
Abstract
Purpose
To characterize the sagittal alignment of each Lenke type and investigate the relationship between coronal and sagittal deformities in adolescent idiopathic scoliotic (AIS) patients.
Methods
A cohort of 184 subjects with AIS was retrospectively recruited. Radiographic data were measured and collected, including the Lenke types, Cobb angles of structural curves, and sagittal spino-pelvic parameters. Subjects were grouped according to their genders, Lenke curve types, lumbar modifiers and the amount of coronal structural curves. The sagittal alignment was then compared between the different groups, and correlation analysis was also taken between coronal and sagittal parameters. Besides, each subject’s Roussouly type was decided and its distribution was compared among different Lenke types.
Results
The cohort included 59 males and 125 females, averagely aged at 15.5 ± 3.3 years old. Most sagittal parameters except thoracic kyphosis (TK) and pelvic tilt (PT) were similar among different Lenke types, while all the sagittal parameters were similar between males and females. The groups with different lumbar modifiers had similar sagittal parameters except TK, which was also true for the groups with different amounts of coronal curves. 42.4 % of the cohort belonged to Roussouly type 3, and the distribution of Roussouly types was comparable among all Lenke types. All sagittal parameters except C7 translation ratio were significantly different among Roussouly types (P < 0.05). Correlation analysis showed that main thoracic (MT) was negatively correlated with lumbar lordosis (LL, r = −0.324), sacral slope (r = −0.321) and spino-sacral angle (r = −0.363). Partial correlation analysis found that thoracolumbar/lumbar was negatively correlated with TK (r = −0.464) and LL (r = −0.422) when MT was controlled.
Conclusions
The influence of coronal deformity on sagittal parameters was limited and mainly reflected in the deviation of TK. Most coronal and sagittal parameters were not significantly correlated, and the coronal deformity types did not change the global sagittal postural patterns.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Scoliosis is usually thought to involve three-dimensional deformities [1–3] that are closely interconnected and interdependent, but this issue has not been sufficiently addressed in previous researches. Recently, the deformity of spine on coronal and sagittal planes has been separately explored and characterized in the patients with adolescent idiopathic scoliosis (AIS) [4–12], and correlation has been proven to exist between different sagittal spino-pelvic parameters [7, 10, 12, 14–18]. However, the relationship of the parameters on different planes has been seldom explored, except for some comparative studies between the groups with a thoracic or lumbar curve in AIS patients [8, 9, 11].
Mac-Thiong et al. [8] and Upasani et al. [9] reviewed the radiographs of AIS patients with a thoracic or lumbar curve and compared the sagittal parameters between these two groups. They found that thoracic kyphosis (TK) was smaller for patients with a thoracic curve, but no difference was detected as regard to pelvic incidence (PI). Likely, other cross-dimensional studies also focused on the comparison of sagittal parameters between the patients with a thoracic or lumbar curve, namely Lenke Type 1 and Type 5, but did not go beyond to include all Lenke types and explore the relationship between coronal and sagittal deformities in this setting. Legaye et al. [7] once examined the relationship between LL and the parameters on other planes, such as the rotation of apical vertebrae and the Cobb angles of coronal curves, and reported that no correlation existed between them. This conclusion, however, was not very convincing, since the report did not list out which types of coronal curves were involved in the study [7].
Through reviewing the radiographic data of all AIS patients, this study aims to characterize and compare the sagittal alignment among all Lenke types, thus to comprehensively investigate the relationship between coronal and sagittal deformities.
Materials and methods
Materials
A cohort of 184 AIS patients who visited our hospital was recruited from Jun 2006 to Dec 2013, and this study was approved by the hospital’s Institutional Review Board. The exclusion criteria were as follows: (1) chronic back pain, leg pain, headache or any other neuromuscular symptom that could obscure the diagnosis; (2) history of trauma or surgery on spine, pelvis or any other position which could alter the previous spinal alignments; (3) any co-morbidity which probably affected the spino-pelvic alignment such as pelvic deformities, leg discrepancy, spondylolysis and spondylolisthesis; (4) incompleteness of patient’s information or lack of some measurements, such as films without femoral heads and/or too vague to be accurately measured; (5) any idiosyncratic finding that would raise a doubt upon the former diagnosis during the course of radiographic review, such as severe wedged vertebrae beyond the normal range of variation.
