
Abstract
Background
The gut microbiota has been associated with overweight and obesity in adults, but the evidence in children is limited. Our aim was to study whether composition of the gut microbiota at the age of 3 years is associated with overweight/obesity in children cross-sectionally.
Methods
Children, who participated in a clinical trial of prenatal vitamin-D supplementation (VDAART), underwent standardized height and weight measurements, and collection of stool samples at 3 years of age. 16 S rRNA sequencing (V4 region) of the stool samples were performed with Illumina MiSeq. Associations between microbiota and overweight/obesity (body mass index z-scores >85th percentile) was analyzed using logistic regression.
Results
Out of 502 children, 146 (29%) were categorized as overweight/obese. Maternal pre-pregnancy BMI, birth weight and length, formula feeding during the first year, high frequency of fast food consumption, and time watching TV or computer screen at 3 years were the risk factors for overweight/obesity. Of the top 20 most abundant genera, high relative abundance of Parabacteroidetes (Bacteroidetes; Bacteroidales) (aOR(95% CI): 0.69 (0.53, 0.90, p = 0.007) per interquartile increase) and unassigned genus within Peptostreptococcae family were inversely associated with overweight/obesity, whereas high relative abundance of Dorea (Firmicutes;Clostridiales) (1.23 (1.05, 1.43, p = 0.009)) was positively associated. Associations were independent of each other. No associations were found between diversity indices and overweight/obesity.
Conclusions
Our data suggest that some of the differences in gut composition of bacteria between obese and non-obese adults can already be observed in 3-year old children. Longitudinal studies will be needed to determine long-term effects.
Similar content being viewed by others


Introduction
Obesity is a worldwide public health concern and is a known risk factor for several diseases such as diabetes, cardiovascular diseases, and cancer [1]. The prevalence of obesity in children and adults is increasing in both developed and developing countries. Overweight and obese children are prone to become obese adults, and obesity in childhood may be a risk factor for cardiovascular disease in adulthood due to increased blood pressure and decrease in high-density lipoprotein cholesterol (HDL) mediated by body mass index (BMI) in adulthood [2].
Risk factors for childhood overweight/obesity reported in the literature include, among others: parental (especially maternal) obesity [3, 4], C-section delivery, formula feeding, antibiotic treatment (both in utero and after birth) [5], smoking during pregnancy and low maternal educational level [3]. High fat/carbohydrate diet, low physical activity, and time spent at the computer/TV are additional often correlated risk factors associated with child adiposity [6,7,8]. Many of these recognized adiposity risk factors have been hypothesized to influence the risk of overweight and obesity by directly or indirectly influencing the composition of the intestinal microbiota and the contribution of those microbiota to a pro-obesogenic breakdown and metabolism of foods [9].
Previous studies have suggested that diversity of the gut microbiota is inversely associated with overweight/obesity [10]. Bacteroidetes/Firmicutes ratio has previously been associated with obesity; however, a recent meta-analysis of mostly adult studies did not find any association [11]. Other studies among adults have identified bacterial taxa that may be associated with overweight/obesity. The levels of Bacteroidetes [12,13,14,15] and its genera Bacteroides [15, 16], Bacteroides-Prevotella group [17, 18], and Bifidobacterium [13, 16, 19,20,21] as well as Methanobrevibacter (Archaea) have been shown to be decreased in gut microbiota of overweight or obese adults, whereas species in Lactobacillus [12, 13, 15, 17, 20] and Roseburia [15, 22] have been enriched. Not all the results have been consistent [19, 23]. Studies in children above 3 years of age have identified similar taxa, especially Bacteroides or Bacteroides/Prevotella group [24,25,26,27] that have been associated with overweight/obesity and in addition, have observed that obesity is associated with lower levels Akkermansia muciniphila [26, 28]. Associations between Faecalibacterium prausnitzii in the gut and overweight/obesity have been inconsistent [24, 26, 27, 29, 30].
We have recently shown that C-section birth was related to higher Shannon diversity index (which takes account both community richness [a simple count of the number of species or number of Operational Taxonomic Units, OTUs, in a sample] and evenness [how equal the abundances of the species or OTUs are]), higher levels of Firmicutes and Proteobacteria coabundance scores, and lower levels of Bacteroidetes scores; and breastfeeding with lower level of Clostridiales in the gut sample collected at the age of 3–6 months [31]. Due to the link between C-section and the risk of overweight/obesity [5], these taxa might be related to the development of overweight and obesity.
Our overall objective was to determine whether gut microbiota among 3-year-old children are associated with overweight/obesity at the same age. In addition, we tested whether other covariates, that may predict overweight/obesity, mediates the observed association between bacterial genera and overweight/obesity in this cross sectional analysis at the age of 3 years.
