
Abstract
Background/Objectives:
Neuroimaging studies in obese subjects have identified abnormal activation of key regions of central reward circuits, including the nucleus accumbens (NAcc), in response to food-related stimuli. We aimed to examine whether women with elevated body mass index (BMI) show structural and resting state (RS) functional connectivity alterations within regions of the reward network.
Subjects/Methods:
Fifty healthy, premenopausal women, 19 overweight and obese (high BMI=26–38 kg m−2) and 31 lean (BMI=19–25 kg m−2) were selected from the University of California Los Angeles’ Oppenheimer Center for Neurobiology of Stress database. Structural and RS functional scans were collected. Group differences in grey matter volume (GMV) of the NAcc, oscillation dynamics of intrinsic brain activity and functional connectivity of the NAcc to regions within the reward network were examined.
Results:
GMV of the left NAcc was significantly greater in the high BMI group than in the lean group (P=0.031). Altered frequency distributions were observed in women with high BMI compared with lean group in the left NAcc (P=0.009) in a medium-frequency (MF) band, and in bilateral anterior cingulate cortex (ACC) (P=0.014, <0.001) and ventro-medial prefrontal cortex (vmPFC) (P=0.034, <0.001) in a high-frequency band. Subjects with high BMI had greater connectivity of the left NAcc with bilateral ACC (P=0.024) and right vmPFC (P=0.032) in a MF band and with the left ACC (P=0.03) in a high frequency band.
Conclusions:
Overweight and obese women in the absence of food-related stimuli show significant structural and functional alterations within regions of reward-related brain networks, which may have a role in altered ingestive behaviors.
Similar content being viewed by others


Introduction
In the lean individual, food intake and body weight are under tight homeostatic regulation.1 Bidirectional signaling between the gut, adipose tissue and the brain acts as an energy-balancing circuit, assuring a stable body weight even in the presence of fluctuations of food intake and physical activity. However, in obesity relative changes in the inputs to this circuit have to be considered, which might disrupt or off-set this balance.2 One important input comes from the mesolimbic dopamine system, which drives food-related behaviors and has a crucial role in the complex interactions between hedonia, reinforcement, motivation, incentive salience and reward prediction.3, 4 From an evolutionary standpoint, this system optimizes survival in a world of limited food supply.5 However, when highly palatable food is readily available, increasingly hedonically driven consumption can lead to an altered state of homeostasis.2 Under these circumstances, the ability to resist the urge to eat is no longer solely dependent on metabolically driven satiety signals, but becomes dependent on the inhibitory effects of prefrontal control mechanisms.
Neuroimaging studies in human subjects have highlighted the parallels between drug addiction and a subset of obesity,6 suggesting that addictive and natural reinforcement from food is dependent on the engagement of brain regions associated with reward.4 Food addiction has been implicated as an important factor in the pathophysiology of obesity in ~11% of overweight and obese women.7 For example, alterations in dopaminergic input from the ventral tegmental area and substantia nigra to the nucleus accumbens (NAcc) can lead to a dysregulation of motivational and reward properties associated with food intake.8 In fact, individual differences in NAcc responses to contextual food cues (including visual, auditory and olfactory) may be one of the main reasons for obese individuals to show addiction-like behaviors resulting in weight gain.9 The majority of insights about brain alterations in food addiction come from PET studies using dopamine receptor ligands,10 and tasked-based functional magnetic resonance imaging (MRI) studies that look at hemodynamic blood-oxygen-level dependent (BOLD) signals while subjects undergo a specific task, such as viewing images of food.11 Studies have also reported obesity-related differences in brain structure. For example, body mass index (BMI) has been shown to be positively correlated with grey matter volume (GMV) in the medial orbitofrontal cortex (OFC), hypothalamus and the left putamen.12 In addition, several studies have identified increases in GMV of the NAcc in obese subjects compared with lean subjects,12, 13 as well as in subjects who had increased eating behaviors but similar BMI compared with control subjects.13 When viewed together, these results suggest that the NAcc is not only associated with evaluating motivationally salient stimuli (food) and in evaluating its subjective value, but that chronically altered ingestive behavior is associated with neuroplastic structural changes in the NAcc.12
There is limited information about obesity-related differences in spontaneous intrinsic BOLD oscillations in the brain (resting-state (RS) functional MRI). Several RS analytic techniques such as fractional amplitude of low-frequency (LF) fluctuation (which computes regional power spectrum intensity of spontaneous brain oscillations)14 and intrinsic functional connectivity have been used to identify disease-related alterations associated with specific brain regions. Such techniques have been used to examine altered neuro-circuitry in obesity.15, 16, 17
Based on previous reports on alterations of the extended reward network in obesity, we aimed to test the following hypotheses in healthy women with and without elevated BMI values: Subjects with elevated BMIs (1) have larger NAcc volumes compared with lean controls, reflecting increased engagement of the reward system and/or secondary neuroplastic effects of obesity on the brain; (2) show alterations in intrinsic oscillatory dynamics of BOLD signal for regions of the extended reward network, including the NAcc; and (3) show increased NAcc functional connectivity within the reward network compared with lean controls.