Methods
The radiographic protocol for the subjects was consistent throughout the study. Pre-operative full length postero-anterior (PA), bending and lateral X-rays of the spine were all taken at our hospital. When taking lateral films, patients stood in an erect comfortable position, with their hands flexed 45°–60° and placed on an adjustable supporting bar (Fig. 1), and gazed horizontally to reduce any inaccuracy caused by head motion. The exposures were taken from the base of the skull to the proximal femora. The distance from the radiographic source to the film was maintained at 180 cm, and the edges of the films were squared in respect to the horizontal and vertical axes. The films were then digitized with a commercially available optical scanner (XR 650, GE, USA). All morphologic data were archived via Picture Archiving and Communication Systems (PACS, GE, USA). Then the films of the recruited subjects were retrieved and measured through PACS on diagonally 20-inch screens, with the resolution at 75 dpi.

Patients’ stance when taking lateral films. Patients stood in an erect comfortable position and were required to have their arms flexed at a consistent angle, which was about 45°–60°, by adjusting the height of a bar to support hands
The parameters and their measuring methods were decided by all authors. Measurements were separately conducted by Hu and Yu. The average results were adopted if no significant difference was found between the two measurements; otherwise, the difference was reported to the senior authors for further confirmation.
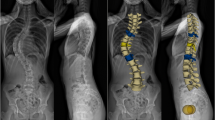
The Lenke type for each subject was re-determined, including curve types (CT, recorded as 1–6) and lumbar modifiers (LM, recorded as A to C). The Cobb angles of any structural curves were measured and recorded as proximal thoracic curve (PrT), main thoracic curve (MT) and thoracolumbar/lumbar (TL/L), as described by Lenke et al. [5]. The amounts of coronal structural curves were counted and represented by curve amounts (CA, recorded as 1–3). On lateral films, the following parameters were measured (Fig. 2): thoracic kyphosis (TK), the subtending angle between superior endplate of T1 and inferior endplate of T12; lumbar lordosis (LL), the angle between superior endplate of L1 and superior endplate of S1; sacral slope (SS), the angle subtended by the superior endplate of S1 and the horizontal line; pelvic incidence (PI), the angle subtended by the line perpendicular to the superior endplate of S1 and the line connecting the midpoint of superior endplate of S1 to hip axis (HA, the midpoint of the line connecting the centers of two femoral heads); pelvic tilt (PT), the angle subtended by the vertical line and the line connecting the midpoint of superior endplate of S1 to HA, which is positive if angulated behind the vertical line and otherwise negative; spino-sacral angle (SSA), the angle between the superior endplate of S1 and the line connecting its midpoint to C7 center, and C7 translation ratio (C7TR), the ratio of the horizontal distance between C7 plumbline and the midpoint of the superior endplate of S1 to the horizontal distance between HA and the midpoint of the superior endplate of S1, which is positive if C7 plumbline and HA are at the same side of the midpoint of superior endplate of S1 and otherwise negative. Besides, the subjects were also categorized by Roussouly classification according to their PI, SS, PT, and thoracic and lumbar sagittal alignments (Fig. 3) [13].

Representative drawings of sagittal spino-pelvic parameters. PI pelvic incidence, PT pelvic tilt, SS sacral slope, C7PL C7 plumbline, HA hip axis, TK thoracic kyphosis, LL lumbar lordosis, SSA spino-sacral angle. C7 translation ratio (C7TR) = a/b, in which “a” represents the horizontal distance between C7 PL and the midpoint of the superior endplate of S1 and “b” represents the horizontal distance between HA and the midpoint of the superior endplate of S1

Representative drawings of Roussouly types. a Type 1: Sacral slope (SS) <35°, apex of lumbar lordosis (LL) at middle L5, the spine is hypolordotic and relatively normokyphotic; b Type 2: SS <35°, apex of LL at base L4, the spine is hypolordotic and hypokyphotic, c Type 3: 35° < SS < 45°, apex of LL at middle L4, the spine is well balanced, d Type 4: SS >45°, apex of LL at base L3, the spine is hyperlordotic and hyperkyphotic
Statistics strategies
Statistical analysis was conducted with IBM SPSS statistics 19 (Chicago, IL, USA). Descriptive statistics were provided in the form of mean ± standard deviation (SD). The subjects were grouped according to gender and the coronal deformity types, including CT, LM and CA, and one-way ANOVA test (Scheffe method for the post hoc test) or Kruskal–Wallis test were then utilized to evaluate the disparities among different groups. Pearson’s correlation test and partial correlation test were utilized to explore the correlation between Cobb angles (MT and TL/L) on coronal plane and the parameters on sagittal plane. Statistical significance was set at 0.05.
