
Abstract
Studying the stability of sit-to-stand (STS) could provide a foundation for clinicians when guiding rehabilitation training. The influence of the seat height on STS stability is unclear. The primary goal of this paper was to identify the position of the center of pressure (COP) and the lower limb joint angles during STS movement from different seat heights in order to analyze the relationship between joint angle and COP and understand the influence of seat height on stability during the STS movement. Thirty young volunteers participated in this experiment. The COP offset in the anterior–posterior direction (COP [ap]) and the change in distance of the COP and the center of gravity (COP–COG) were analyzed and compared. The results indicated that seat height has a significant effect on COP at Extension phase (Phase III [p = 0.045]), and COP–COG at the time when the buttocks are about to leave the seat (T1 [p = 0.01]). The stability of STS from the low seat was better than from the high seat. The lower limb joint angles at the time when the hip joint angle reaches its maximum value (T3) and COP (ap) during Phase III were negatively correlated, while lower limb joint angles at the time when the buttocks are about to leave the seat (T1) and COP–COG at the time when the buttocks are about to leave the seat (T1) were positively correlated. The ankle joint angle had more influence than other lower limb joints on STS stability at the time when the buttocks are about to leave the seat (T1).
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The sit-to-stand (STS) movement must be repeated many times a day as a necessary component of independent activities of daily living (Pavão et al. 2015; Brech et al. 2013; Millor et al. 2014). Studies have shown that difficulty performing the STS movement increases the risk of falls and death (Pena Cabra and Watanabe 2013; Sloot et al. 2020), as well as the rate of injury and hospitalization (Buurke et al. 2023). Compared with walking, people fall more frequently during STS (Rapp et al. 2012; Pozaic et al. 2016). Riley et al. (1997) classified failure to complete the STS movement into two types. The first, called the “sitback” failure, occurs when an individual rises only slightly off the chair and then sits back down. The second, called the “step” failure, occurs when an individual is unable to stop the movement in a stable standing position, causing them to take a forward step. Both of these situations are related to the instability caused by poor balance control ability. To improve the STS movement and prevent falls, it is very important to study patterns of stability and instability during this functional movement.
Current research on stability during STS primarily includes two aspects: the influence of movement strategy on STS stability and the role of subject-specific factors, including age, disease, and psychological factors, in STS stability. Jeon et al. (2019) studied STS stability in adults when performed with symmetrical and asymmetrical foot positions and found that using an asymmetrical initial foot position during the STS movement improved postural stability. Akram and McIlroy (2011) defined the stable phase of the STS movement, calculated the total path of the center of pressure (COP), and found that foot position did not affect the duration of the stable phase or the total COP path during the initial second of the stable phase. This research improves the understanding of the dynamic instability of STS. Fujimoto and Chou (2012) compared STS stability in the elderly and young people and found that age affected the acceleration of the center of mass during the STS movement, thereby affecting stability. Honda et al. (2021) investigated the differences in lower limb muscle power (LLMP) during sit-to-stand exercise between young and older adults with a reduced seat height. The results indicated that elderly participants exhibited significantly lower forward LLMPs and upward center of mass velocity (CoMv) compared to their younger counterparts, while there was no significant difference in forward CoMv. Suriyaamarit and Boonyong (2020) investigated the effects of seat height and seat forward tilt on STS ability in children with spastic cerebral palsy. Jones et al. (2016) examined the impact of seat height and forelimb rise on the dynamics of Sit-to-walk and sit-to-stand-walk tasks in young, healthy individuals. Pavão et al. (2015) studied the effect of cerebral palsy on the stability of children during STS and found that cerebral palsy primarily affected stability during the initial phase of STS. Aberg et al. (2010) found that fear factors have an impact on stability in the mediolateral direction during STS movement. Yang et al. (2023a) compared the motion feature parameters obtained under different initial foot angles (IFA) and explored the effects of different IFA on body kinematics and dynamics in STS tasks.
