
Abstract
Purpose
Investigate the axial plane deformity in the scoliotic segment and its relationship to the deformity in the frontal and sagittal planes.
Methods
Two hundred subjects with AIS (Cobb ≥ 20°) underwent low dose biplanar X-rays with 3D reconstruction of the spine and pelvis. All structural curves were considered and were distributed as follows: 142 thoracic (T), 70 thoracolumbar (TL), and 47 lumbar curves (L). Common 3D spino-pelvic and scoliosis parameters were collected such as: frontal Cobb; torsion index (TI); hypokyphosis/lordosis index (HI). Parameters were compared between each type of curvature and correlations were investigated between the 3 planes.
Results
Frontal Cobb was higher in all T (45 ± 19°) and TL (41 ± 15°) curves compared to L curves (35 ± 14°, p = 0.004). TI was higher in T curves when compared to TL and L curves (TI: 15 ± 8°, 9 ± 6°, 7 ± 5°, p < 0.001). HI was similar between curve types. T curves showed significant correlations between the 3 planes: Cobb vs. TI (r = 0.76), Cobb vs. HI (r = − 0.54) and HI vs. TI (r = − 0.42). The axial plane deformity was related to the frontal deformity and the type of curvature (adjusted-R2 = 0.6).
Conclusion
Beside showing the most severe deformity frontally and axially compared to TL and L curves, the T curves showed strong correlations between the 3 planes of the deformity. Moreover, this study showed that the axial plane deformity cannot be fully determined by the frontal and sagittal deformities, which highlights the importance of 3D assessment in the setting of AIS.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Adolescent Idiopathic Scoliosis (AIS) is a three-dimensional spinal deformity [1] and its treatment depends on several factors, especially the frontal Cobb angle, routinely used as an indicator for the magnitude of deformity. The diagnosis and/or treatment decision based on the frontal Cobb angle alone could be biased as it is a projection of the true 3D deformity in the 2D frontal plane. The importance of 3D evaluation of the scoliotic deformity, mainly in the axial planes, and its impact on treatment planning increased in significance since the first publications of Cotrel and Dubousset and the CD instrumentation [2]. Furthermore, it has been shown that even in mild scoliosis (Cobb < 25°), the deformity can evolve, especially in the axial plane, independently of the type of curvature [3]. The axial plane has been shown to be essential in the definition of a severity index to differentiate progressive from non-progressive forms of mild scoliosis [4]. Moreover, recent studies showed that the evaluation of the axial vertebral rotation at the apex is important in the determination of brace efficacy [5]. Although the evaluation of the axial deformity in routine clinical practice is still not common, spine surgeons aim to correct the scoliotic deformity in all 3 planes, regardless of the technique used [6].
Several studies have already endeavored to better understand the relationship between the axial plane and the two remaining planes of the scoliotic deformity in subjects with AIS, with a positive correlation shown between the frontal and axial planes and a negative correlation between the frontal and sagittal planes, assessed only in major thoracic curves [7]. It was also reported that the sagittal deformity may alter the rotational stability and magnitude of scoliosis [8]. Multiple factors have been attributed to the relationship between the 3 planes, including the type of major scoliotic curvature (thoracic, thoracolumbar or lumbar) [9]. However, the previously mentioned studies mostly focused on only one type of curvature [10,11,12,13,14,15]. The study of the 3D morphology of the scoliotic segment and especially the assessment of the axial plane in different types of curvatures in subjects with AIS remains unelucidated.
Thus, the aim of this study was to investigate the axial plane deformity in subjects with AIS with different types of curves and its relationship to the frontal and sagittal deformities. We hypothesized that the axial deformity in the scoliotic segment can be determined by the frontal and sagittal deformities.
Methods
This is a cross-sectional IRB approved (CEHDF742) study. Non-operated subjects with AIS, recruited between January 2013 and December 2018, who presented to our center for radiographic assessment, aged between 10 and 18 years with a Cobb ≥ 20°, were included. Subjects with structural leg length discrepancy > 1 cm were excluded. All participants and their legal guardians signed a written informed consent form.
