
Abstract
Purpose
Sit-to-stand (STS) is a basic skill for maintaining a high-quality life. The purpose of this study was to examine the effect of handrail height on the peak moment of the lower extremity joint under the support of the knee joint in ST and to provide quantified kinematics and kinetics data to help determine the STS movement strategy under the optimal handrail height. This research could also provide a starting point for the design and control of STS assistive devices.
Methods
Thirty healthy young adult subjects participated in this experiment. They grabbed handrails of different heights to perform STS at a speed of their choice. Kinematics data from the marker points at the subject’s joints were obtained through a high-definition camera, and the reaction forces at the foot, hip, and knee were measured through force-measuring devices. The inverse kinetics method was used to calculate the moment of the subject’s lower limb joints. Finally, kinematics data and kinetic data were analyzed and compared.
Results and conclusions
The peak moments of the knee joint and hip joint at different handrail heights were significantly different (P = 0.005, P < 0.001). As the handrail height increased, the peak moments of the knee joint and hip joint decreased and the maximum trunk tilt angle also decreased significantly (P < 0.001). These findings indicated that the use of a combination of knee joint support and high handrails could make STS movement easier.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Sit-to-stand (STS) is one of the most common movements in daily life (Chou et al. 2003). Getting up from a sitting position is a complex activity: the process of moving from a stable 3-point support (sitting position) to a 2-point support (standing position) requires sufficient muscle strength, proper posture control, and balance skills (Naomi et al. 1995; Hirata et al. 2008; Mapaisansin et al. 2020). STS ability is the most basic skill for human beings in maintaining a high-quality life. Failure to complete this movement causes damage to the function and mobility of the lower limbs of the human body, falling, and even death (Roebroeck et al. 1994; Janssen et al., 2002; Sekiguchi et al. 2020).
The execution of STS movement varies from person to person because many factors affect an individual’s STS movement performance. These include internal factors, such as age and muscle strength of the lower limbs; and external factors, such as the handrail, seat height, and foot position (Alexander et al. 1991; Linden et al. 1994; Bohannon et al. 2008; Janssen, 2008; Turcot et al., 2012). It is difficult to change internal factors in a short period of time to achieve the effect of improving STS movement ability. Therefore, it is important to understand how to adjust external factors so that patients can perform STS movement easily and naturally (Kinoshita et al. 2015).
Maki et al. (2011) suggested that the stability of STS movement can be increased by installing handrails in appropriate positions, reducing the risk of falling for the elderly. The use of a handrail can also significantly reduce the load on the injured knee, thereby reducing pain (Qiu et al. 2019). It is therefore necessary to improve the patient’s STS movement ability by setting up a handrail. However, the handrail must be positioned at an appropriate height to help the user safely navigate the difficult stage of the STS movement.
In recent years, some scholars have evaluated the effect of handrail height on the kinematics and kinetics of lower limb joints in STS movement (Kinoshita et al. 2015; Kinoshita, 2012). Kinoshita et al. studied the effect of the height of the handrails on both sides on the kinetics of the lower limbs during STS movement. The results showed that changing the height of the handrails significantly affected the joint moment of the lower limbs. Compared to using no handrails, the combination of low handrails and high handrails reduces the joint moment of the lower limbs the most, reducing the total moment of the lower limb joints of college students and the elderly by 12% and 15%, respectively. At the same time, this combination of handrails also reduced the time required to perform STS movements. In addition, compared with using no handrails, when using low handrails, the hip flexion angle, ankle dorsiflexion angle, and trunk tilt angle will increase; when using high handrails, the hip flexion angle and trunk tilt angle will decrease.
Many studies have been conducted on handrails. Takeda et al. (2009) studied the differences in the effects of handrails on the kinematics and kinetics of pregnant and non-pregnant women. Chihara et al. (2015) determined the optimal handrail position and tilt angle when completing STS movement by comparing the total physical load of muscle. Research by Lee et al. (2018) has shown that the use of bilateral grab handrails can significantly reduce the peak joint extension moment of the lower limbs during STS movement. Yamakawa et al. (2019) have determined that for knee pain patients, placing the handrail on the affected side can reduce the peak moment of the knee joint. Kato et al. (2020) showed that compared with traditional vertical handrails, subjects produced greater handrail reaction force when using curved handrails for STS movement. A study by Qiu et al. (2020) compared the effects of different handrail grip positions and trunk tilt angles on the joint moment of the lower limbs. Numerous studies have investigated the role of handrails in STS movement, but there have been few studies on the height of the handrails, and the main studies conducted were ones in which the handrails were placed on both sides of the body. A part of the handrails of the existing STS assistive devices were set in front of the patient to help the patient complete the standing movement. For the assistive devices with the handrail set in the front, it is still necessary for us to determine which kind of handrail height can maximize the effect of the handrail.