Modifying the seat height is an important tool clinicians use when formulating rehabilitation plans and guiding rehabilitation training (Sadeh et al. 2023). A higher seat reduces the trunk tilt angle, hip angular velocity, and peak moment (Munro et al. 1997; Suriyaamarit and Boonyong 2020; Rodosky et al. 1989; Yang et al. 2023b; Arborelius et al. 1992), and the studies by Pavão et al. (2015) and Jeon et al. (2019) demonstrated that trunk tilt angle and hip joint angular velocity affected stability; thus, it is important to study the effect of seat height on stability during STS. However, few studies have evaluated the effect of seat height on STS stability. When the seat height changes, the change in the COP in the anterior–posterior (AP) direction during the STS movement is unclear, as is the relationship between joint angle and COP during STS.
The primary goal of this paper was thus to identify the position of the COP and the lower limb joint angles during STS movement from different seat heights in order to analyze the relationship between joint angle and COP and understand the influence of seat height on stability during the STS movement. It serves as a foundation for clinicians to develop STS rehabilitation training plans and guide the process of rehabilitation training. Simultaneously, it holds significant implications for future rehabilitation chair design.
2 Method
2.1 Subjects
A total of 30 young people aged 20–30 years were recruited as subjects for this study, comprising 15 males and 15 females. The subjects’ characteristics are presented in Table 1. All subjects had to be able to independently complete the STS movement without assistance in order to be included in the study. The exclusion criteria were those with a history of any major surgery; those with vision, hearing, or sensation impairments; and those with neurological or musculoskeletal diseases. The recruitment period was from December 10 to December 25, 2021. The study was approved by the Academic Ethics and Scientific Ethics Special Committee of the Academic Committee of Tianjin University of Science and Technology. All subjects signed an informed consent statement prior to participating in this study.
2.2 Instrumentation
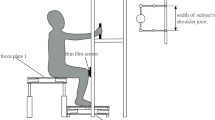
We used a high-definition camera (EOS 200D II, 1920 × 1080 pixel, 60fps Canon, Tokyo, Japan) to collect kinematic data in the sagittal plane during STS, as shown in Fig. 1. Two force plates were installed, one on the chair and one under the subjects’ feet, to measure reaction force. Each force plate included adjustable anchor bolts, two 700 mm × 500 mm stainless steel plates with a thickness of 5 mm, and four force sensors (GJBHX-III/50 kg, QISHENG, Bengbu, China). The force sensors were distributed on the four corners of the stainless-steel plate and had a sampling frequency of 80 Hz.

Experimental setup
2.3 Protocol
As shown in Fig. 2, we designed two experimental conditions: a low seat (L) with a height of 420 mm and a high seat (H) with a height of 520 mm. The low seat height (420 mm) is the same as the standard seat height (420 mm). The standard seat height is set as the average of the sitting knee height at the 50th percentile of adult males and adult females. The high seat height is 100 mm higher than the low seat height. Before collecting data, markers were attached to the ankle, knee, hip, and shoulder joints on the right side of each subject's body. All subjects were required to wear black tights to prevent excessive movement from affecting the accuracy of the markers during STS, and crossed their arms across their chests and sat on a chair without a backrest.

Diagram showing the two experimental conditions, with a low seat (L) and a high seat (H) condition
During data collection, after the subject sat down, the high-definition camera and the two force plates began sampling simultaneously. Four seconds later, a “prepare, start” instruction was issued, and the subject stood up from the seat at their speed of choice. After completing the STS, the subject was issued a “stop” instruction, at which time each device ceased recording data.
2.4 Data analysis
STS movements were captured with a high-definition camera to obtain sagittal-plane images of the body, which were then imported into Adobe Photoshop 2018 (Adobe Systems Software Ireland Ltd) to extract each image frame. The ankle joint marker was used as the coordinate origin, a Cartesian coordinate system was established to obtain the pixel coordinates of the knee, hip, and shoulder joint markers, and the actual coordinates of each marker were obtained through calibration.
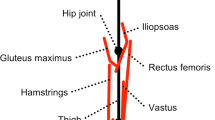
To perform kinematic analysis, as shown in Fig. 3, the ankle joint was defined as the origin (in the OXY coordinate system, the AP direction was X, the vertical direction was Y, and the coordinate system was consistent with the coordinate system established when we obtained kinematic data through image processing) and a link segment model of the human body was established that included the foot, shank, thigh, and trunk (including the head). The angles formed by the shank, thigh, and trunk with the positive horizontal axis represented the ankle joint angle (θ1), knee joint angle (θ2), and hip joint angle (θ3), respectively. All data were normalized to time. The kinematic data of the ankle, knee, and hip joint angles were then calculated based on the obtained marker trajectory data.