Data acquisition
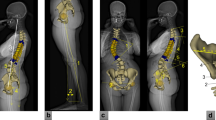
Demographic parameters were collected for each subject: age, gender, weight and height. All subjects underwent low dose biplanar X-rays (EOS® Imaging, Paris, France). Subjects were asked to stand in the free standing position [16] with subsequent 3D reconstructions of the spine (Stereos®, EOS® Imaging, Paris, France; v.1.6.4.7977) (Fig. 1). The following spino-pelvic parameters were obtained in 3D (Fig. 2): pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), L1S1 lordosis, T1T12 kyphosis, frontal Cobb, and apical vertebral rotation (AVR). The upper and lower end-vertebrae of the scoliotic curves, as well as the location of the apex were noted. Subjects were grouped by major curve type [17]: Thoracic (T, apex between T2 and T11), Thoracolumbar (TL, apex at T12 or L1) and Lumbar (L, apex between L2 and L4).

Biplanar X-ray of a subject with major thoracic curve with frontal, sagittal and axial views of the 3D spine reconstruction

3D spino-pelvic and scoliosis parameters
The 3D reconstruction was then processed using a specific software (Arts et Métiers ParisTech), and the morphological parameters used to calculate the severity index were extracted [4]: intervertebral axial rotation at the upper and lower junctions (UIAR and LIAR, respectively); torsion index (TI), calculated as the mean of the sums of the intervertebral axial rotations within the scoliotic segment, from lower to upper junction; hypokyphosis/lordosis index (HI), calculated as the difference between local kyphosis/lordosis at the apical level of the scoliotic subject, and the mean value at the equivalent level of a non-scoliotic control group (same control group as the original publication: 20F/33 M, age 21 [9–36] years) [4]. A negative value means either hypokyphosis (thoracic segment) or hypolordosis (lumbar segment). The aforementioned severity index parameters were calculated for all the structural curves. The scoliotic deformity was evaluated using the Cobb angle for the frontal plane, TI for the axial plane and HI for the sagittal plane. The validity and reliability of the 3D reconstructions were previously studied [18,19,20,21,22,23] and the estimated uncertainty on the parameters used to evaluate the 3 planes deformity is 5–6°.
Statistics
Demographic data were compared between groups of major curve types using either ANOVA or Kruskal–Wallis test (for age, weight and height) depending on the normality of the data (Shapiro–Wilk’s test), and a chi-squared test (for gender).
The spino-pelvic parameters were compared between patients depending on the major curve type. The severity index parameters were compared between all structural scoliotic segments depending on the type of curvature. Both comparisons were applied using an ANOVA or Kruskal–Wallis test.
To evaluate the relationship between the 3 planes of the deformity, Pearson’s correlations were computed between frontal Cobb (frontal plane), TI (axial plane) and HI (sagittal plane), for each type of the structural scoliotic curvatures.
To investigate the relationship between the axial plane and both the frontal and sagittal planes, a multiple linear regression was computed while considering the type of structural curvatures (ANCOVA model).
The level of significance was set at 0.05. Statistical analyses were performed using Xlstat® (Addinsoft, Paris, France; v.2018.5).
Results
A total of 200 subjects with a major Cobb of 43 ± 18° (mean ± standard deviation) [min: 20° to max:110°] were included. The sample consisted of 80 Lenke-1, 1 Lenke-2, 32 Lenke-3, 60 Lenke-5 and 27 Lenke-6. The major scoliotic curves were classified as follows: T = 115, TL = 60 and L = 25 and demographic data were comparable between groups (p > 0.05; Table 1). When including all structural curves, the scoliotic segments were classified as: T = 142, TL = 70 and L = 47.