It is difficult for the elderly or other patients to complete the STS movement due to the decreased muscle strength of the lower limbs and the limited range of motion of the knee joint. Knee joint support refers to placing a baffle in front of the patient’s knee joint to apply a force parallel to the ground and pointing to the posterior of the patient on the knee joint. At present, many STS assistive devices have adopted knee support (Burnfield et al., 2013; Mataji et al. 2015; Kim et al. 2018), combined with handrails to help improve the patient’s STS ability. So as to effectively help users complete daily activities and STS rehabilitation training. But within existing STS movement studies, we have not found any research on knee joint support. It is still unclear whether a certain amount of support at the knee joint can achieve the effect of assisting standing. Therefore, research on knee support is also very necessary.
From our analysis of the above literature, we understand that handrail height and knee joint support are crucial for STS movement. However, there are few studies on the effect of handrail height and knee joint support on STS movement, and the comprehensive effect of knee joint support and handrail height on STS movement remains unclear. The quantitative kinetics data to determine the optimal handrail height has not yet been obtained. The quantitative kinematics data that can determine the STS motion strategy with the optimal handrail height also has not yet been obtained. The purpose of this study was to examine the effect of the height of the handrails on the peak moment of the lower extremity joint under the support of the knee joint, and to provide quantified kinematics and kinetics data to help determine the STS movement strategy with the optimal handrail height. This study could also provide a starting point for the design and control of STS assistive devices.
First, we assume that the height of the handrails has a particular effect on the trunk tilt angle. The higher the handrails, the smaller the trunk tilt angle. Second, we assume that different handrail heights affect the peak joint moments of the lower limbs, including the peak joint moments of the ankle, knee, and hip. The higher the handrails, the lower the peak joint moment of the lower limbs should be.
Method
Subjects
This study recruited 30 healthy adult subjects, including 15 men and 15 women. The inclusion criteria was ability to complete the STS movement independently. Those who had undergone major orthopedic surgery, had neurological diseases and musculoskeletal mobility problems, or had any sensory, visual, auditory, or cognitive impairments were excluded. Table 1 lists the sex, age, height, and weight of the subjects. This study was conducted from March 1 to March 10, 2021, and was approved by the Academic Ethics and Scientific Ethics Committee of the Academic Committee of Tianjin University of Science and Technology. All subjects signed an informed consent form prior to participating in this study.
Instrumentation and data acquisition
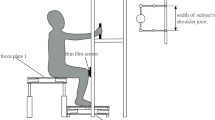
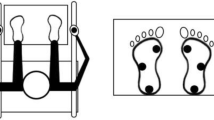
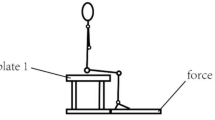
In this study, a backless, height-adjustable seat was used. The handrail was placed horizontally in front of the subjects and was cylindrical in shape with an adjustable height. When the subject stayed in a sitting position, a knee joint support was set on the front of the knee, and two flexible film pressure sensors (MD30-60, Leanstar, Suzhou, China) were placed on the knee joint support to collect data on the pressure at the knee joint. The sampling frequency of flexible film pressure sensors is 20 Hz. The seat was equipped with a force plate 1 (Fig. 1a) to collect data on the pressure on the buttocks. The force plate 1 consisted of three force sensors (GJBHX-III/50 kg, QISHENG, Bengbu, China), an intelligent digital instrument (DLV4896, QISHENG, Bengbu, China), a four-in and one-out plastic junction box (DLJXH, QISHENG, Bengbu, China), and two 400 mm × 300 mm stainless steel plates. The sampling frequency of force plate 1 is 80 Hz. Plantar reaction force data was collected by the force plate 2 located under the subject’s feet, as shown in Fig. 1b. The force plate 2 consisted of four force sensors (GJBHX-III/50 kg, QISHENG, Bengbu, China), intelligent digital instruments (DLV4896, QISHENG, Bengbu, China), four stainless steel square tubes, and two 700 mm × 500 mm stainless steel plates. The sampling frequency of force plate 2 is 80 Hz.

Force plates. a side view of the force plate 1. b side view of the force plate 2. c top view showing both force plates
Red point stickers with round white background were used as reflective markers, which were pasted on the subjects’ right side of the ankle, knee, hip, and shoulder joints, respectively, before the experiment. A high-definition camera (EOS 200D II, 1920 × 1080 pixel, 60 fps, Canon) was used to collect the kinematic data of each marker on the sagittal plane during STS movement. Subjects were required to wear black tights to prevent the shaking of fat from affecting the accuracy of the kinematic data recorded at each joint marker.