Materials and methods
Participant selection
Fifty healthy women aged 18–40 years were recruited through the University of California, Los Angeles, and community using advertisements. The sample included 31 lean women (mean age: 25.42 years, s.d.: 5.86; BMI: 19–25 kg m−2) and 19 overweight or obese women (mean age: 27.05 years; s.d.: 7.03; BMI: 26–38 kg m−2). All subjects were right-handed, pre-menopausal and classified as healthy after a clinical assessment that included a modified Mini-International Neuropsychiatric Interview Plus 5.0,18 a brief structured interview for major Axis I psychiatric disorders in DSM-IV19 and ICD-10,20 and the Hospital Anxiety and Depression questionnaire.21
The subjects provided written informed consent and all procedures were reviewed and approved by the University of California Los Angeles Medical Institutional Review Board. Further exclusion criteria included pregnancy, substance abuse, tobacco dependence, psychiatric illness, diabetes and any digestive or eating disorders such as anorexia or bulimia nervosa. Subjects were also excluded if they were currently on medication such as analgesics or antidepressants. Subjects who had undergone any obesity-reduction surgery were also excluded.
Structural and RS data acquisition
MRI images were acquired on a Siemens 3 Tesla Trio scanner (Erlangen, Germany). Structural scans included a standard T1-weighted magnetization-prepared rapid acquisition gradient echo scan, which was acquired with the following parameters: echo time=3.26 ms, repetition time=2200 ms, slices=176, slice thickness=1.0 mm and voxel size=1 × 1 × 1 mm, with the exception of three obese subjects whose structural images were collected with the following parameters: echo time=3 ms, repetition time=2000 ms, slices=160, slice thickness=1 mm and voxel size=1 × 1 × 1 mm.
Functional MRI RS scans between 8m6s and 10m6s in length were acquired with an echo planar sequence with the following parameters: echo time=28 ms, repetition time=2000 ms, scan duration=8m6s–10 m6s, flip angel=77°, field of view=220 mm, slices=40 and slice thickness=4.0 mm, and slices were obtained with whole-brain coverage.
Structural MRI image processing and analysis
Outlines around the NAcc were manually created with the help of the intensity contour function within FSLview (FMRIB’s Software Library, www.fmrib.ox.ac.uk/fsl.22, 23 First, slices were selected where the anterior NAcc is most visible. To determine the superior border of the NAcc, an oblique line was drawn from the inferior most tip of the lateral ventricle (where it meets the caudate) to the inferior most medial tip of the putamen. Next, the inferior border of the NAcc was determined using the contour function and with the help of determining the position of the caudate (http://neuromorphometrics.org:8080/Seg/html/segmentation/accumbens_area.html). The LONI (Laboratory of Neuroimaging) pipeline (http://pipeline.loni.usc.edu/), a graphical workflow environment, was used to obtain total brain volumes for all subjects. The NAcc region of interest (ROI) values were then aggregated and entered in a general linear model in SPSS while controlling for age and total brain volumes, to compare the NAcc volumes in the two groups (obese and overweight compared with lean female subjects).