Methods
The study population consisted of children, who participated in the VDAART clinical trial (The Vitamin D Antenatal Asthma Reduction Trial), a two arm, double-blind, placebo controlled, randomized, clinical trial of vitamin D supplementation in the pregnant mother to prevent asthma and allergy in childhood in three clinical centers across the United States – Boston, MA, St. Louis, MO, and San Diego, CA [32]. Pregnant women, who either had a personal history of or whose partner had a history of allergies/asthma, were randomized (n = 880) during the first trimester of pregnancy (10–18 weeks) to one of two treatment arms of a 4-year clinical trial: 4000 IU Vitamin D + prenatal vitamins or 400 IU Vitamin D + prenatal vitamins. VDAART was approved by the Institutional Review Boards (IRB: 2009P000557) of the participating Clinical Centers and the Data Coordinating Center, with pregnant women signing informed consent at the first enrollment visit. A total of 502 children, who had stool samples and information on height and weight at the age of 3 years, were included into the present study.
Maternal pre-pregnancy BMI was ascertained by medical chart review. Questionnaires regarding baseline characteristics (e.g. maternal age, marital status, smoking during pregnancy, family income, and parental race/ethnicity) were administered at enrollment. Child’s race/ethnicity was based on parental report. Information on child’s gender, birth weight and height, and mode of delivery was abstracted from labor and delivery records [33]. Children were followed up with repeated quarterly questionnaires from the age of 3 months, including questions about breast- and formula-feeding, antibiotic treatment, time spent watching TV or computer screen, sleeping time and time for active play separately on the weekdays and on weekends. Frequency of fast food consumption at the age of 3 years was asked using a question “How often has child eaten something from a fast food restaurant in the last month?”. At yearly visits, weight and height were measured in a standardized fashion. Two people measured standing height using the Shorr Length Board®.
BMI based z-score
Age- and sex-specific BMI z-scores and percentiles using national reference data were calculated using CDC SAS Macro (A SAS Program for the 2 000 CDC Growth Charts) [34]. Children were classified as overweight/obese if their BMI z-score percentile was greater than the 85th percentile.
Diet in the past month in the 3-year follow-up
In the 3-year questionnaire, parents were asked about children’s diet for the past month using total of 87 questions of intake frequency of different food items. Due to missing data, two diet scores were created by Principal component analyses (PCA) using VARIMAX rotation with 41 variables without missing data (n = 502) and with total of 87 variables with missing data (n = 378). In both PCAs, score 1 was related mostly with unhealthy food and desserts (e.g. white bread, fried chicken and brownies) whereas score 2 was related to healthy food (e.g. fruits and vegetables). PCA scores (1 and 2) of the 87 variables correlated highly with PCA scores (1 and 2) of 41 variables (n = 378, r = 0.92 and 0.81, respectively), and thus, PCA scores of the 41 variables were used in the further analyses.
Assessment of vitamin-D status
Measurement of 25-hydroxyvitamin D [25(OH)D] has been described previously. Briefly, at the age of 3 years, circulating 25(OH)D was determined using DiaSorin Liaison® (see Supplemental Material) [32, 33].
Stool sample collection and sequencing
The methods of stool sample collection and sequencing are described in the Supplemental Material in detail. Briefly, the child’s stool sample was collected by parents and samples were stored in freezers until processing. Stool samples were not collected if the child received any oral antibiotics in the previous 7 days. DNA extraction was performed on stool samples, and the bacterial 16 S rRNA sequencing (V4 region) was performed with the Illumina MiSeq. A total of 506 children’s stool samples were collected and out of those, 502 also had information on BMI (mean age 36.1 months; age range 33.2–41.1 months).
Relative abundance of taxa, diversity indices, and functional pathways
One read per operational taxonomic unit (OTU) were filtered from the OTU table. The average (SD) number of raw reads (>1read/OTU) across all samples was 51,713 (mean ± SD = 51,713 ± 21,756). The measurements of bacteria/archaea were based on relative abundance i.e. the percentage of reads of a taxon per the total reads in a sample. For adjusted models, the relative abundances of genera were log-transformed (natural logarithm) and divided by range between 25th and 75th percentiles per genus. Shannon diversity index (which takes account both community richness [a simple count of the number of species or number of OTUs in a sample] and evenness [how equal the abundances of the species or OTUs are]) and richness (total number of observed OTUs in a sample) were measured from 35,089 OTUs with the Vegan package in RStudio. In total, taxa from 13 phyla, 45 orders, 102 families and 244 genera were identified. Taxonomy is only the first step in considering how gut microbes may lead to child adiposity, and we are interested in the inferred function of the microbial communities, as this is another step towards understanding the biology underlying taxonomic associations. Thus, Phylogenetic Investigation of Communities by Reconstruction of Unobserved States (PICRUSt) was used to impute the functional metagenome (KEGG pathways) (see Supplemental Material) [35].