Protocol
The subject’s sitting knee height was first measured, which was defined as H1. Then the subject’s sitting shoulder height was measured, which was defined as H2. H3 was defined as the sum of sitting knee height and sitting shoulder height (Fig. 2a). Prior to the experiment, the seat height was adjusted to sitting knee height, and the subjects were asked to sit on the seat with their backs upright.

Three conditions for the STS
During the experiment, the subjects chose their preferred feet position, held the handrails with both hands, and chose the distance between the two hands. Upon the “one, two, three, start” instruction, they moved from the seat at the speed of their choice. Force plate 1, force plate 2, flexible film pressure sensors, and the high-definition camera simultaneously began to record data, until the subject completed the STS task and sent out the “stop” instruction, upon which data collection stopped.
The subjects were asked to randomly perform the following 3 sets of STS experiments (Fig. 2).
-
a)
Low Handrail (LH): Grabbing the handrail with a height of 80% H3 for STS movement
-
b)
Neutral Handrail (NH): Grabbing the handrail with a height of 100% H3 for STS movement
-
c)
High Handrail (HH): Grabbing the handrail with a height of 120% H3 for STS movement
Subjects were asked to practice each experimental condition 2–3 times to familiarize themselves with the procedure. Each experiment was carried out 3 times, and the subjects rested for an appropriate time between each experiment.
During the experiment, the points where data recording errors can occur as well as the accuracy of equipment operation ware paid special attention. In the process of data analysis, if there was an obvious error in the data of a subject. We will first look for the reason. If it is determined by the equipment during the experiment or other controllable factors in the experiment, we would do the experiment again and re-record the data until a satisfactory result was achieved.
Data analysis
Once the high-definition camera had recorded the entire process of STS, Adobe Photoshop 2018 (Adobe Systems Software Ireland Ltd, US) was used to extract each image frame at a frequency of 60 fps. Using the ankle joint marker as the coordinate origin, a Cartesian coordinate system was established to obtain the pixel position coordinates of the knee, hip, and shoulder joint. The pixel position coordinates of the makers were calibrated to obtain the actual position coordinates of each joint marker. After the image processing of the STS movement was completed, the actual trajectory of each marker point was obtained. In order to perform a kinematics analysis, a link segment model of the human body was constructed in the sagittal plane. The model consisted of four segments of the human body (head-trunk, thigh, shank, and foot) and four joints (shoulder, hip, knee, and ankle), as shown in Fig. 3. The angles between the shank, thigh, and trunk and the horizontal line of the coordinate system represented the angles of the ankle (\({{\varvec{\theta}}}_{1}\)), knee (\({{\varvec{\theta}}}_{2}\)), and hip joints (\({{\varvec{\theta}}}_{3}\)), respectively. The trunk tilt angle (\({{\varvec{\theta}}}_{4}\)) was defined as the complementary angle of \({{\varvec{\theta}}}_{3}\) and the ankle dorsiflexion angle (\({{\varvec{\theta}}}_{5}\)) was defined as the complementary angle of \({{\varvec{\theta}}}_{1}\). The position and direction of the coordinate system of the human body model were equivalent to the calibration coordinate system. The position coordinates of the markers of adjacent joints were used to obtain the joint trajectories of the knee, hip, and shoulder joints, and calculated the angles of the ankle, knee, and hip joints. The finite difference method and joint trajectory data were used to calculate the velocity of the knee, hip, and shoulder joints. Since the finite difference method is not applicable for the first and last collected data regions, the forward and backward difference methods were used at the beginning and end, respectively (Gordon et al. 2013).

The planar link segment model (θ1: ankle angle; θ2: knee angle; θ3: hip angle; θ4: trunk anteversion angle; θ5: ankle dorsiflexion angle)
This study used an inverse kinetics method to calculate the moments at the ankle, knee, and hip joints during the STS movement. Due to the different sampling frequencies of the force plate, flexible film pressure sensor, and high-definition camera, Origin 2018 (OriginLab, USA) was used to fit the data of the force plate and the flexible film pressure sensor with spline fitting. Then the interpolation points at a frequency of 60 Hz were used to determine the pressure of the foot, hip, and knee. According to inertial parameters of the adult human body, distribution of relative mass (Protection and Labour, 1988), the subject's body size parameters (length of shank and thigh) measured before the experiment, pressure value of force plates, and the flexible film pressure sensor, and the calculated kinematics data (joint angle, angular acceleration, center of mass coordinates of thigh and shank, center of mass acceleration), inverse kinetics equations were listed from the foot to the thigh. Next, the joint moment of the ankle, knees, and hip were calculated.