In brief, Cobb angle was significantly lower in subjects with L curves compared to both T and TL curves (35 ± 14° and 45 ± 19° vs. 41 ± 15°, respectively). TI, UIAR and LIAR were significantly higher in subjects with T curves compared to both TL and L curves. The thoracic kyphosis T1T12 was significantly lower in subjects with major T curves compared to subjects with major L curves (30 ± 13° vs. 38 ± 12°, respectively). Detailed comparisons were presented in Table 2.
When controlling for Cobb, the HI did not differ between the types of all curvatures, indicating that the loss of lordosis or kyphosis was similar between the different types of curvature (T = − 2°, TL = − 2° and L = − 1.5°; p = 0.06). However, the TI (T = 15°, TL = 9° and L = 8°), UIAR (T = 8°, TL = 6° and L = 5°) and LIAR (T = 9°, TL = 7° and L = 5°) were still significantly higher in T curves when compared to TL and L curves (all p < 0.001).
Moderate to strong correlations were found between the 3 planes in all T curvatures but not for TL and L curves (Fig. 3). Strong positive correlations were found between TI and frontal Cobb for the 3 types of curvatures (T: r = 0.76, p < 0.001; TL: r = 0.62, p < 0.001; L: r = 0.62, p < 0.001). A strong negative correlation was found between frontal Cobb and HI for the T curves (r = − 0.54, p < 0.001), but not for the TL and L curves (p = 0.13 and p = 0.26, respectively). A moderate negative correlation was found between HI and TI for T curves (r = − 0.42, p < 0.001), but not for TL and L curves (p = 0.25, p = 0.42, respectively).

Correlations between scoliotic deformity parameters in the 3 planes in different types of structural scoliotic curvatures (T thoracic; TL thoracolumbar; L lumbar)
The multiple linear regression showed that the axial plane deformity (TI) was correlated (adjusted-R2 = 0.6) to the frontal Cobb and the type of curvature.
Discussion
The axial plane deformity is known to be primordial in the assessment of the scoliotic spine in both treatment planning and its follow-up, especially when assessing curve progression. This study evaluated the axial plane deformity in the scoliotic segment with different types of curvature and its relationship to the frontal and sagittal deformities.
Subjects with major T curves presented with more severe frontal, sagittal and axial deformities compared to TL and L curves and showed moderate to strong correlations between the deformity in the 3 planes.
As expected, the number of subjects with major thoracic deformity (n = 115) was larger than the number of subjects with major thoracolumbar (n = 60) and lumbar deformities (n = 25), as found in previous studies [24].
T1T12 kyphosis was lower in major T curves in accordance with previous studies [25]. Subjects with structural T curves presented higher TI, UIAR and LIAR when compared to TL and L curves. This finding indicates that subjects with T curves represent the primary axial deformity throughout the scoliotic segment when compared to TL and L curves. A previous study including only mild scoliosis (Cobb < 25°) showed that subjects with major T curves presented the same Cobb angle, with the same UIAR and LIAR compared to major TL and L curves but higher TI [3]. The current study, having included subjects with more severe scoliosis (Cobb ≥ 20°), showed that structural T curves presented higher Cobb, TI, UIAR and LIAR when compared to TL and L curves.
We calculated, in this study, the hypokyphosis/lordosis index (HI) comparing the local curvature, centered at the apex, to non-scoliotic subjects. The HI was found to be comparable between the three types of curvatures. This shows that the location of the scoliotic deformity creates the same amount of sagittal deformity (loss of lordosis/kyphosis), independently of the type of curvature.
It is known that subjects with major T curves have a higher rate of surgical treatment (35%) when compared to TL and L curves (13%) [26]. This could be explained by the fact that subjects with major T scoliosis present a higher magnitude of frontal deformity, as shown in the current study; this might be simply due to a recruitment bias. However, even when controlling for the Cobb angle, torsion index, UIAR and LIAR remained higher in the T group. Thus, our results show that subjects with T curves present with a higher magnitude of axial deformity compared to major TL and L curves, independently from the severity of the frontal plane.