Statistical analyses
Chi-square analysis was used for comparison between determinants and overweight/obesity to identify possible confounding factors. Mann–Whitney U test were used for comparisons between the relative abundances of phyla or top 20 most abundant genera among children who were overweight/obese and non-overweight/non-obese children and for comparisons between relative abundance of Dorea and time spent watching TV or computer screen, or consumption of fast food among children who were overweight/obese and non-overweight/non-obese children. Spearman’s correlation coefficients were calculated. Logistic regression models (adjusted for maternal education level) were used to determine associations between an interquartile range increase in natural log-transformed bacterial abundance and odds of overweight/obesity at age 3. All the models were adjusted for maternal education level. Other potential confounders for the association between the gut microbiome and overweight/obesity were examined (all determinants with p-values <0.2 shown in Table 1), but they did not change the estimates, and so were not analyzed further. In addition, the models for diversity indices and overweigh/obesity were adjusted for sampling age. The results are presented as adjusted odds ratios (aORs) and their 95% confidence intervals (95% CI). Two-sided p < 0.05 was considered significant. In the sensitivity analysis, 21 (4%) underweight children (BMI z-score percentile was the 5th percentile or lower) were excluded from the reference (non-overweight/non-obesity) group. Bonferroni correction was used for multiple testing. The data were analyzed using SAS 9 (SAS Institute Inc., Cary, NC, USA).
Results
Risk factors for overweight/obesity
Out of 502 children, 146 (29%) children were defined as overweight or obese. Half of the children were African Americans and 32% were white. Several maternal and child determinants for child overweight/obesity were identified (p-values < 0.2 in X2-test, Table 1). After adjustment for maternal education level, maternal pre-pregnancy obesity, higher birth weight and length, formula feeding during the first year, high frequency of fast food consumption and time spent watching TV or computer screen at 3 years were the risk factors for overweight/obesity (Table 1). No associations were found between child overweight/obesity and gender, race, maternal age, marital status, mode of delivery, vitamin D level at birth (25(OH)D levels ≥30 ng/mL vs. <30 ng/mL) or at the age of 3 years, breastfeeding, antibiotic treatment until the age of 3 years (Table 1), the number of courses of antibiotics since birth (Supplemental material Table E1), smoking during pregnancy, family income, antibiotic treatment during delivery, preterm delivery (<37 weeks of the gestation), sleeping time during weekends or weekdays, and time for active play during weekends or weekdays (data not shown). Time spent watching TV or computer screen during weekends tended to have similar effect as for weekdays, but it was weaker (data not shown). PCA factors 1 (data not shown) and 2 (Table 1) of diet did not have clear dose-response effect on overweight/obesity.
Bacterial phyla, Firmicutes/Bacteroidetes ratio vs. overweight/obesity
At the phylum level, the most abundant phyla were Firmicutes (mean relative abundance 62.4%) and Bacteroidetes (24.2%), which made up the highest proportion of relative abundances of 13 phyla followed with lower levels of Actinobacteria (8.9%), Proteobacteria (2.2%) and Verrucomicrobia (2.1%). None of the relative abundances of the top abundant phyla were statistically different between children who were overweight/obese and non-overweight/non-obese children (p > 0.2), except Verrucomicrobia, which had the same association as Akkermansia genus (below), as it was the only genus within Verrucomicrobia that was detected (mean relative abundances: overweight/obesity 1.6% vs. non-overweight/non-obesity 2.3%, p-value 0.03). Tertiles of Firmicutes/Bacteroidetes ratio were not associated with overweight/obesity (aOR (95% CI) 1.41 (0.87, 2.27) for middle tertile and 1.08 (0.66, 1.76) for the highest tertile vs. the lowest tertile).
Top 20 most abundant genera vs. overweight/obesity
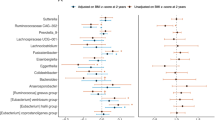
At the genus level, the majority of the top 20 most abundant genera belonged to the Firmicutes phylum, and the genera were mainly within the Clostridiales order (Table 2). When the relative abundances of the top 20 genera were compared, the levels of Ruminococcus, Akkermansia, and Parabacteroidetes were lower and the level of Dorea were higher (Mann–Whitney U test, p < 0.05) in children who were overweight/obese as compared to non-overweight/non-obese children (Fig. 1). The majority of correlation coefficients within the top 20 abundant genera were between −0.3 and 0.3 (see in the Supplemental material Table E2). The highest correlations were found between Coprococcus and an unassigned genus within Lachnospiraceae family (U. from now on) and Clostridiales U. (r = 0.54 and 0.51, respectively).