Force plate 1, force plate 2, flexible film pressure sensors, and the high-definition camera were turned on in advance to record data. Two seconds after these devices started to record data, the subjects were allowed to start STS movement. When processing the data, the center of pressure (COP) was calculated based on the plantar reaction force data, and the start time of STS movement was judged based on the fluctuations in the position of the COP in the anterior–posterior direction. The fluctuation of the COP in the anterior–posterior direction is the result of the vertical force change. Therefore, it was accurate and effective to use the fluctuation of the COP in the anterior–posterior direction to judge the beginning of the STS movement (Kralj et al. 1990; Lindemann et al. 2003). Since the COP data fluctuated within a certain interval, we selected the first second of COP data, and the COP fluctuation interval was calculated according to the 95% confidence interval. Starting from a certain moment, when the position of the COP was not within this fluctuation interval for 0.2 s, we considered this moment as the start time of the STS (T0). The data of different devices were intercepted from time T0 to synchronize the data of these devices.
The time of all data was normalized. The total movement time was set as T; that is, the movement started at 0% T and ended at 100% T. The variables under each experimental condition were obtained by averaging the discrete values across the three selected trails, and all kinematics and kinetics curves were produced using Origin 2018 (OriginLab, USA) for spline fitting and data smoothing.
The STS movement was divided into four phases (Fig. 4).
-
Phase I Flexion phase (T0–T1): The beginning of the movement (the change in the angle of the hip joint \(\Delta {{\varvec{\theta}}}_{3}\)> 0.1°) until the hip was about to leave the chair (the change in the angle of the knee joint \(\Delta {{\varvec{\theta}}}_{2}\)> 0.1°) was the flexion phase. During Phase I, only the trunk was tilted forward. The hip joint was in flexion, and the thighs and shank remained stable.
-
Phase II Transition phase (T1–T2): The beginning of the hip leaving the chair surface until reaching the maximum trunk tilt angle was the transitional phase. During Phase II, the hip joint was still in flexion, but the knee joint began to extend.
-
Phase III Extension phase (T2–T3): From reaching the maximum trunk tilt angle to the first stop of hip extension (the horizontal velocity of the hip joint was equal to 0 for the first time). During Phase III, the hip joint changed from flexion to extension, and the knee joint continued to extend.
-
Phase IV Stabilization phase (T3–T4): From the first stopping of the hip joint extension to the end of the STS movement.

Three phases of STS movement
Even when the subject was standing, there were varying degrees of body swaying, so it was difficult to define the end time of the stabilization phase. Thus, we have considered only phases I, II, and III.
Statistical analysis
The Shapiro–Wilk test was used to test normality. The data in this study were normally distributed (P = 0.036). Taking handrail height as the influencing factor, a one-way repeated measures ANOVA on the lower limb joint moment, lower limb joint angle, and movement time was performed to test whether there were significant differences under different handrail heights. Then the Least Significant Difference (LSD) post-hoc test was performed. All statistical analyses were performed using the SPSS 22.0 (SPSS Ver.22, IBM-SPSS Inc., Chicago, IL, USA), and the significance level was set at less than 0.05.
Results
Movement time
The average and standard deviation of total movement time and the percent of movement time in each phase to complete the STS movement under different handrail heights, as well as the results of ANOVA, are shown in Table 2. Statistical analysis of the data showed that there was no significant difference in total movement time under different handrail heights (P = 0.42). There was no significant difference in the percent of movement time in phase I (P = 0.103), phase II (P = 0.165), and phase III (P = 0.269) under different handrail heights.
Joint moment
For handrails of different heights, the average and standard deviation of the ankle, knee, and hip joint moments at T0, T1, T2, and T3 during the STS movement, as well as the results of the ANOVA and the LSD post-hoc test, are shown in Table 2.
At the beginning of the movement (T0), there were significant differences in hip joint moment at different handrail heights (P < 0.001). After the LSD post-hoc test, there were significant differences in hip joint moment at any two given handrail heights. At the end of phase I (T1), there were significant differences in knee joint moment (P = 0.035) and hip joint moment (P = 0.037) at different handrail heights. After the LSD post-hoc test, there were significant differences in knee joint moment and hip joint moment at any two given handrail heights. At the end of phase II (T2), there were significant differences in knee joint moment and hip joint moment at different handrail heights (P = 0.042, P = 0.011). After the LSD post-hoc test, there were significant differences in knee moments at any two given handrail heights, and there were also significant differences in hip joint moments at any two handrail heights. At the end of phase III (T3), there was no significant difference in ankle joint moment, knee joint moment, and hip joint moment at different handrail heights.