RS MRI image preprocessing
Image processing and data analysis were performed using Statistical Parametric Mapping 8 (SPM8) software (Wellcome Department of Cognitive Neurology, London, UK). Processing was done through the SPM toolbox, Data Processing Assistant for Resting-State fMRI,24 where data were slice-time and motion corrected. Nuisance covariate regression was performed to minimize physiological noise using six head motion parameters, white matter signal and corticospinal fluid signal. Data were spatially normalized to the Montreal Neurological Institute template using structural scans. Spatial smoothing with a 4-mm3 Gaussian kernel occurred after calculation of frequency and connectivity maps.24
Frequency analysis
Although frequency analyses of RS scan data typically compute power with a 0.01- to 0.10-Hz band, the frequency spectrum can be further subdivided to better reflect the neural origin of their sources.14 For each RS scan, the BOLD signal time-course data of each voxel was transformed to the frequency domain and was subdivided into slow-5 (0.01–0.027 Hz), slow-4 (0.027-0.073 Hz) and slow-3 (0.073-0.198 Hz) frequency bands thought to represent different neuronal oscillation classes.25, 26 These bands will be referred to LF, medium frequency (MF) and high frequency, respectively. Relative power within each of the three bands was computed for each voxel in the brain using fractional amplitude of LF fluctuation and normalized to the mean.14 This technique involves summing the oscillatory amplitudes across a particular frequency range (that is, 0.027–0.073 Hz), then dividing by the amplitude sum across a more inclusive range (that is, 0–.25 Hz), thereby assessing the ratio of power for a particular frequency band to the power of the entire frequency range. A grey matter mask was applied to restrict analysis to grey matter regions. For the results of the frequency band analyzes we focused on the LF and MF bands only, as the high-frequency band can contain noise (possibly due to interference from physiologic measures).
The general linear model in SPM8 was used to compare group data (overweight and obese; lean) × band (LF; MF), with age included as a covariate. Using an ROI approach,27 group contrasts (overweight and obese group versus lean group) were performed for each band, to identify regions with altered frequency power distributions. Anatomically-based ROIs were created using the Wake Forest University PickAtlas toolbox in SPM8. Regions were chosen based on involvement within the extended reward network, as upregulation of reward circuits that drive ingestive behavior include brain regions concerned with reward, salience, central autonomic and cortical inhibition (prefrontal control). The brain regions included the NAcc, hippocampus, OFC, vmPFC, ACC, amygdala, insula and regions of the striatum (caudate, putamen andpallidum).4, 5, 8 Contrast images were thresholded at P=0.001 and uncorrected and small volume correction was employed to determine significance of ROI based on P<0.05, corrected for family-wise error rate. False discovery rate was applied to control for the type I error inherent in testing multiple ROIs.28, 29
Seed-based functional connectivity analysis
Altered frequency power distribution can be accompanied by altered functional connectivity;30, 31, 32 thus, the functional connectivity of the regions identified in the above analysis was examined, focusing particularly on the region in the left NAcc. Using MarsBar,33 a seed was defined for the NAcc using results of the frequency analysis; thus, the NAcc seed was confined to the portion of the NAcc, demonstrating altered frequency distribution. For readability, the functionally defined NAcc cluster is sometimes simply referred to as the NAcc in the Results and Discussion sections. In addition, the other reward-related regions with significant group differences in frequency power were used as ROIs in the functional connectivity analysis (ACC and ventro-medial prefrontal cortex (vmPFC)). Band-specific Fisher-transformed maps of the bivariate correlation between seed ROI time course and all other voxels were created using Data Processing Assistant for Resting-State fMRI. Band-specific functional connectivity in overweight and obese versus lean women was compared using an ROI approach similar to other studies,34 and a two-sample t-test in SPM8 using age as a covariate. Significance was determined at P<0.05 family-wise error corrected and ROIs were further false discovery rate corrected for multiple comparisons.28, 29 Correlations between brain measures (structural, frequency power and functional connectivity) and BMI were conducted in SPSS.35
Results
Demographic and clinical characteristics
The subject groups showed no statistically significant difference in age or any clinical measure (Supplementary Table 1). BMI for the lean group ranged from 19.52 to 25.09 kg m−2 with an average of 22.32 kg m−2. BMI for the overweight/obese group ranged from 25.88 to 37.56 kg m−2 with an average of 31.83 kg m−2. With all values being within the normal range, the two groups also did not differ in symptom levels of anxiety (F=0.361, P=0.553), depression (F=2.301, P=0.139).
Structural analysis (NAcc volumes)
After controlling for age and total brain volume, the high BMI group had larger bilateral NAcc volumes compared with the lean group (Table 1), even though this difference only reached statistical significance for the left hemisphere (F=4.936 P=0.031). The left NAcc volume showed a significant correlation with BMI over all subjects (r=0.351; P=0.013; Figure 1).

Correlation between BMI and the left NAcc volume. Significant positive correlations were seen with increasing BMI for the left NAcc volume (r=0.351, P=0.013).