Mean relative abundances of the top 20 bacterial genera of a) overweight/obese and b) non-overweight/non-obese children. The rest of the genera have been summed up into a group ‘Rest’. Percentage of the relative abundances in overweight/obese vs. non-overweight/non-obese children are in parentheses. *p-value < 0.05 from Mann–Whitney U test
Seven out of 20 genera were associated with overweight/obesity (p < 0.1) after adjusting for maternal education level (Table 3). High relative abundances of Parabacteroidetes (Bacteroidetes; Bacteroidales) and Peptostreptococcae U. (Firmicutes;Clostridiales) were inversely associated with overweight/obesity, and similar tendency were seen with Ruminococcus (Firmicutes; Clostridiales) and Akkermansia (Verrucomicrobia;Verrucomicrobiales) (Table 3). High relative abundance of Dorea (Firmicutes;Clostridiales) was positively associated with overweight/obesity and similar tendency were seen with relative abundances of Streptococcus (Firmicutes; Lactobacillales) and Roseburia (Firmicutes;Clostridiales). When multiple testing was taken account, none of the associations retained their significance (p-values for Parabacteroidetes 0.14 and for Dorea 0.17), except in sensitivity analyses when underweight children were excluded from the reference group (see below).
Within Lachnospiraceae family, Dorea was one of the 6 studied genera, which all tended to be risk factors for overweight/obesity (Table 3). However, the relative abundance of Lachnospiraceae family was not significantly associated with overweight/obesity (aOR (95% CI) 1.22 (0.93, 1.60) per interquartile increase, p = 0.15). No significant changes were observed in the estimates, when the models were additionally adjusted for the frequency of fast food consumption (Table 4), or for race, maternal pre-pregnancy BMI or other known risk factors (listed in the Table 1) for overweight/obesity (data not shown), or when all 7 genera were mutually adjusted (Table 4).
Diversity indices and overweight/obesity
The mean and standard deviation of Shannon diversity index and richness were 5.01 ± 0.47 (range 3.24–5.92) and 2 842 ± 771 (range, 66–7133), respectively. No associations were found with Shannon index or richness and overweight/obesity (see the Supplement material, Table E3).
Levels of relative abundance of Dorea and overweight/obesity
Relative abundance of Dorea was higher in children who were overweight/obese compared to children who were non-overweight/non-obese if the children watched TV or computer screen 1 h/day or more on weekdays (see Supplemental material, Figure E1). Relative abundance of Dorea was higher in children who were overweight/obese compared to children who were non-overweight/obese, if the children consumed fast food once per week (see Supplemental material, Figure E2). Associations between diet, antibiotic treatment and TV watching and high levels (>median) of Dorea, Roseburia, Peptostreptococcae U., and Akkermansia are reported in the supplemental material (Supplement material, Table E4).
Effect modification on diet and time spent watching TV or computer screen
None of the associations between the relative abundances of seven genera and overweight/obesity were modified by breast- or formula feeding, the frequency of fast food consumption or time spent watching TV or computer screen (Supplemental material, Table E5) i.e. the estimates did not considerably change when the models were adjusted with the suggested effect modifiers.
Functional pathways
G protein-coupled receptors, fatty acid elongation in mitochondria, fatty acid metabolism or biosynthesis, that have previously been linked to overweight/obesity [36, 37], were analyzed. The first two were rare in children (majority were not detected). None of the analyzed four pathways were associated with overweight/obesity, except fatty acid elongation in mitochondria, which tended to be inversely associated with overweight/obesity (Supplemental material, Table E6). Fatty acid elongation in mitochondria was not associated with the relative abundance of Dorea, Parabacteroidetes or Peptostreptococcae U. (data not shown).
Sensitivity analyses
When underweights excluded from the reference group, the association between relative abundance of Dorea and overweight/obesity became stronger (aOR (95% CI) 1.31 (1.11, 1.55) per interquartile increase, p = 0.0013) and its significance remained when multiple testing was taken account (p = 0.03) (see the Supplemental material, Table E7).
Race and sex
Ethnic and gender differences were tested using interaction term in the model. Analyses suggested that in some cases associations of relative abundances of Parabacteroides, Dorea and Roseburia with overweight/obesity were stronger for non-white children than for white children (Supplemental Table E8), and also stronger in boys than in girls (Supplemental Table E9).
Discussion
Almost one third of the 502 3-year-old children that participated in this study were categorized as overweight/ obese. Maternal pre-pregnancy BMI, high birth weight and length, formula feeding during the first year, high frequency of fast food consumption, and time spent watching TV or computer screen at 3 years were the risk factors for overweight/obesity. Of the top 20 most abundant enteral microbiome genera, high relative abundance of Parabacteroidetes and Peptostreptococcae U. were inversely associated with overweight/obesity, whereas high relative abundance of Dorea was positively associated with overweight/obesity. Time spent watching TV or a computer screen on weekdays was positively associated with high levels of Dorea and similar tendency was seen with high frequency of fast food consumption. No associations were found with Shannon index or richness and overweight/obesity.