Figure 5 shows the average and standard deviation of the peak joint moment of 30 subjects at different handrail heights. For the ankle joint, there was no significant difference between the peak ankle moment at different handrail heights (P = 0.437). For the knee joint, there was a significant difference between the peak moment of the knee joint under different handrail heights (P = 0.005). After the LSD post-hoc test, there was a significant difference in the peak moment of the knee joint between LH and NH (P = 0.009); between NH and HH (P < 0.001); and between LH and HH (P = 0.001). For the hip joint, there was a significant difference between the peak moment of the hip joint with different handrail heights (P < 0.001). After the LSD post-hoc test, there was a significant difference in the peak moment of the hip joint between LH and NH (P = 0.026); between NH and HH (P = 0.001); and between LH and HH (P < 0.001).

Max joint moment of lower limbs. *P < 0.05
Joint angle
The average and standard deviation of the joint angles at T1 and T2 as well as the results of ANOVA and the LSD post-hoc test with different handrail heights are shown in Table 2. Under different handrail heights, there was no significant difference in the ankle angle at T1 (P = 0.423) or hip angle (P = 0.2); however, the knee angle at T1 was significantly different (P = 0.015). After the LSD post-hoc test, there were significant differences in the knee angle at any two given handrail heights.
Under different handrail heights, there was no significant difference in the ankle angle at T2 (P = 0.351) or the knee angle (P = 0.686); hip angle, on the other hand, showed a significant difference under different handrail heights (P < 0.001). Trunk tilt angle at T2 showed a significant difference under different handrail heights (P < 0.001).
Joint velocity
Figure 6 shows the joint velocities of the lower limbs at different handrail heights. The figure shows that the velocity trends of the knee, hip, and shoulder joints all increase first and then decrease. Both knee and hip joints reach their maximum velocity in the extension phase, while the maximum posterior/anterior velocity of the shoulder joints is reached in the transition phase, and maximum superior/inferior velocity occurs in the extension phase.

Joint velocity of lower limbs. The symbol (black up-pointing triangle) represents T1, and (black circle) is T2 = the maximum trunk tilt angle
Discussion
The primary purposes of this study were to examine the effect of handrail height on the peak moment of the lower extremity joint under the support of the knee joint, and to provide quantified kinematics and kinetics data. The results showed that total movement time and the percent of movement time in each phase during the STS movement were not affected by handrail height, while the peak joint moments of the knee and hip were affected by handrail height and the trunk tilt angle varied greatly under different handrail heights.
The total time to produce the STS movement under different conditions in our study was approximately 1.7 s. This finding is similar to that of Nuzik et al. (1986), who reported an STS duration of 1.8 s in a study conducted on 55 healthy adults. Norman-Gerum and Mcphee (2020) reported that healthy adults completed STS movement in 1.86 s. The time data in our study were consistent with their results. The total STS movement time described in this study is much shorter than the 2.25 s reported by Roebroeck et al. (Roebroeck et al., 1994) and the 3.33 s reported by Kralj et al. (1990). In addition, the time of the stabilization phase was not included when calculating the total time. This could also explain why our measured total time of the STS movement was shorter than theirs.
In addition, we analyzed the difference between the total time of STS movement and the percent of movement time in each phase. We concluded that neither the total time nor the percent of movement time in each phase is affected by the height of the handrail. This result differed from findings on the effect of handrail height on the total time of movement from Kinoshita et al. (2015) Their results showed that handrail height has a significant effect on movement time. Based on the difference between the two research results, we speculated that the movement time may be related not only to the height of the handrail, but also to the form of the handrail. Their article mainly used a bilateral handrail, while our study used the horizontal handrail. The difference in the form of handrail was the most likely cause of the difference in the STS movement time between the two studies. The specific relevance of this apparent conflict must be further tested and analyzed.
Regarding the joint moment of the lower limbs, the joint moments of the lower limbs at T0, T1, T2, and T3, as well as the peak joint moments of the lower limbs were analyzed during the entire STS movement. For the STS movement as a whole, the knee and hip joints had higher moments than the ankle joints. This result was consistent with the study of Pinheiro et al. (2019).
In terms of the moments at different phases, the experimental results show that the height of the handrail only had a significant effect on the moment of the hip joint at T0. From to the movement characteristics at T0, it was not difficult to find that the STS movement at T0 had just started, and the trunk was about to be tilted forward. Only the hip joint was about to participate in the movement, so the handrail height only affected hip joint moment at T0. The higher the handrail, the easier the hip joint at the beginning of the movement. At T1 and T2, the height of the handrail affected both the knee and the hip joint moments. Based on these results, we speculated that at T1 and T2, the knee and hip joints had already begun to participate in STS movement. Therefore, the moments of the knee and hip joints were different at different handrail heights. At T3, since the subject had reached the standing state, the height of the handrail no longer affected the lower limb joint moment at that time.