Fractional amplitude of LF fluctuation group comparison
The fractional amplitude of LF fluctuation results for the MF and LF bands are summarized in Table 2. When comparing the high BMI group with the lean group, the left NAcc had greater frequency power in the MF band (P=.009) (Figure 2a). There was no significant correlation between the left NAcc brain volume and frequency power in either the MF (r=0.228, P=0.115) or LF (r=0.126, P=0.388) bands. The bilateral ACC (left P<0.001, right P=0.014) and vmPFC/OFC (left P<0.001, right P=0.034) showed greater frequency power in the LF band (Figure 2b). There were no brain regions that had greater frequency power in the lean subjects. None of the other ROIs showed significant group differences.

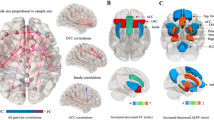
Fractional amplitude of low-frequency fluctuation (fALFF) analysis in the overweight and obese group compared with the lean group for both (a) MF (0.027–0.073 Hz) and (b) LF (0.01–0.027 Hz) frequency bands. In the MF band (a), greater frequency power was observed in the left NAcc. In the LF band (b), greater frequency power was observed in the ACC and vmPFC.
Functional connectivity of the NAcc
The region within the left NAcc and the other regions (bilateral ACC and vmPFC) identified in the above frequency analysis were used to determine the functional connectivity between these regions. These results are summarized in Table 3. The left NAcc region demonstrated band-specific altered functional connectivity with the ACC and vmPFC in the high BMI group compared with the lean group. In the MF band, greater NAcc functional connectivity was observed in the overweight and obese group with the left and right ACC (P=0.024; P=0.024), and the right vmPFC/OFC (P=0.0315) (Figure 3a). In the LF band, greater NAcc functional connectivity was observed with the left ACC (P=0.03) (Figure 3b). Functional connectivity and BMI was found to be significantly correlated for all the regions that had greater functional connectivity with the defined cluster of the left NAcc in the high BMI group for both MF (right ACC (P<0.001, r=0.522), left ACC (P=0.013, r=0.349), and right vmPFC/OFC (P<0.001, r=0.517)) and LF (left ACC (P=0.023, r=0.321)) bands. No NAcc functional connectivity was observed to be greater in the lean group.

(a and b) Functional connectivity analysis of the left NAcc with other reward-based regions in the overweight and obese group compared with the lean group. Functional connectivity analysis using the left NAcc as a seed region showed greater functional connectivity in the overweight and obese group (compared with the lean group) with reward-based regions of altered frequency identified in the fractional amplitude of low-frequency fluctuation (fALFF) analysis. In the MF band (a), greater connectivity observed between the seed region and the ACC, and R vmPFC. In the LF band (b), greater functional connectivity was observed between the seed region and L ACC.
Discussion
In this study, we examined differences between healthy women with high and normal BMI regarding NAcc volume, frequency distribution of intrinsic BOLD oscillations and in terms of NAcc functional connectivity. The main findings of the study were as follows: women with increased BMI had (1) significantly larger left NAcc volumes, (2) increased band-specific frequency power in key regions of the extended reward network, including the NAcc, and (3) increased functional connectivity of a region within the NAcc with other extended reward-related regions that had also demonstrated altered frequency. The findings of this study are consistent with an alteration in central reward circuits in the pathophysiology of obese women. To our knowledge, this is the first study to demonstrate abnormalities in the intrinsic oscillation and connectivity of the RS brain in women with increased BMI.
Increased BMI is associated with larger NAcc volume
Our findings of increased GMV of the NAcc are consistent with previous reports that focused on male/female differences (20), and adolescent (24) and elderly (46) subjects showing greater GMV in reward regions with higher BMI. Based on positive correlations between serum leptin levels and greater GMV in NAcc and ventral striatum, it has previously been suggested that the obesity-related structural differences may be a consequence of increased signaling from adipose tissue to the brain,12 rather than a consequence of altered ingestive behavior. Further support for a hypothesized role of adipocyte-related signals influencing brain structure comes from a recent study in morbidly obese subjects, in which structural brain changes were negatively correlated with body fat.36 Brain-imaging findings from other disorders of ingestive behavior (for example, anorexia nervosa and bulimia nervosa) also suggest the possible role of signals related to body fat or hydration, rather than to food intake or addiction, in the development of structural brain differences. For example, a systematic review done by Van den Eyden et al.37 suggests there is a general increase in volume of brain regions in bulimia nervosa and binge-eating disorder, which are ingestive behavioral disorders that are associated with increased eating. However, there is a general decrease in brain volumes observed in anorexia nervosa, a disorder characterized by severe reduction in food intake and loss of body fat.37 Together, these studies suggest that adipocyte-related signaling to the brain may result in both increases as well as decreases in GMV, and that these alterations are based on the degree of food and water intake. Mechanistic studies in rodent models are required to further test this hypothesis.
