballantyne M, Stevens B, Guttmann A, Willan AR, Rosenbaum P. Transition to neonatal follow-up programs: is attendance a problem? J Perinat Neonatal Nurs. 2012;26:90–8.
Tang BG, Lee HC, Gray EE, Gould JB, Hintz SR. Programmatic and administrative barriers to high-risk infant follow-up care. Am J Perinatol. 2018;35:940–5.
Dorling JS, Field DJ. Follow up of infants following discharge from the neonatal unit: structure and process. Early Hum Dev. 2006;82:151–6.
Nehra V, Pici M, Visintainer P, Kase JS. Indicators of compliance for developmental follow-up of infants discharged from a regional NICU. J Perinat Med. 2009;37:677–81.
Spittle A, Orton J, Anderson P, Boyd R, Doyle LW. Early developmental intervention programmes post-hospital discharge to prevent motor and cognitive impairments in preterm infants. Cochrane Database Syst Rev. 2012;12:CD005495.
Bockli K, Andrews B, Pellerite M, Meadow W. Trends and challenges in United States neonatal intensive care units follow-up clinics. J Perinatol. 2014;34:71–4.
Catlett AT, Thompson RJ Jr., Johndrow DA, Boshkoff MR. Risk status for dropping out of developmental followup for very low birth weight infants. Public Health Rep. 1993;108:589–94.
J LO, McGinley JL, Fox LM, Spittle AJ. Challenges of neurodevelopmental follow-up for extremely preterm infants at two years. Early Hum Dev. 2015;91:689–94.
Bruni R, Bahamonde LG, Gupta M, Findlay RD, Bean X. Long-term follow up of NICU graduates: social variables, not clinical problems, determine drop-out rates and access to health care † 1215. Pediatr Res. 1998;43:208.
Mas C, Gerardin P, Chirpaz E, Carbonnier M, Mussard C, Samperiz S, et al. Follow-up at two years of age and early predictors of non-compliance in a cohort of very preterm infants. Early Hum Dev. 2017;108:1–7.
Tin W, Fritz S, Wariyar U, Hey E. Outcome of very preterm birth: children reviewed with ease at 2 years differ from those followed up with difficulty. Arch Dis Child Fetal Neonatal Ed. 1998;79:F83–7.
Callanan C, Doyle L, Rickards A, Kelly E, Ford G, Davis N. Children followed with difficulty: how do they differ? J Paediatr Child Health. 2001;37:152–6.
Wolke D, Söhne B, Ohrt B, Riegel K. Follow-up of preterm children: important to document dropouts. Lancet. 1995;345:447.
Slater MA, Naqvi M, Andrew L, Haynes K. Neurodevelopment of monitored versus nonmonitored very low birth weight infants: the importance of family influences. J Dev Behav Pediatr. 1987;8:278–85.
Williams DR, Collins C. Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Rep. 2001;116:404–16.
Bailey ZD, Krieger N, Agenor M, Graves J, Linos N, Bassett MT. Structural racism and health inequities in the USA: evidence and interventions. Lancet. 2017;389:1453–63.
Kim NH, Youn YA, Cho SJ, Hwang JH, Kim EK, Kim EA, et al. The predictors for the non-compliance to follow-up among very low birth weight infants in the Korean neonatal network. PLoS ONE. 2018;13:e0204421.
Guillen U, DeMauro S, Ma L, Zupancic J, Roberts R, Schmidt B, et al. Relationship between attrition and neurodevelopmental impairment rates in extremely preterm infants at 18 to 24 months: a systematic review. Arch Pediatr Adolesc Med. 2012;166:178–84.
Vohr BR, Wright LL, Dusick AM, Perritt R, Poole WK, Tyson JE, et al. Center differences and outcomes of extremely low birth weight infants. Pediatrics. 2004;113:781–9.
Logan JR The Persistence of Segregation in the 21(st) Century Metropolis. City Community 2013, 12. https://doi.org/10.1111/cico.12021.
Willis E, McManus P, Magallanes N, Johnson S, Majnik A. Conquering racial disparities in perinatal outcomes. Clin Perinatol. 2014;41:847–75.
Johnson S, Dickinson K, Mandic CG, Willis E. Community matters for children’s health. Pediatr Ann. 2011;40:152–60.
Byrd DR, Katcher ML, Peppard P, Durkin M, Remington PL. Infant mortality: explaining Black/White disparities in Wisconsin. Matern Child Health J. 2007;11:319–26.
Chi G, Parisi D. Highway expansion effects on urban racial redistribution in the post—civil rights period. Public Works Manag Policy. 2011;16:40–58.
Ballantyne M, Benzies K, Rosenbaum P, Lodha A. Mothers’ and health care providers’ perspectives of the barriers and facilitators to attendance at Canadian neonatal follow-up programs. Child Care Health Dev. 2015;41:722–33.
Ballantyne M, Stevens B, Guttmann A, Willan AR, Rosenbaum P. Maternal and infant predictors of attendance at neonatal follow-up programmes. Child Care Health Dev. 2014;40:250–8.
Acknowledgements
Statistical support was provided through the Division of Quantitative Health Sciences. This study was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant Number UL1TR001436. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. We would like to thank the MCW Division of Neonatology and the members of the CHW Neonatal Neurocritical Care Program for their support.
Funding
This study was also supported by internal funding through MCW Department of Pediatrics.
Author information
Authors and Affiliations
Contributions
CS designed the study and wrote the manuscript with guidance from EC and SC. EC performed the statistical analysis with oversight from the Division of Quantitative Health Sciences.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Swearingen, C., Simpson, P., Cabacungan, E. et al. Social disparities negatively impact neonatal follow-up clinic attendance of premature infants discharged from the neonatal intensive care unit. J Perinatol 40, 790–797 (2020). https://doi.org/10.1038/s41372-020-0659-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-020-0659-4
- Springer Nature America, Inc.
This article is cited by
-
Developing a practical neurodevelopmental prediction model for targeting high-risk very preterm infants during visit after NICU: a retrospective national longitudinal cohort study
BMC Medicine (2024)
-
Families as partners in neonatal neuro-critical care programs
Pediatric Research (2024)
-
Racial and ethnic socioenvironmental inequity and neuroimaging in psychiatry: a brief review of the past and recommendations for the future
Neuropsychopharmacology (2024)
-
Identifying barriers and facilitators to care for infants with bronchopulmonary dysplasia after NICU discharge: a prospective study of parents and clinical stakeholders
Journal of Perinatology (2024)
-
Socioeconomic disparities in the postnatal growth of preterm infants: a systematic review
Pediatric Research (2024)