It is worth noting that for the knee joint, at T1 and T2, the difference in knee joint moments under NH and HH conditions was relatively small, while the moment of the knee joint under LH condition was about 0.1 Nm/KG higher than that under the other two conditions. Consequently, when the handrail height was lower than the sitting shoulder height, the knee joint required a greater moment to start STS movement, and when the handrail height was equal to or greater than the sitting shoulder height, the moment required for the knee joint to begin the STS movement was relatively small. Throughout the STS movement, there was no significant difference in the ankle joint moment at different handrail heights. This could be due to the fact that this study was conducted under the condition of knee joint support, which would greatly limit the ankle dorsiflexion angle. The ankle dorsiflexion angle did not change from T0 to T1. After T1, the ankle dorsiflexion angle began to decrease. In comparison with the case of no knee joint support, the ankle dorsiflexion angle did not increase. Therefore, the handrail height had little effect on the ankle moment.
For the peak joint moment of the lower limbs in the entire STS movement, there was no significant difference in the peak moment of the ankle joint at different handrail heights. Only the peak moments of the knee and hip joints were affected by handrail height. Under LH conditions, the peak moment of the knee joint was 0.62 N.m/kg, and the peak moment of the hip joint was 1.296 N.m/kg. Under NH conditions, the peak moment of the knee joint was 0.555 N.m/kg, and the peak moment of the hip joint was 1.178 N.m/kg. Under HH conditions, the peak moment of the knee joint was 0.516 N.m/kg, and the peak moment of the hip joint was 1.026 N.m/kg. Given these values, it was not difficult to determine that as the height of the handrail increased, the peak joint moments of the knee and hip both decreased. Yoshioka et al. (2014) studied the effect of seat height on STS movement and found that the peak hip joint moment was approximately 1.1 N.m/kg when the seat height was 40 cm, similar to the hip joint moment calculated in our study. The seat height used in our study was determined based on the sitting knee height of the subjects. In our study, from a statistical analysis of the subjects’ body size information, the average knee height was about 40 cm. This could further demonstrate the effectiveness of our study. In addition, Yoshioka et al. obtained a knee joint moment peak of 0.85 N.m/kg and an ankle joint moment peak of 0.5 N.m/kg in their experiment with a seat height of 40 cm; both of these values were larger than the peak moments measured in our study. We believe that this is mainly due to the use of knee joint support in our experiment. When the knee joint was supported, a horizontal posterior force was added to the knee joint. In contrast to the case of STS movement without knee joint support, this force had a significant effect on reducing the joint moment of the knee and ankle, helping to reduce effort.
Regarding the maximum trunk tilt angle, there were significant differences in the trunk tilt angle under different handrail heights. The results of this study showed that as the height of the handrail increased, the maximum trunk tilt angle decreased. The reason for this might be that the handrail used in this study was positioned directly in front of the subject. When the handrail was raised, the restriction on the trunk tilt angle would increase. When there was a handrail in front, the subject would also decrease their forward lean for fear of touching the handrail. A similar viewpoint was also put forward in a previous study (Dekker et al. 2007). The handrail placed in front of the subject would grant them a certain psychological aversion and limit the tilt angle of the subject's trunk. The study by Yoshioka et al. (2007) showed that the trunk tilt angle is an important parameter for STS. They studied the relationship between the STS movement mode and the peak joints moment and showed that the peak moment of the hip joint can be significantly reduced when the trunk tilt angle is small. This result is consistent with our research results. The trunk tilt angle in the HH condition was the smallest, and the peak hip joint moment was also the smallest. Based on this, we concluded that the use of high handrails could reduce the peak joint moments of the lower limbs. For patients with weak lower limb muscle strength, increasing the height of the handrail could effectively help them complete the STS movement.
Due to the nature of our subjects and experimental protocols, this study has certain limitations. First, this study used young subjects, aged around 24. An analysis of the elderly and the patient populations has not yet been carried out, so the results of this study cannot not be directly applied to the elderly and patient populations. Second, although the subjects included both men and women, the interaction between handrail height and gender has not been analyzed, and further study is needed. Third, this study was completed under knee joint support. There was no control group; that is, the knee joint support was removed, and experiments with LH, NH, and HH were carried out to study the specific effects of knee joint support. Future study should utilize a control group to investigate the effect of the knee joint support. Finally, when performing STS kinematics and kinetic parameter measurement, the experimental setup we used was different from the experimental setup used in other studies. Although the measurement results basically reflected the characteristics of human kinematics and kinetics. The difference in the experimental setup will have a certain impact on the comparison between our measurement results and the measurement results of other studies.