Increased spontaneous brain oscillations in individuals with high BMI within the LF and MF bands
To identify specific regions for the functional connectivity analyses, we first performed a regional frequency analysis of spontaneous RS oscillations. Frequency power differences showed that women with increased BMI had a greater mean amplitude in the LF and MF bands relative to the entire frequency spectrum in the left NAcc and the bilateral ACC and vmPFC (that is, regions of the extended reward network). The fact that no significant correlations were found between the left NAcc volume and oscillatory amplitude in the MF or LF bands suggests that there is no simple relationship between structural and RS differences.38, 39, 40
Although the functional consequences of differences in regional brain oscillations are not fully understood,31, 41 we may speculate about possible interpretations relevant to ingestive behavior and obesity. One interpretation of increased frequency power in lower bands (including both LF and MF bands) is that it reflects reduced neuronal firing.41, 42 Reduced activity in the NAcc could reflect the loss of dopamine 2 receptors in this brain region, which has previously been reported in obese subjects, and is associated with impaired dopamine signaling43 and a decrease in the inhibitory role of the NAcc.44 Reduced activity in the ACC and vmPFC could also reflect altered dopamine signaling, as decreased availability of striatal dopamine 2 receptors has previously been linked to decreased activity in the PFC and ACC in both obesity and drug addiction.45, 46 These cortical regions are involved in inhibitory control.47 It has been hypothesized that reduced engagement of the PFC/ACC contributes to the lack of behavioral control in individuals with different forms of addiction.6
The separation of frequency bands used in this analysis was based on the observation that behaviorally relevant brain oscillations have linearly distributed center frequencies on the natural logarithmic scale.25 Even though the functional relevance of differences obtained with this analysis method are incompletely understood,41, 42, 48, 49 it has been used in several published reports.15, 30, 38, 39, 40, 50, 51 For example, variability in frequency power has been studied in mild cognitive impairment50 as well as Parkinson’s disease where treatment-related changes in frequency power of motor cortex/basal ganglia have been related to motor performance.15, 51 Kilpatrick et al.30 identified band-specific BOLD fluctuation differences after ingestion of high-sucrose compared with low-sucrose beverages in the nucleus tractus solitarius, which also demonstrated altered band-specific functional connectivity. These studies provide support that band-specific alterations in frequency power are functionally relevant and can be used to identify affected brain regions with altered activity/connectivity.30
Increased NAcc functional connectivity with cortical reward-related regions in subjects with high BMI
The increased functional connectivity between the left NAcc cluster with the ACC and vmPFC in the high BMI group compared with the lean group in this study is similar to findings reported in individuals addicted to nicotine and other drugs.52, 53 In heroin users,54 the observed increased functional connectivity between regions involved in reward, craving and motivation (for example, between NAcc, ACC and OFC) were thought to be related to compulsive behaviors characteristic of heroin addicts. An increase in functional connectivity between the NAcc and cortical control regions has also been observed in other compulsive disorders, not related to substance abuse.53, 55 For example, in obsessive–compulsive disorder patients, greater functional connectivity of the ACC with regions including the NAcc is suggested to contribute to the loss of control observed in these subjects.55
Limitations
The unilateral structural and functional alterations observed for the (left) NAcc may be a consequence of sample size (as a trend was observed for the right NAcc), or it may reflect a true laterality. Future studies in larger populations need to address this question. There is limited information on the interpretation of frequency band oscillations and their physiological significance. Given that activation of brain regions through a task has been shown to shift frequency distribution towards higher frequencies,56 one possible interpretation of the increased lower frequency power is that these regions are less active; however, other interpretations are possible.41, 42 For example, band-specific alterations in frequency power may reflect altered balance between local processing versus long-range inputs with increased MF power reflecting greater local processing. It has also been suggested that examining functional connectivity of various bands would have similar physiological implications.31
No autonomic measures were collected to address how they might have an impact on RS measures.57, 58 However, we controlled for possible influences of autonomic activity on RS oscillations by regressing out nuisance variables and focusing on bands less influenced by physiological noise (LF and MF). As the subjects used in the study were collected from a database, we did not have consistent information in regards to dietary habits, fasting, appetite and hunger. As a result, we were not able to correlate the observed biological abnormalities with behavioral patterns of food intake. In addition, due to the nature of the data collection, time of day for the scans is variable. Finally, the study was performed only in female subjects. Several studies have reported sex-related differences in obesity, addiction and related neurobiology,12, 59, 60 and it is therefore likely to be that findings may differ in a male population.