Results
The cohort included 59 males and 125 females, aged at 15.5 ± 3.3 years old averagely. There were 75 subjects in Lenke Type 1, which was the largest group and composed 40.8 % of the cohort. Only 9 subjects belonged to Lenke type 6, the smallest group. PrT was similar in Lenke Type 2 and Type 4, but MT and TL/L varied significantly among the corresponding Lenke types (Table 1).
The average PI was 43.1° ± 10.1° for the cohort. All sagittal parameters were similar between males and females, as well as among different LM groups except TK (Fig. 4; Table 4). Most sagittal parameters were similar among different Lenke types except TK and PT (Tables 2, 4). Particularly, TK in Lenke Type 1 was significantly smaller than in Type 4, and all the other sagittal parameters had no significant difference between two Lenke types (Table 2). Besides, all sagittal parameters except TK were similar among different CA groups (Fig. 4; Table 4).

Comparison of sagittal angular parameters between different groups. a All parameters were similar between males and females, b TK was different between different lumbar-modifier groups but other sagittal parameters were comparable, c TK was different between the groups with different coronal curve amounts while other sagittal parameters were similar, d all angle parameters were different among Roussouly groups. *Statistically significant at P < 0.05. One-way ANOVA test
All the different Lenke groups showed a comparable distribution of Roussouly classification, with Roussouly type 3 having the largest proportion, which occupied 42.4 % of the cohort (Table 3). All sagittal parameters except C7TR were significantly different among Roussouly types (Fig. 4; Table 4).
Correlation analysis was conducted between MT and sagittal parameters for Lenke type 1 group, and between TL/L and sagittal parameters for Lenke type 5 group. Correlations were found between MT and LL, SS, SSA for the former but none between TL/L and sagittal parameters for the latter (Table 5). Furthermore, partial correlation as above was examined for subjects with double structural curves, namely Lenke Type 3 and Type 6. Correlation was found between TL/L and TK, LL, when MT was controlled, but not between MT and all sagittal parameters when TL/L was controlled (Table 6).
Discussion
This study investigated the relationship between coronal and sagittal deformities in AIS patients, identified the influence of some coronal factors (curve types, lumbar modifiers and curve amounts) upon sagittal alignment, and examined possible correlations between some parameters on the two planes. The results and findings contributed to a better understanding of this pathology.
Pelvic incidence has been reported to be relevant with the development of AIS, but whether as a compensatory or a causal factor remains unclear [7–9, 15, 19]. PI acts as a core factor in the maintenance and regulation of sagittal balance, and does not alter with one’s postures or surgery [7, 10, 15, 16, 20, 21]. This study found that PI was similar in different genders and hardly affected by coronal deformities (Fig. 4; Table 4). Averagely, PI was 43.1° ± 10.1° for the cohort, similar to Qiu’s report on Chinese AIS population [11] but lower than that of Caucasian counterparts [7–9, 12]. Besides, previous comparison studies reported similar PI between the two groups with a thoracic or lumbar curve [8, 9], which was echoed by this study (Table 4). This phenomenon was also noted by La Maida et al. [22]. Therefore, we speculated that, though PI might be relevant with the development of AIS, it could not be a strong determinant on AIS types. This speculation was consolidated by the finding of PI’s similarity among the groups categorized by coronal factors such as curve types and curve amounts (Fig. 4; Table 4) as well as its insignificant correlations with coronal Cobb angles (Tables 5, 6).
Previous articles reported that AIS patients with a thoracic curve had smaller TK than those with a lumbar curve but other sagittal parameters were comparable [8, 9, 23], which was also true in this study (Tables 2, 4). Mac-Thiong et al. [8] mentioned that TK is mainly related to the shape and orientation of thoracic vertebrae and intervertebral discs. These factors, however, are altered in AIS patients, especially in those with thoracic curves, which can result in the deviation of TK from the normal values. Correspondingly, TK in this study is smaller than that of asymptomatic population [16, 17, 23]. Moreover, TK in Lenke Type 1 was slightly smaller than in Lenke Type 5 group. But in other Lenke types which also contain a main thoracic curve, TK was comparable or even higher than in Lenke Type 5 (Table 2). This phenomenon implied that the alteration of thoracic vertebrae and discs in AIS does not always mean a decrease in TK. Besides, the correlation analysis between MT and TK in this study generated no significant result (Tables 5, 6). These findings suggested that the relationship between TK and coronal deformities was very complex rather than simple and straight.