Conclusion
In summary, we found that under the condition of knee joint support, the height of the handrail is an important factor that affects the moments of the lower limb joints in STS. By comparing the peak moments of the ankle, knee, and hip joints, we found that when using high handrails, the peak moments of the knee and hip joints are the smallest. For the knee and hip joints, a high handrail could help patients complete STS movement with the least amount of effort and help the patient navigate this difficult stage of STS movement more easily. This finding is of great help in determining the patient’s movement strategy, and it is also extremely important for the design and control of STS assistive devices. Regarding the STS assistive device that uses knee joint support and handrails to help patients complete STS, for instance, the designer could choose high handrails to help patients complete the movement. In view of the phase joint angles shown in Table 2, the designer could determine the postures that the patient should have at different phases and use the assistive device to help the patient reach these postures. The velocity of STS movement could be controlled according to the velocity profiles in Fig. 6 to enable the patient to perform the STS movement more easily.
Data availability
The datasets used and/or analyzed for the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Alexander NB, Schultz AB, Warwick DN. Rising From a Chair: Effects of Age and Functional Ability on Performance Biomechanics. J Gerontol. 1991;3:91–8.
Bohannon RW, Barreca SR, Shove ME, Lambert C, Masters LM, Sigouin CS. Documentation of daily sit-to-stands performed by community-dwelling adults. Physiother Theory Pract. 2008;24(6):437–42.
Burnfield J M, Bernadette M C, Yu S, et al. Comparative Kinematic and Electromyographic Assessment of Clinician- and Device-Assisted Sit-to-Stand Transfers in Patients With Stroke[J]. Physical Therapy (10):1331–41.
Chihara T, Fukuchi N, Seo A. Optimum position and orientation of handrail for sit-to-stand movement. Journal of Advanced Mechanical Design Systems and Manufacturing. 2015;9(3):JAMDSM0036–JAMDSM0036.
Chou SW, Wong AMK, Leong CP, Hong WS, Tang FT, Lin TH. Postural control during sit-to stand and gait in stroke patients. Am J Phys Med Rehabil. 2003;82(1):42–7.
Dekker D, Buzink SN, Molenbroek JMF, Bruin RD. Hand supports to assist toilet use among the elderly. Appl Ergon. 2007;38(1):109–18.
Gordon D, Robertson E, Caldwell GE. Research Methods in Biomechanics, Research Methods in Biomechanics, Place Published, 2013.
Hirata Y, Higuchi J, Hatsukari T, Kosuge K. Sit-to-stand assist system by using handrail and electric bed moving up and down. IEEE Ras & Embs International Conference on Biomedical Robotics & Biomechatronics. 2008.
Janssen WGM, Bussmann Hans BJ, Stam HJ. Determinants of the Sit-to-Stand Movement: A Review. Phys Ther. 2002;9:9.
Janssen WGM. The Sit-to-Stand Movement recovery after stroke and objective assessment. erasmus mc university medical center rotterdam. 2008.
Kato T, Sekiguchi Y, Honda K, Izumi S, Kanetaka H. Comparison of handrail reaction forces between two different handrails during sit-to-stand movement in the elderly - ScienceDirect. Clinical Biomechanics, 2020, 80.
Kim S W, Song J, Suh S, et al. Design And Experiment Of A Passive Sit-To-Stand And Walking (STSW) Assistance Device For The Elderly[C]// 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE, 2018.
Kinoshita S. Handrail position and shape that best facilitate sit-to-stand movement. J Back Musculoskelet Rehabil. 2012;25(1):33–45.
Kinoshita S, Kiyama R, Yoshimoto Y. Manabu. Effect of Handrail Height on Sit-To-Stand Movement. Plos One. 2015, 10(7): e0133747.
Kralj A, Jaeger RJ, Munih M. Analysis of standing up and sitting down in humans: definitions and normative data presentation. J J Biomech. 1990;23(11):1123–38.
Lee SJ, Mehta-Desai R, Oh K, Sanford J, Prilutsky BI. Effects of bilateral swing-away grab bars on the biomechanics of stand-to-sit and sit-to-stand toilet transfers. Disabil Rehabil Assist Technol. 2018;14(3):1.
Lindemann U, Claus H, Stuber M, et al. Measuring power during the sit-to-stand transfer[J]. Eur J Appl Physiol. 2003;89(5):466–70.
Linden DWV, Brunt D, Mcculloch MU. Variant and invariant characteristics of the sit-to-stand task in healthy elderly adults. Arch Phys Med Rehabil. 1994;75(6):653–60.
Maki BE, Sibley KM, Jaglal SB, Bayley M, Brooks D, et al. Reducing fall risk by improving balance control: Development, evaluation and knowledge-translation of new approaches[J]. J Safety Res. 2011;42(6):473–85.