Summary and clinical implications
Our results demonstrating structural, functional and connectivity alterations in women with increased BMI support the important role of alterations within the extended reward network, including inhibitory cortical control mechanisms that can lead to the ingestive behaviors, which are more driven by hedonic as opposed to metabolic aspects of food intake. As the subjects in this study were only selected by their differences in BMI and not by differences in behavioral measures of food intake (such as measures of food addiction), the findings suggest that such an increased influence of reward-driven mechanism is likely to be present in varying degrees in obese subjects in general. However, the alteration may become the predominant mechanism in subjects with increasing scores on the food addiction questionnaire.7 Future studies are needed to validate these observations in a larger group of male and female subjects with different degrees of behavioral food addiction, and to determine the potential use of these measures as a potential neurobiological biomarker for subsets of obese individuals. If confirmed, such biomarkers could be used to enrich patients for therapeutic trials and to evaluate the effectiveness of therapeutic interventions.
References
Havel PJ . Peripheral signals conveying metabolic information to the brain: short-term and long-term regulation of food intake and energy homeostasis. Exp Biol Med 2001; 226: 963–977.
Morton GJ, Meek TH, Schwartz MW . Neurobiology of food intake in health and disease. Nat Rev Neurosci 2014; 15: 367–378.
DiLeone RJ, Taylor JR, Picciotto MR . The drive to eat: comparisons and distinctions between mechanisms of food reward and drug addiction. Nat Neurosci 2012; 15: 1330–1335.
Volkow ND, Wang GJ, Baler RD . Reward, dopamine and the control of food intake: implications for obesity. Trends Cogn Sci 2011; 15: 37–46.
Mayer EA . Gut feelings: the emerging biology of gut-brain communication. Nat Rev Neurosci 2011; 12: 453–466.
Volkow ND, Wang GJ, Tomasi D, Baler RD . Obesity and addiction: neurobiological overlaps. Obesity Rev 2013; 14: 2–18.
Pedram P, Wadden D, Amini P, Gulliver W, Randell E, Cahill F et al. Food addiction: its prevalence and significant association with obesity in the general population. PloS One 2013; 8: e74832.
Kenny PJ . Reward mechanisms in obesity: new insights and future directions. Neuron 2011; 69: 664–679.
Demos KE, Heatherton TF, Kelley WM . Individual differences in nucleus accumbens activity to food and sexual images predict weight gain and sexual behavior. J Neurosci 2012; 32: 5549–5552.
Carnell S, Gibson C, Benson L, Ochner CN, Geliebter A . Neuroimaging and obesity: current knowledge and future directions. Obesity Rev 2012; 13: 43–56.
Garcia-Garcia I, Jurado MA, Garolera M, Segura B, Marques-Iturria I, Pueyo R et al. Functional connectivity in obesity during reward processing. Neuroimage 2012; 66C: 232–239.
Horstmann A, Busse FP, Mathar D, Muller K, Lepsien J, Schlogl H et al. Obesity-related differences between women and men in brain structure and goal-directed behavior. Front Hum Neurosci 2011; 5: 58.
Schafer A, Vaitl D, Schienle A . Regional grey matter volume abnormalities in bulimia nervosa and binge-eating disorder. Neuroimage 2010; 50: 639–643.
Zou QH, Zhu CZ, Yang Y, Zuo XN, Long XY, Cao QJ et al. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: fractional ALFF. J Neurosci Methods 2008; 172: 137–141.
Kwak Y, Peltier SJ, Bohnen NI, Muller ML, Dayalu P, Seidler RD . L-DOPA changes spontaneous low-frequency BOLD signal oscillations in Parkinson’s disease: a resting state fMRI study. Front Syst Neurosci 2012; 6: 52.
Brown VM, Labar KS, Haswell CC, Gold AL, Mid-Atlantic MW, Beall SK et al. Altered resting-state functional connectivity of basolateral and centromedial amygdala complexes in posttraumatic stress disorder. Neuropsychopharmacology 2014; 39: 361–369.
Volkow ND, Wang GJ, Fowler JS, Tomasi D, Baler R . Food and drug reward: overlapping circuits in human obesity and addiction. Curr Topics Behav Neurosci 2012; 11: 1–24.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998; 59: 22–33, quiz 34-57.
American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders 4. American Psychiatric Association: Washington, DC, 1994.
World Health Organization International Statistical Classification of Disease and Related Health Problems, Tenth Revision (IDC-10). World Health Organization: Geneva, 2004.