Risk factors for overweight/obesity
We found similar risk factors for overweight/obesity that have been reported previously. The strongest risk factor with dose-response was the frequency of consumption of fast food, as was found recently in the cross-sectional study among 72,900 children from 17 countries [38]. Pre-pregnancy maternal obesity (BMI ≥ 30), high birth weight and height, and formula feeding were associated with the risk of overweight/obesity, as has been shown in previous studies [5]. In contrast to previous studies, C-section birth mode was not a significant risk factor for overweight/obesity in the present study or in the Danish birth cohort study [39]. Families should be guided to eat more healthy foods and minimize fast foods to attempt to prevent overweight/obesity in early childhood.
Depleted genera in overweight/obesity
High proportions of Parabacteroidetes and Peptostreptococcae U. were inversely associated with overweight/obesity. In addition, we found a tendency that the relative abundances of Ruminococcous and Akkermansia were inversely associated with overweight/obesity. No other studies have linked Peptostreptococcae U. with lean children/adults. In line with our results, case-control studies in adults and older children (mostly Caucasians) have found similar inverse association between Parabacteroidetes [15, 27], Ruminococcous [19], and Akkermansia, and overweight/obesity [26, 28]. In contrast to our results, in a case-control study among Japanese adults, Ruminococcus bromii and obeum were enriched in obese adults, where the non-obese comparison group was defined as borderline underweight (the mean BMI 18.6 kg/m2) [40]. Comparison between studies may be difficult when the sample collection age, ethnicity of the study populations, methodologies for sample handling, extraction, and sequencing technologies can vary between studies. The knowledge of the association between gut microbiota and obesity is limited, especially in children: most of the previous studies have used quantitative polymerase chain reactions (qPCRs), which quantify the targeted taxa, however, the method does not describe and quantify any other taxa that are not targeted a priori.
Dorea and overweight/obesity
In line with our findings, higher level of Dorea formicigenerans was associated with overweight/obesity in adults [15]. Our NGS sequencing method was not able to go further than genus level. However, when Dorea with 5 other genera within Lachnospiraceae family, which tended to be associated with overweight/obesity, was analyzed, the relative abundance of Lachnospiraceae (at the family level) was not associated with overweight/obesity. In contrast, a recent birth cohort study from Canada (2/3 Caucasian mothers) with earlier collected stool samples (at the age of 3–4 months) showed that higher levels of relative abundance of Lachnospiraceae family was associated with overweight at the age of 12 months, but no association was found with samples collected at the age of 12 months [41]. A higher level of taxonomy may increase the background noise thus reducing any association. Other analytical methods, such as qPCR are needed to increase the accuracy of the taxa. Also, larger sample sizes are needed for studies in the future.
Diet, antibiotic treatment, and consumption of fast food and 7 genera
Diet and antibiotic treatment were not associated with seven genera (Parabacteroidetes, Dorea, Roseburia, Ruminococcus, Peptostreptococcae U., Streptococcus, and Akkermansia), even though they were associated directly with overweight/obesity. Interestingly in a recent early-life high-fat diet mouse model found that the diet decreased the relative abundances of Bifidobacterium and Akkermansia, and increased the level of Dorea [42]. In addition, none of the risk factors modified the effects between the relative abundances of the seven genera and the presence of overweight/obesity. One reason that no effect modification was observed might be that we restricted the analyses to only the most abundant 20 genera, which may not include the taxa that might have been modified by diet and antibiotic treatments. In addition, as have been seen with dietary intervention studies, the responses might be seen only at the species level [10]. Also, we had a cross-sectional data set: early childhood dietary determinants e.g. breastfeeding may not have strong effect on 3-year gut microbiota; even though they are risk factors for overweight/obesity at the same age.
Gut microbiota
The gut microbiota changes with time, and it has been found to reach adulthood-like microbiota between ages 2–3 years. However, it has been suggested that the development of microbiota might undergo change for even longer [43]. Changes in the microbiota are most related to diet when infants start to ingest solid food. In the present study, the dominant phyla were Firmicutes followed by Bacteroidetes, as has been found also in adult studies [44].
Obesity is associated with low-grade inflammation [45]. It has been suggested that the lipopolysaccharide (LPS), that is a part of the outer membrane structure in gram-negative bacteria, stimulates inflammation [46]. LPS is produced and released continuously in the gut, when membranes of cells of gram-negative bacteria are broken down. It has also been shown that there are structural differences in LPS generation by various stimuli [47] resulting in variation in immunological markers such as pro-inflammatory cytokines [45].