Several studies have attempted to evaluate the relationship between the 3 planes of the scoliotic deformity [10,11,12,13] but were limited by the use of 2D frontal and lateral radiographs with a less accurate evaluation of the axial plane. A recent study, using biplanar X-rays with subsequent 3D reconstructions, found significant correlations between the 3 planes while considering only subjects with major thoracic scoliosis [7]. The current study, including all 3 types of structural curves, showed that only subjects with T scoliosis presented significant correlations between the 3 planes, with the TL and L groups only presenting correlations between the frontal and axial planes. This could be due to the fact that the thoracolumbar and lumbar segments of the spine behave differently than the thoracic segment, due to the absence of the rib cage, and to the higher mobility of the thoracolumbar and lumbar segments.
The present study showed that up to 60% (R2) of the axial deformity can be determined by the frontal deformity in AIS. Thus, at least 40% of the axial deformity remained unelucidated, highlighting the importance of evaluating the axial deformity in addition to the frontal deformity when assessing the severity of scoliosis in patients with AIS.
This finding may suggest that any surgery correcting both frontal and sagittal planes might not automatically fully correct the axial plane deformity. This was suggested by recent studies showing that surgical correction in two planes cannot fully correct the third plane [27, 28].
In conclusion, thoracic curves demonstrated more severe deformity in the frontal and axial planes compared to TL and L curves. Moreover, thoracic curves demonstrated a significant correlation between the three planes of deformity. Furthermore, the axial plane deformity cannot be fully determined from frontal and sagittal measurements which highlights the importance of independent axial measurement from 3D reconstructions when treating AIS.
References
Kane WJ (1977) Scoliosis prevalence: a call for a statement of terms. Clin Orthop Relat Res. https://doi.org/10.1097/00003086-197707000-00006
Dubousset J, Cotrel Y (1991) Application technique of Cotrel-Dubousset instrumentation for scoliosis deformities. Clin Orthop Relat Res. https://doi.org/10.1097/00003086-199103000-00012
Courvoisier A, Drevelle X, Dubousset J et al (2013) Transverse plane 3D analysis of mild scoliosis. Eur Spine J 22:2427–2432
Skalli W, Vergari C, Ebermeyer E et al (2017) Early detection of progressive adolescent idiopathic scoliosis: a severity index. Spine (Phila Pa 1976) 42:823–830
Kwan KYH, Cheung AKP, Koh HY et al (2021) Brace effectiveness is related to 3-dimensional plane parameters in patients with adolescent idiopathic scoliosis. J Bone Joint Surg Am 103:37–43
Fischer CR, Kim Y (2011) Selective fusion for adolescent idiopathic scoliosis: a review of current operative strategy. Eur Spine J 20:1048–1057
Sullivan TB, Reighard FG, Osborn EJ et al (2017) Thoracic idiopathic scoliosis severity is highly correlated with 3D measures of thoracic kyphosis. J Bone Joint Surg Am 99:e54
Adam CJ, Askin GN, Pearcy MJ (2008) Gravity-induced torque and intravertebral rotation in idiopathic scoliosis. Spine (Phila Pa 1976) 33:30–37
Upasani VV, Tis J, Bastrom T et al (2007) Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: how do these two curve types differ? Spine (Phila Pa 1976) 32:1355–1359
Hu P, Yu M, Liu X et al (2016) Analysis of the relationship between coronal and sagittal deformities in adolescent idiopathic scoliosis. Eur Spine J 25:409–416
Ni H, Zhu X, He S et al (2010) An increased kyphosis of the thoracolumbar junction is correlated to more axial vertebral rotation in thoracolumbar/lumbar adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 35:1334–1338
Morrison DG, Chan A, Hill D et al (2015) Correlation between Cobb angle, spinous process angle (SPA) and apical vertebrae rotation (AVR) on posteroanterior radiographs in adolescent idiopathic scoliosis (AIS). Eur Spine J 24:306–312