Mykletun A, Stordal E, Dahl AA . Hospital Anxiety and Depression (HAD) scale: factor structure, item analyses and internal consistency in a large population. Br J Psychiatry 2001; 179: 540–544.
Smith SM, Zhang Y, Jenkinson M, Chen J, Matthews PM, Federico A et al. Accurate, robust, and automated longitudinal and cross-sectional brain change analysis. Neuroimage 2002; 17: 479–489.
Woolrich MW, Jbabdi S, Patenaude B, Chappell M, Makni S, Behrens T et al. Bayesian analysis of neuroimaging data in FSL. Neuroimage 2009; 45: S173–S186.
Chao-Gan Y, Yu-Feng Z . DPARSF: A MATLAB Toolbox for “Pipeline” Data Analysis of Resting-State fMRI. Front Syst Neurosci 2010; 4: 13.
Buzsaki G, Draguhn A . Neuronal oscillations in cortical networks. Science 2004; 304: 1926–1929.
Zuo XN DMA, Kelly C, Shehzad ZE, Gee DG, Klein DF, Castellanos FX et al. The oscillating brain: complex and reliable. Neuroimage 2010; 49: 1432–1445.
Poldrack RA . Region of interest analysis for fMRI. Soc Cogn Affect Neurosci 2007; 2: 67–70.
Benjamini Y, Hochberg Y . Controlling the false discovery rate - a practical and powerful approach to multiple testing. J R Stat Soc B Met 1995; 57: 289–300.
Pike N . Using false discovery rate for multiple comparisons in ecology and evolution. Methods Ecol Evol 2011; 2: 278–282.
Kilpatrick LA, Coveleskie K, Connolly L, Labus JS, Ebrat B, Stains J et al. Influence of sucrose ingestion on brainstem and hypothalamic intrinsic oscillations in lean and obese women. Gastroenterology 2014; 146: 1212–1221.
Song X, Zhang Y, Liu Y . Frequency specificity of regional homogeneity in the resting-state human brain. PloS One 2014; 9: e86818.
Salomon RM, Cowan RL, Rogers BP, Dietrich MS, Bauernfeind AL, Kessler RM et al. Time series fMRI measures detect changes in pontine raphe following acute tryptophan depletion. Psychiatry Res 2011; 191: 112–121.
Brett M AJ, Valabregue R, Poline JB . Region of interest analysis using an SPM toolbox. Neuroimage 2002; 16, abstract 497.
Xu X, Aron A, Westmaas JL, Wang J, Sweet LH . An fMRI study of nicotine-deprived smokers' reactivity to smoking cues during novel/exciting activity. PloS One 2014; 9: e94598.
IBMCorp IBM SPSS Statistics for Windows, Version 21.0. IBM Corp.: Armonk, NY, 2012.
Karlsson AK, Kullberg J, Stokland E, Allvin K, Gronowitz E, Svensson PA et al. Measurements of total and regional body composition in preschool children: a comparison of MRI, DXA, and anthropometric data. Obesity 2013; 21: 1018–1024.
Van den Eynde F, Suda M, Broadbent H, Guillaume S, Van den Eynde M, Steiger H et al. Structural magnetic resonance imaging in eating disorders: a systematic review of voxel-based morphometry studies. Eur Eat Disord Rev 2012; 20: 94–105.
Guo W, Song Y, Liu F, Zhang Z, Zhang J, Yu M et al. Dissociation of functional and anatomical brain abnormalities in unaffected siblings of schizophrenia patients. Clin Neurophysiol 2014. e-pub ahead of print 6 September 2014; doi:10.1016/j.clinph.2014.08.016.
Hu S, Chao HH, Zhang S, Ide JS, Li CS . Changes in cerebral morphometry and amplitude of low-frequency fluctuations of BOLD signals during healthy aging: correlation with inhibitory control. Brain Struct Function 2014; 219: 983–994.
Han Y, Lui S, Kuang W, Lang Q, Zou L, Jia J . Anatomical and functional deficits in patients with amnestic mild cognitive impairment. PloS One 2012; 7: e28664.
Fox MD, Raichle ME . Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci 2007; 8: 700–711.
Pan WJ, Thompson GJ, Magnuson ME, Jaeger D, Keilholz S . Infraslow LFP correlates to resting-state fMRI BOLD signals. Neuroimage 2013; 74: 288–297.
Wang GJ, Volkow ND, Logan J, Pappas NR, Wong CT, Zhu W et al. Brain dopamine and obesity. Lancet 2001; 357: 354–357.