In the U.S., both Type 2 diabetes mellitus and obesity have skyrocketed. Thus, future work on the relation of gut microbiota to childhood adiposity may have relevance for understanding the etiology of both obesity and Type 2 diabetes mellitus [48].
The main strength of the present study is the objectively measured height and weight, as well as high resolution next generation microbiome sequencing data. Gut microbiome samples were collected in 3-year-old children. At that age, the gut microbiota is generally established and reflects an adult-like microbiome. A weakness of the study is the cross-sectional study design, in which causality of the associations cannot be verified. We cannot rule out that social desirability bias, which may affect subjective study measures such as dietary assessment, physical activity and screen time, could influence our study results. A general weakness of currently applied next generation amplicon sequencing methods is that the taxonomic resolution to the species level is hardly ever possible. However, the method described overall gut microbiota, and not just the prior targeted taxa that have been analyzed previously with qPCRs.
In conclusion, our data show that some of the differences in gut composition of bacteria between obese and non-obese adults can also be observed in 3-year old children. This suggests that changes in the gut microbiome that may predispose to adult obesity begin in early childhood. Further follow-up will determine whether these differences become more pronounced as the children get older and additional studies will be needed to identify possible mechanisms by which the gut microbiome composition predisposes to obesity.
References
Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81. https://doi.org/10.1016/S0140-6736(14)60460-8.
Umer A, Kelley GA, Cottrell LE, Giacobbi P,Jr, Innes KE, Lilly CL. Childhood obesity and adult cardiovascular disease risk factors: a systematic review with meta-analysis. BMC Public Health. 2017;17:683.
Morgen CS, Angquist L, Baker JL, Andersen AM, Michaelsen KF, Sorensen TIA. Prenatal risk factors influencing childhood BMI and overweight independent of birth weight and infancy BMI-a path analysis within the Danish National Birth Cohort. Int J Obes (Lond) 2017;42:594–602. https://doi.org/10.1038/ijo.2017.217.
Vos MB, Welsh J. Childhood obesity: update on predisposing factors and prevention strategies. Curr Gastroenterol Rep. 2010;12:280–7.
Mueller NT, Whyatt R, Hoepner L, Oberfield S, Dominguez-Bello MG, Widen EM et al. Prenatal exposure to antibiotics, cesarean section and risk of childhood obesity. Int J Obes. 2015;39:665–70. https://doi.org/10.1038/ijo.2014.180.
Francis L, Shodeinde L, Black MM, Allen J. Examining the obesogenic attributes of the family child care home environment: a literature review. J Obes. 2018;2018:3490651. https://doi.org/10.1155/2018/3490651.
Taverno Ross SE, Macia L, Documet PI, Escribano C, Kazemi Naderi T, Smith-Tapia I. Latino parents’ perceptions of physical activity and healthy eating: at the intersection of culture, family, and health. J Nutr Educ Behav. 2018;50:968–76.
Sanchez M, Panahi S, Tremblay A. Childhood obesity: a role for gut microbiota? Int J Environ Res Public Health. 2014;12:162–75.
Shore SA, Cho Y. Obesity and asthma: microbiome-metabolome interactions. Am J Respir Cell Mol Biol. 2016;54:609–17.
Sonnenburg JL, Backhed F. Diet-microbiota interactions as moderators of human metabolism. Nature. 2016;535:56–64.
Walters WA, Xu Z, Knight R. Meta-analyses of human gut microbes associated with obesity and IBD. FEBS Lett. 2014;588:4223–33.
Armougom F, Henry M, Vialettes B, Raccah D, Raoult D. Monitoring bacterial community of human gut microbiota reveals an increase in Lactobacillus in obese patients and Methanogens in anorexic patients. PLoS One. 2009;4:e7125.
Million M, Angelakis E, Maraninchi M, et al. Correlation between body mass index and gut concentrations of Lactobacillus reuteri, Bifidobacterium animalis, Methanobrevibacter smithii and Escherichia coli. Int J Obes. 2013;37:1460–6.
Turnbaugh PJ, Hamady M, Yatsunenko T, et al. A core gut microbiome in obese and lean twins. Nature. 2009;457:480–4.
Verdam FJ, Fuentes S, de Jonge C, et al. Human intestinal microbiota composition is associated with local and systemic inflammation in obesity. Obesity (Silver Spring). 2013;21:E607–15. https://doi.org/10.1002/oby.20466.
Santacruz A, Collado MC, Garcia-Valdes L, et al. Gut microbiota composition is associated with body weight, weight gain and biochemical parameters in pregnant women. Br J Nutr. 2010;104:83–92. https://doi.org/10.1017/S0007114510000176.