Pizones J, Zúñiga L, Sánchez-Mariscal F et al (2016) Relationship between the different torsion-related thoracic deformity parameters of adolescent idiopathic scoliosis. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-016-1762-2
Hong JY, Kim KW, Suh SW et al (2017) Effect of coronal scoliotic curvature on sagittal spinal shape. Clin Spine Surg 30:E418–E422
Hayashi K, Upasani VV, Pawelek JB et al (2009) Three-dimensional analysis of thoracic apical sagittal alignment in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 34:792–797
Faro FD, Marks MC, Pawelek J et al (2004) Evaluation of a functional position for lateral radiograph acquisition in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 29:2284–2289
Lenke LG, Betz RR, Harms J et al (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 83:1169–1181
Ilharreborde B, Jean S, Steffen S et al (2011) Angle measurement reproducibility using EOS three-dimensional reconstructions in adolescent idiopathic scoliosis treated by posterior instrumentation. Spine (Phila Pa 1976) 36:1306–1313
Glaser DA, Doan J, Newton PO (2012) Comparison of 3-dimensional spinal reconstruction accuracy. Spine (Phila Pa 1976) 37:1391–1397
Somoskeöy S, Tunyogi-Csapó M, Bogyó C et al (2012) Accuracy and reliability of coronal and sagittal spinal curvature data based on patient-specific three-dimensional models created by the EOS 2D/3D imaging system. Spine J 12:1052–1059
Rehm J, Germann T, Akbar M et al (2017) 3D-modeling of the spine using EOS imaging system: Inter-reader reproducibility and reliability. PLoS ONE 12:e0171258
Jiang F, Simões L, Ouellet J et al (2020) Accuracy of EOS imagining technology in comparison to computed tomography in the assessment of vertebral rotational orientation in instrumented spines in adolescent idiopathic scoliosis. Spine (Phila Pa 1976). https://doi.org/10.1097/brs.0000000000003739
Al-Aubaidi Z, Lebel D, Oudjhane K et al (2013) Three-dimensional imaging of the spine using the EOS system: is it reliable? A comparative study using computed tomography imaging. J Pediatr Orthop B 22:409–412
Wang W, Zhu Z, Zhu F et al (2012) Different curve pattern and other radiographical characteristics in male and female patients with adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 37:1586–1592
Newton PO, Osborn EJ, Bastrom TP et al (2019) The 3D sagittal profile of thoracic versus lumbar major curves in adolescent idiopathic scoliosis. Spine Deform 7:60–65
Dolan LA, Weinstein SL (2007) Surgical rates after observation and bracing for adolescent idiopathic scoliosis: an evidence-based review. Spine (Phila Pa 1976) 32:91–100
Miyazaki M, Ishihara T, Abe T et al (2020) Analysis of reciprocal changes in upper cervical profiles after posterior spinal fusion with the simultaneous double rod rotation technique for adolescent idiopathic scoliosis. Orthop Traumatol Surg Res 106:1275–1279
Schlösser TP, Abelin K, Jelle G et al (2020) Comparison of different strategies on three—dimensional correction of AIS: which plane will suffer? Eur Spine J. https://doi.org/10.1007/s00586-020-06659-2
Funding
This research was funded by the research council of the University of Saint-Joseph in Beirut (Project FM300).
Author information
Authors and Affiliations
Contributions
MK, CV, WS, AJB, JM, GK, KK, IG, AA: made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data; or the creation of new software used in the work. MK, CV, WS, AJB, JM, GK, KK, IG, AA: drafted the work or revised it critically for important intellectual content. MK, CV, WS, AJB, JM, GK, KK, IG, AA: approved the version to be published. MK, CV, WS, AJB, JM, GK, KK, IG, AA: agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
None.
Ethics
This is an IRB approved study (University of Saint-Joseph-CEHDF742).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Karam, M., Vergari, C., Skalli, W. et al. Assessment of the axial plane deformity in subjects with adolescent idiopathic scoliosis and its relationship to the frontal and sagittal planes. Spine Deform 10, 509–514 (2022). https://doi.org/10.1007/s43390-021-00443-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43390-021-00443-y