Without the confinement of the thoracic cage, lumbar spine is more flexible than thoracic spine and prone to alter in accordance to PI, so as to compensate for the sagittal imbalance. In this study, correlation between TL/L and sagittal parameters did not bear statistical significance, except that TL/L was in partial correlation with TK and LL among the subjects with two structural curves (Tables 5, 6). In this way, any positive or negative correlation could not be solidly obtained. More regretfully, there were few previous correlation studies on the relationship between TL/L and sagittal parameters. Legaye et al. [7] once studied on adult scoliotic patients, but no statistical evidence was found for the correlation between coronal curves and LL (r = −0.04585, P > 0.05).That study recruited both thoracic and lumbar scoliotic females, but neither grouped them accordingly nor took correlation analysis separately. Therefore, its conclusion was too sketchy to be convincing. We speculated that the coronal deformity is merely one of the factors that affect LL, and that, considering the correlation chain among sagittal parameters [7–12, 14–18, 24], LL essentially acts as a compensation for the sagittal imbalance under the regulation of PI. In fact, even if the coronal deformity really has an impact on LL, correlation analysis does not necessarily generate statistically significant results, since the underlying relationship may be quite complicated rather than straightforward.
Spino-sacral angle can be a general measurement of the kyphosis of the whole spine and was repeatedly reported correlated with PI and SS [7–12, 14–19, 24]. SSA is also regulated by PI, to compensate for the alteration of sagittal alignment and to maintain the gravity axis near HA, which is coherent to the principle of bearing loads and keeping sagittal balance with the least energy expenditure [1, 7, 17, 19, 20, 22, 24]. In this study, no correlation between SSA and MT, TL/L was established (Tables 5, 6). C7 plumbline is often referred as an optimal reflection of the global spinal balance, and its clinical interpretation shall be made according to its relative position with respect to HA and supero-posterior corner of S1 [19]. Mac-Thiong et al. [14] employed C7TR (see “Materials and methods”) in their study on normal Caucasian adults, whose average C7TR was −1.1 ± 11.3. In this study, C7TR was −3.3 ± 9.0 averagely (Table 2), indicating that the C7 plumbline drifts away from HA farther among AIS patients. However, C7TR might not be an ideal parameter, as our study showed that it remained stable among almost all subgroups and did not correlate with coronal curves (Fig. 4; Tables 4, 5, 6). This study found that 72.4 % of the recruited subjects stood with C7 plumbline behind HA and supero-posterior corner of S1. The proportion is similar to Yu’s report in scoliotic population but lower than that in Mac-Thiong’s report in normal Caucasian population [12, 14]. Thus, as pointed out previously, the anterior shift of C7 plumbline may indicate the risk of the development of sagittal spinal imbalance, and the possible underlying pathology should be screened and identified [14, 19, 25].
Noticeably, this study showed that the difference of sagittal alignment among Lenke types was merely reflected in the variation of TK and PT (Tables 2, 4). It insinuated that Lenke classification might not be an effective indicator to predict the sagittal postural patterns among AIS [5]. Based on SS, the apical vertebrae of LL, lumbar tilt and the local of inflection point, Roussouly et al. [13] classified the sagittal postural patterns into four types (Fig. 3) and this classification possessed excellent capacity to stratify out the four levels of sagittal parameters, which was also confirmed by this study (Fig. 4; Table 4). Besides, similar to Yu’s report [12]. Roussouly Type 3 occupied the largest proportion of the cohort, which was 42.6 % in our study (Table 3). Intriguingly, our study found that the distribution of Roussouly types in different Lenke groups was almost identical (Table 3), suggesting that the two classifications are probably independent from each other.
One major limitation of this study was the small size of the cohort. For example, there were only 9 subjects in Lenke Type 6 group. Consequently, correlation analysis with such a small amount is not very convincing. Besides, AIS consists of deformities on three dimensions, but this article only concentrated on the relationship between coronal and sagittal deformities. Further studies may include all the three planes to be more valuable and comprehensive.
Conclusion
The sagittal parameters were similar in males and females, and the types of coronal deformity had a limited influence on sagittal parameters except thoracic kyphosis. No correlation was found between the Cobb angles of structural curves on coronal plane and most sagittal parameters. Besides, the distribution of Roussouly classification was similar among different Lenke groups and coronal deformity types did not alter the global sagittal postural patterns of AIS patients.