Ferrer M, Ruiz A, Lanza F, et al. Microbiota from the distal guts of lean and obese adolescents exhibit partial functional redundancy besides clear differences in community structure. Environ Microbiol. 2013;15:211–26.
Furet JP, Kong LC, Tap J, et al. Differential adaptation of human gut microbiota to bariatric surgery-induced weight loss: links with metabolic and low-grade inflammation markers. Diabetes. 2010;59:3049–57.
Schwiertz A, Taras D, Schafer K, Beijer S, Bos NA, Donus C, et al. and SCFA in lean and overweight healthy subjects. Obesity (Silver Spring). 2010;18:190–5.
Million M, Lagier JC, Yahav D, Paul M. Gut bacterial microbiota and obesity. Clin Microbiol Infect. 2013;19:305–13.
Mayorga Reyes L, Gonzalez Vazquez R, Cruz Arroyo SM, et al. Correlation between diet and gut bacteria in a population of young adults. Int J Food Sci Nutr. 2016;67:470–8.
Tims S, Derom C, Jonkers DM, et al. Microbiota conservation and BMI signatures in adult monozygotic twins. ISME J. 2013;7:707–17.
Patil DP, Dhotre DP, Chavan SG, et al. Molecular analysis of gut microbiota in obesity among Indian individuals. J Biosci. 2012;37:647–57.
Riva A, Borgo F, Lassandro C, Verduci E, Morace G, Borghi E, et al. Pediatric obesity is associated with an altered gut microbiota and discordant shifts in Firmicutes populations. Environ Microbiol. 2017;19:95–105.
Bervoets L, Van Hoorenbeeck K, Kortleven I. et al. Differences in gut microbiota composition between obese and lean children: a cross-sectional study. Gut Pathog. 2013;5:10.
Borgo F, Verduci E, Riva A, Lassandro C, Riva E, Morace G, et al. Relative abundance in bacterial and fungal gut microbes in obese children: a case control study. Child Obes. 2017;13:78–84. https://doi.org/10.1089/chi.2015.0194.
Hu HJ, Park SG, Jang HB, et al. Obesity alters the microbial community profile in Korean adolescents. PLoS One. 2015;10:e0134333.
Karlsson CL, Onnerfalt J, Xu J, Molin G, Ahrne S, Thorngren-Jerneck K. The microbiota of the gut in preschool children with normal and excessive body weight. Obesity (Silver Spring). 2012;20:2257–61.
Payne AN, Chassard C, Zimmermann M, Muller P, Stinca S, Lacroix C. The metabolic activity of gut microbiota in obese children is increased compared with normal-weight children and exhibits more exhaustive substrate utilization. Nutr Diabetes. 2011;1:e12.
Balamurugan R, George G, Kabeerdoss J, Hepsiba J, Chandragunasekaran AM, Ramakrishna BS. Quantitative differences in intestinal Faecalibacterium prausnitzii in obese Indian children. Br J Nutr. 2010;103:335–8.
Sordillo JE, Zhou Y, McGeachie MJ. et al. Factors influencing the infant gut microbiome at age 3-6 months: findings from the ethnically diverse Vitamin D Antenatal Asthma Reduction Trial (VDAART). J Allergy Clin Immunol. 2017;139:482–91.
Litonjua AA, Lange NE, Carey VJ, et al. The Vitamin D Antenatal Asthma Reduction Trial (VDAART): rationale, design, and methods of a randomized, controlled trial of vitamin D supplementation in pregnancy for the primary prevention of asthma and allergies in children. Contemp Clin Trials. 2014;38:37–50.
Litonjua AA, Carey VJ, Laranjo N, et al. Effect of prenatal supplementation with vitamin D on asthma or recurrent wheezing in offspring by age 3 years: the VDAART Randomized Clinical Trial. JAMA. 2016;315:362–70.
A SAS Program for the 2000 CDC Growth Charts (ages 0 to <20 years). Atlanta, GA. The Center for Disease Control and Prevention. October 27, 2016; Available at: https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm. Accessed on 20 October 2016.
Langille MG, Zaneveld J, Caporaso JG, et al. Predictive functional profiling of microbial communities using 16S rRNA marker gene sequences. Nat Biotechnol. 2013;31:814–21. https://doi.org/10.1038/nbt.2676
Boulange CL, Neves AL, Chilloux J, Nicholson JK, Dumas ME. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Med. 2016;8:42.
Barlow GM, Yu A, Mathur R. Role of the gut microbiome in obesity and diabetes mellitus. Nutr Clin Pract. 2015;30:787–97.
Braithwaite I, Stewart AW, Hancox RJ. et al. Fast-food consumption and body mass index in children and adolescents: an international cross-sectional study. BMJ Open. 2014;4:e005813.