Russo SJ, Nestler EJ . The brain reward circuitry in mood disorders. Nat Rev Neurosci 2013; 14: 609–625.
Goldstein RZ, Volkow ND . Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 2002; 159: 1642–1652.
Volkow ND, Wang GJ, Fowler JS, Telang F . Overlapping neuronal circuits in addiction and obesity: evidence of systems pathology. Phil Transact R Soc Lond B Biol Sci 2008; 363: 3191–3200.
Bush G, Luu P, Posner MI . Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn Sci 2000; 4: 215–222.
Xue SW, Li D, Weng XC, Northoff G, Li DW . Different neural manifestations of two slow frequency bands in resting fMRI: A systemic survey at regional, inter-regional, and network levels. Brain Connect 2014; 4: 242–255.
Yu R, Chien YL, Wang HL, Liu CM, Liu CC, Hwang TJ et al. Frequency-specific alternations in the amplitude of low-frequency fluctuations in schizophrenia. Hum Brain Mapp 2014; 35: 627–637.
Han Y, Wang J, Zhao Z, Min B, Lu J, Li K et al. Frequency-dependent changes in the amplitude of low-frequency fluctuations in amnestic mild cognitive impairment: a resting-state fMRI study. Neuroimage 2011; 55: 287–295.
Esposito F, Tessitore A, Giordano A, De Micco R, Paccone A, Conforti R et al. Rhythm-specific modulation of the sensorimotor network in drug-naive patients with Parkinson's disease by levodopa. Brain 2013; 136: 710–725.
Gu H, Salmeron BJ, Ross TJ, Geng X, Zhan W, Stein EA et al. Mesocorticolimbic circuits are impaired in chronic cocaine users as demonstrated by resting-state functional connectivity. Neuroimage 2010; 53: 593–601.
Hong LE, Gu H, Yang Y, Ross TJ, Salmeron BJ, Buchholz B et al. Association of nicotine addiction and nicotine’s actions with separate cingulate cortex functional circuits. Arch Gen Psychiatry 2009; 66: 431–441.
Ma N, Liu Y, Li N, Wang CX, Zhang H, Jiang XF et al. Addiction related alteration in resting-state brain connectivity. Neuroimage 2010; 49: 738–744.
Cheng Y, Xu J, Nie B, Luo C, Yang T, Li H et al. Abnormal resting-state activities and functional connectivities of the anterior and the posterior cortexes in medication-naive patients with obsessive-compulsive disorder. PloS One 2013; 8: e67478.
Baria AT, Baliki MN, Parrish T, Apkarian AV . Anatomical and functional assemblies of brain BOLD oscillations. J Neurosci 2011; 31: 7910–7919.
Fan J, Xu P, Van Dam NT, Eilam-Stock T, Gu X, Luo YJ et al. Spontaneous brain activity relates to autonomic arousal. J Neurosci 2012; 32: 11176–11186.
Iacovella V, Hasson U . The relationship between BOLD signal and autonomic nervous system functions: implications for processing of “physiological noise”. Magn Reson Imaging 2011; 29: 1338–1345.
Lovejoy JC, Sainsbury A . Stock Conference Working G. Sex differences in obesity and the regulation of energy homeostasis. Obesity Rev 2009; 10: 154–167.
Fattore L, Melis M, Fadda P, Fratta W . Sex differences in addictive disorders. Front Neuroendocrinol 2014; 35: 272–284.
Acknowledgements
This research was supported in part by grants from the National Institute of Health: P50 DK064539, P30 DK041301, R01 DK048351 and K01 DK085133. Pilot scans were provided by the Ahamsom-Lovelace Brain Mapping Center.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies this paper on the Nutrition & Diabetes website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Coveleskie, K., Gupta, A., Kilpatrick, L. et al. Altered functional connectivity within the central reward network in overweight and obese women. Nutr & Diabetes 5, e148 (2015). https://doi.org/10.1038/nutd.2014.45
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2014.45
- Springer Nature Limited
This article is cited by
-
Excess BMI in early adolescence adversely impacts maturating functional circuits supporting high-level cognition and their structural correlates
International Journal of Obesity (2023)
-
Neuroimaging Investigations of Obesity: a Review of the Treatment of Sex from 2010
Current Obesity Reports (2023)
-
Aberrant impulse control circuitry in obesity
Molecular Psychiatry (2022)
-
Effects of gastric bypass surgery on brain connectivity responses to hypoglycemia
Endocrine (2022)
-
Body size estimation in obesity: a systematic review and meta-analysis
Experimental Brain Research (2021)