Link segment model of the human body in the sagittal plane
Due to the different sampling frequencies of the force plates and the high-definition camera, we performed spline curve-fitting on the STS kinematics and foot reaction force. The data were then interpolated at a frequency of 60 Hz to obtain the data required to calculate the COP and center of gravity. The STS start time was determined based on the fluctuations in the COP in the AP direction (Yamako et al. 2017; Frykberg and Häger 2015). We assumed that the COP data fluctuated within a certain interval when the subject was at rest.This fluctuation interval was calculated by selecting the COP data from the first second and calculating the COP fluctuation interval withing this time frame with 95% confidence interval. The start time of the STS was defined as the moment when the COP exceeded the fluctuation interval for 0.2 s. The end of the STS movement was defined as the moment when the hip joint angle reached its maximum value for the first time.
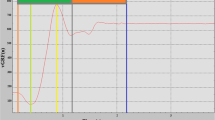
T0 is the start time of the exercise, T1 is the time when the buttocks are about to leave the seat, T2 is the time when the hip joint angle reaches its minimum value, and T3 is the time when the hip joint angle reaches its maximum value. We divided the STS process into three phases, as shown in Fig. 4. Phase I was the flexion momentum phase (T0–T1), Phase II was the momentum transfer phase (T1–T2), and Phase III was the extension phase (T2–T3).

Three phases of the sit-to-stand movement
We used the maximum offset of the COP and the ankle joint in the AP direction (COP [ap]) to describe the stability during each phase (Phase I, Phase II and Phase III) and the change in distance of the COP and the center of gravity (COP–COG) to describe the stability of each STS key position (T1, T2, and T3). The larger the value of COP (ap) and COP–COG, the worse the stability (Medeiros et al. 2015).
2.5 Statistical analysis
The normality of the COP and joint angle data was tested using the Shapiro–Wilk test, and the data were determined to have a normal distribution. The Shapiro–Wilk normality test is a statistical procedure employed to ascertain whether a given dataset adheres to a normal distribution. This test is extensively recommended due to its ability to accommodate small sample sizes (< 50 samples) (González-Estrada and Cosmes 2019). SPSS 17.0 (SPSS Inc, Chicago, IL) was used for data analysis, and the significance level was p < 0.05. The effect of seat height on subjects' COP (ap), COP–COG, and joint angles was analyzed by single-factor repeated measures analysis of variance. Anova with a single factor of repeated measures can be employed to compare the variances in the observed measurements at various time points. This design mitigates the impact of inter-individual variations on the comparison of outcome metrics. Pearson correlation analysis was used to analyze the correlation between joint angle and COP (ap) and between joint angle and COP–COG. The Pearson correlation coefficient was originally used in statistics to represent the correlation between two variables. It is now widely used in natural sciences to measure the correlation between two variables (Wang et al. 2022).
3 Results
3.1 Stability
As shown in Table 2, we compared the differences in COP (ap) during each phase and across the entire STS movement under two conditions, as well as the differences in COP–COG at T1, T2, and T3. p value represents a significant level, and p value < 0.05 is considered significant. Eta squared (η2), it represents the proportion of the degree of variation of the dependent variable that can be explained among all degrees of variation through analysis of variance. η2 < 0.01, it is a small effect. η2 < 0.06, it is a moderate effect.η2 < 0.14,it is a major effect. In the AP direction, there was not a significant difference between the two conditions in COP (ap) during Phase I and Phase II (p = 0.861 and p = 0.949, respectively), while there was a significant difference between the two conditions in COP (ap) during Phase III (p = 0.045). There was a significant difference between the two conditions in COP–COG at T1 (p = 0.01), while there was not a significant difference between the two conditions in COP–COG at T2 and T3 (p = 0.29 and p = 0.14, respectively).
3.2 Joint angle
As shown in Table 3, we compared the differences between the two conditions in joint angles at T0, T1, T2, and T3. The ankle angles under the two conditions were significantly different at T0, T1, and T2 (p = 0.022, p = 0.002, and p < 0.001, respectively), and there was no significant difference at T3 (p = 0.745). The knee angles during high and low seat conditions were significantly different at T0, T1, and T2 (p < 0.001, p < 0.001, and p < 0.001, respectively), while they were not significantly different at T3 (p = 0.225). There was a significant difference between conditions in hip joint angle at T2 (p = 0.043) and no significant difference at T0, T1, and T3 (p = 0.544, p = 0.596, and p = 0.273, respectively).