References
Dubousset J (1995) Three dimensional analysis of the scoliotic deformity. In: Weinstein SL (ed) Pediatric Spine: Principles and Practice. Raven Press, New York, pp 479–495
Sangole AP, Aubin CE, Labelle H et al (2008) Three-dimensional classification of thoracic scoliotic curves. Spine (Phila Pa 1976) 34(1):91–99
Schlosser TP, van Stralen M, Brink RC et al (2014) Three-dimensional characterization of torsion and asymmetry of the intervertebral discs versus vertebral bodies in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 39(19):E1159–E1166
King HA, Moe JH, Bradford DS et al (1983) The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am 65(9):1302–1313
Lenke LG, Betz RR, Harms J et al (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am 83(8):1169–1181
Qiu G, Zhang J, Wang Y et al (2005) A new operative classification of idiopathic scoliosis: a peking union medical college method. Spine (Phila Pa 1976) 30(12):1419–1426
Legaye J, Beaupere G, Hecquet J et al (1998) Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J 7(2):99–103
Mac-Thiong JM, Labelle H, Charlebois M et al (2003) Sagittal plane analysis of the spine and pelvis in adolescent idiopathic scoliosis according to the coronal curve type. Spine (Phila Pa 1976) 28(13):1404–1409
Upasani VV, Tis J, Bastrom T et al (2007) Analysis of sagittal alignment in thoracic and thoracolumbar curves in adolescent idiopathic scoliosis: how do these two curve types differ? Spine (Phila Pa 1976) 32(12):1355–1359
Lonner BS, Auerbach JD, Sponseller P et al (2010) Variations in pelvic and other sagittal spinal parameters as a function of race in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 35(10):E374–E377
Qiu Y, Liu Z, Zhu Z et al (2012) Comparison of sagittal spinopelvic alignment in Chinese adolescents with and without idiopathic thoracic scoliosis. Spine (Phila Pa 1976) 37(12):E714–E720
Yu M, Silvestre C, Mouton T et al (2013) Analysis of the cervical spine sagittal alignment in young idiopathic scoliosis: a morphological classification of 120 cases. Eur Spine J 22(11):2372–2381
Roussouly P, Gollogly S, Berthonnaud E et al (2005) Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976) 30(3):346–353
Mac-Thiong JM, Roussouly P, Berthonnaud E et al (2010) Saggital parameters of global spinal balance: normative values from a prospective cohort of seven hundred nine Caucasian asymptomatic adults. Spine (Phila Pa 1976) 35(22):E1193–E1198
Vaz G, Roussouly P, Berthonnaud E et al (2002) Sagittal morphology and equilibrium of pelvis and spine. Eur Spine J 11(1):80–87
Mac-Thiong JM, Berthonnaud E, Dimar JR et al (2004) Sagittal alignment of the spine and pelvis during growth. Spine (Phila Pa 1976) 29(15):1642–1647
Mac-Thiong JM, Labelle H, Berthonnaud E et al (2007) Sagittal spinopelvic balance in normal children and adolescents. Eur Spine J 16(2):227–234
Zhu Z, Xu L, Zhu F et al (2014) Sagittal alignment of spine and pelvis in asymptomatic adults: norms in Chinese populations. Spine (Phila Pa 1976) 39(1):E1–E6
Roussouly R, Pinheiro-Franco JL (2011) Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur Spine J 20(Suppl 5):S609–S618
Labelle H, Roussouly P, Berthonnaud E et al (2004) Spondylolisthesis, Pelvic incidence, and spinopelvic balance: a correlation study. Spine (Phila Pa 1976) 29(18):2049–2054
Le Huec JC, Aunoble S, Philippe L et al (2011) Pelvic parameters: origin and significance. Eur Spine J 20(Suppl 5):S564–S571
La Maida GA, Zottarelli L, Mineo GV et al (2013) Sagittal balance in adolescent idiopathic scoliosis: radiographic study of spino-pelvis compensation after surgery. Eur Spine J 22(Suppl 6):S859–S867
Schlosser TP, Shah SA, Reichard SJ et al (2014) Differences in early sagittal plane alignment between thoracic and lumbar adolescent idiopathic scoliosis. Spine J 14(2):282–290
Boulay C, Tardieu C, Hecquet J et al (2006) Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J 15(4):415–422
Roussouly P, Gollogly S, Noseda O et al (2006) The vertical projection of the sum of the ground reactive forces of a standing patient is not the same as the C7 plumb line: a radiographic study of the sagittal alignment of 153 asymptomatic volunteers. Spine (Phila Pa 1976) 31(11):E320–E325
Conflict of interest
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subjects of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
P. Hu and M. Yu are equal contributors and shall share the first authorship.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Hu, P., Yu, M., Liu, X. et al. Analysis of the relationship between coronal and sagittal deformities in adolescent idiopathic scoliosis. Eur Spine J 25, 409–416 (2016). https://doi.org/10.1007/s00586-015-3986-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-015-3986-y