Mapaisansin P, Suriyaamarit D, Boonyong S. The development of sit-to-stand in typically developing children aged 4 to12 years: Movement time, trunk and lower extremity joint angles, and joint moments. 2020 (76) 14–21.
Matjacic Z, Zadravec M, Oblak J. Sit-to-Stand Trainer: An Apparatus for Training "Normal-Like" Sit to Stand Movement[J]. IEEE Transactions on Neural Systems & Rehabilitation Engineering A Publication of the IEEE Engineering in Medicine & Biology Society, 2015, 24(6).
Naomi K, Fukagawa, Albert, B, Schultz. Muscle Function and Mobility Biomechanics in the Elderly: An Overview of Some Recent Research. J Gerontol A Biol Sci Med Sci. 1995, 50A(Special Issue):60–63.
Norman-Gerum V, Mcphee J. Comprehensive description of sit-to-stand motions using force and angle data[J]. J Biomech. 2020;112:110046.
Nuzik S, Lamb R, Vansant A, Hirt S. Sit-to-Stand Movement Pattern A Kinematic Study. Phys Ther. 1986;66(11):1708.
Pinheiro C, Lopes J M, Moreira L, Sanz-Merodio D, Garcia E. Kinematic and kinetic study of sit-to-stand and stand-to-sit movements towards a human-like skeletal model. 2019 IEEE 6th Portuguese Meeting on Bioengineering (ENBENG). IEEE, 2019.
Protection B, Labour MO. Human dimensions of Chinese adults. 1988.
Qiu C, Okamoto S, Yamada N, Akiyama Y, Yamada Y. Patient Simulation: Handrail Position for Knee-OA Patients Considering Physical Burden and Stability. 2019 IEEE 1st Global Conference on Life Sciences and Technologies (LifeTech). 2019.
Qiu C, Okamoto S, Akiyama Y, Yamada Y. Lower-limb moments during sit-to-stand movement with different handrail grip position and trunk tilt angle. 2020 IEEE/SICE International Symposium on System Integration (SII). IEEE, 2020.
Roebroeck ME, Doorenbosch CAM, Harlaar J, Jacobs R, Lankhorst GJ. Biomechanics and muscular activity during sit-to-stand transfer. Clin Biomech. 1994;9(4):235.
Sekiguchi Y, Honda K, Phakdepiboon T, Jinde M, Kato T, Kanetaka H, Izumi S. Effects of shelf bar assistance on kinetic control during sit-to-stand in healthy young and elderly subjects. ScienceDirect. Journal of Biomechanics, 2020, 106.
Takeda K, Katsuhira J, Takano A. Effects of handrail use during sit-to-stand in the third trimester. Int J Ind Ergon. 2009;39(6):988–94.
Turcot K, Armand S, Fritschy D, Hoffmeyer P, Suvà D. Sit-to-stand alterations in advanced knee osteoarthritis. Gait & Posture. 2012;36 1:68–72.
Yamakawa K, Okamoto S, Kubo R, Yamada N, Akiyama Y, Yamada Y. Knee Pain Patient Simulation for Recommendation of Sit-to-Stand Handrail Positions.IEEE Transactions on Human-Machine Systems, 2019, PP (99):1–7.
Yoshioka S, Nagano A, Himeno R, Fukashiro S. Computation of the kinematics and the minimum peak joint moments of sit-to-stand movements. Biomed Eng Online. 2007;6(1):26–26.
Yoshioka S, Nagano A, Hay D C, Fukashiro S. Peak hip and knee joint moments during a sit-to-stand movement are invariant to the change of seat height within the range of low to normal seat height. BioMedical Engineering OnLine,13,1(2014–03–12), 2014, 13(1):27.
Acknowledgements
The authors thank The Tianjin Natural Science Foundation (19JCZDJC33200), Tianjin Natural Science Foundation (18JCQNJC75300).
Funding
This study has been funded by The Tianjin Natural Science Foundation (19JCZDJC33200), Tianjin Natural Science Foundation (18JCQNJC75300).
Author information
Authors and Affiliations
Contributions
Conceptualization: Min Li, Qiang Xue, Shuo Yang, Xiaolong Han, Shouwei Zhang.
Formal analysis: Min Li
Methodology: Min Li, Qiang Xue
Supervision: Qiang Xue
Visualization: Xiaolong Han, Shouwei Zhang
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Academic Ethics and Scientific Ethics Committee of the Academic Committee of Tianjin University of Science and Technology.
Consent to participate
All subjects provided informed consent prior to participation.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, M., Xue, Q., Yang, S. et al. Effects analysis of handrail height on sit-to-stand movement under knee joint support in healthy young adults. Res. Biomed. Eng. 38, 617–628 (2022). https://doi.org/10.1007/s42600-022-00212-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42600-022-00212-4