Vinding RK, Sejersen TS, Chawes BL, Bonnelykke K, Buhl T, Bisgaard H, et al. Cesarean delivery and body mass index at 6 months and into childhood. Pediatrics 2017;139:e20164066.
Kasai C, Sugimoto K, Moritani I, et al. Comparison of the gut microbiota composition between obese and non-obese individuals in a Japanese population, as analyzed by terminal restriction fragment length polymorphism and next-generation sequencing. BMC Gastroenterol 2015; 15:100.
Forbes JD, Azad MB, Vehling L, et al. Association of exposure to formula in the hospital and subsequent infant feeding practices with gut microbiota and risk of overweight in the first year of life. JAMA Pediatr. 2018;172:e181161.
Villamil SI, Huerlimann R, Morianos C, Sarnyai Z, Maes GE. Adverse effect of early-life high-fat/high-carbohydrate (“Western”) diet on bacterial community in the distal bowel of mice. Nutr Res. 2018;50:25–36.
Hollister EB, Riehle K, Luna RA. et al. Structure and function of the healthy pre-adolescent pediatric gut microbiome. Microbiome. 2015;3:36.
Eckburg PB, Bik EM, Bernstein CN. et al. Diversity of the human intestinal microbial flora. Science. 2005;308:1635–1638.
Keane KN, Calton EK, Carlessi R, Hart PH, Newsholme P. The bioenergetics of inflammation: insights into obesity and type 2 diabetes. Eur J Clin Nutr. 2017;71:904–12. https://doi.org/10.1038/ejcn.2017.45.
Cani PD, Amar J, Iglesias MA, et al. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007;56:1761–72.
Lindberg AA, Weintraub A, Zahringer U, Rietschel ET. Structure-activity relationships in lipopolysaccharides of Bacteroides fragilis. Rev Infect Dis. 1990;12(Suppl 2):S133–41.
Paun A, Danska JS. Modulation of type 1 and type 2 diabetes risk by the intestinal microbiome. Pediatr Diabetes. 2016;17:469–77.
Acknowledgements
We thank families who have taken part of the VDAART study. We would like to thank Nancy Laranjo for data management; John Ziniti and Nicholas Wolfe for helping with the microbiota data and advanced statistical analyses; Pauli Tuoresmäki for helping with the figure. We also thank the project coordinator, study coordinators and research assistants at the VDAART clinical centers (at Washington University St. Louis, Boston University Medical Center and Kaiser Permanente Southern California). This study was supported by NIH grants HL091528, HL108818 and 1UL1TR001430, and the research grants from the Academy of Finland (grant 287675); the Juho Vainio Foundation; the Foundation for Pediatric Research; and by the National Institute for Health and Welfare, Finland.
Funding
AB has received research grants from the NIH. DRG was funded by NIH grant HL108818. STW and AAL were funded by NIH grant HL091528. The remaining authors (AMK, JES, LBB, GTOC and RSZ) have no financial relationships relevant to this article to disclose.
Author information
Authors and Affiliations
Contributions
Dr. Karvonen carried out the initial statistical analyses, interpreted data, drafted the initial manuscript, and reviewed and revised the manuscript; Dr. Sordillo designed sequencing assessment, interpreted data, and reviewed and revised the manuscript; Drs. Gold, Bacharier, O’Connor, Zeiger, and Beigelman acquired and interpreted data, revised manuscript critically for important intellectual content; Drs. Weiss, Litonjua, and Gold designed the study concept. Drs. Weiss and Litonjua coordinated and supervised data collection, interpreted data, revised manuscript critically for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Karvonen, A.M., Sordillo, J.E., Gold, D.R. et al. Gut microbiota and overweight in 3-year old children. Int J Obes 43, 713–723 (2019). https://doi.org/10.1038/s41366-018-0290-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-018-0290-z
- Springer Nature Limited
This article is cited by
-
Multivariate Analysis and Correlation Study Shows the Impact of Anthropometric and Demographic Variables on Gut Microbiota in Obese Egyptian Children
Current Microbiology (2024)
-
Characterization of gut microbiota associated with metabolic syndrome and type-2 diabetes mellitus in Mexican pediatric subjects
BMC Pediatrics (2023)
-
Gut microbiome transitions across generations in different ethnicities in an urban setting—the HELIUS study
Microbiome (2023)
-
Nine weeks of high-intensity indoor cycling training induced changes in the microbiota composition in non-athlete healthy male college students
Journal of the International Society of Sports Nutrition (2021)
-
Preliminary evidence for an influence of exposure to polycyclic aromatic hydrocarbons on the composition of the gut microbiota and neurodevelopment in three-year-old healthy children
BMC Pediatrics (2021)