3.3 Correlation analysis
As shown in Table 4, we analyzed the correlation between COP (ap), COP–COG, and the joint angles at T1, T2, and T3. The correlation between COP (ap) and ankle joint is significant at T3 time, but not significant at T1 and T2 time. The correlation between COP (ap) and knee joint is significant at T2 and T3, but not significant at T1. The correlation between COP (ap) and ankle joint is significant at T3 time, but not significant at T1 and T2 time. The correlation between COP–COG and ankle joint is significant at T1 and T3, but not significant at T2. The correlation between COP–COG and knee joint is significant at T1 and T3, but not significant at T2. The correlation between COP–COG and hip joint is significant at T1 time, but not significant at T2 and T2 time.
4 Discussion
This study aimed to identify changes in COP and lower limb joint angles when the seat height changes during the STS movement in order to analyze the relationship between joint angle and COP and understand the influence of seat height on stability during the STS movement. For this reason, we carried out STS experiments under high and low seat conditions.The results indicated that seat height has a significant effect on COP (ap), COP–COG, and lower limb joint angles. The angles of the ankle, knee, and hip joints at T1 and T3 were correlated with COP (ap) and COP–COG.
Medeiros et al. (2015) and Danion and Latash (2011) reported that the greater the COP displacement, the worse the stability. When comparing STS under two conditions, we found that in the AP direction, the STS stability in the low seat condition (COP [ap] = 46.909 mm) was better than the STS stability in the high seat condition (COP [ap] = 57.619 mm) during Phase III. The seat height may have primarily affected stability during Phase III by influencing body posture at T2. Some studies have shown that a higher seat height reduce the trunk tilt angle (Munro et al. 1997; Suriyaamarit and Boonyong 2020). As shown in Fig. 5, according to our phase division, the trunk tilt angle reaches its maximum value at T2. At this time point, the trunk tilt angle of the low seat condition (35°) was greater than the trunk tilt angle of the high seat condition (32°) and the ankle joint angle of the low seat condition (74°) was smaller than the ankle joint angle of the high seat condition (76°); thus, at T2, the body’s center of gravity in the low seat condition was closer to the ankle joint. As the postures under the two conditions were virtually identical at T3, the horizontal displacement of the center of gravity in Phase III was small when the seat was low; therefore, the stability during the low seat condition was good.

Comparison of body postures at different time points under high seat (blue) and low seat (black) conditions
As shown in Fig. 5, under the two conditions, body posture was virtually the same at T0. In the low seat condition, the body was more anterior at T1 and the horizontal displacement of the center of gravity was greater during Phase 1 than in the high seat condition. However, the results of the analysis of variance showed no significant difference in COP (ap) between low seat and high seat conditions. Because the subject did not leave the seat between T0 and T1, this may be due to the seat providing stability for the subject, causing there to be minimal effect on COP (ap) during Phase I.
As STS movement failure usually occurs at the time of seat off (T1) and the end of the extension phase (T3) (Sloot et al. 2020), we primarily focused on STS stability at T1 and T3. At T1, stability under the low seat condition (COP–COG = 112.8 mm) was better than stability under the high seat condition (COP–COG = 138.1 mm). Figure 5 depicts the increased forward body tilt, anterior center of gravity, and smaller distance between the center of gravity and the ankle joint in the low seat condition, which all indicate a better STS stability.
Correlation analysis showed that the COP (ap) in Phase III was negatively correlated with the angles of the ankle, knee, and hip joints at T3, indicating that the larger the joint angle at T3, the smaller the COP (ap) value in Phase III. This provided a unique understanding of this phase of STS. When patients are performing rehabilitation training and require additional stability during STS, their lower limb joint angles should be increased as much as possible at T3, perhaps by attempting to maintain the shank and trunk perpendicular to the ground, to reduce the COP (ap) and improve the STS stability.
Correlation analysis results indicated that the COP–COG at T1 was positively correlated with the angles of the ankle, knee, and hip joints at T1. As shown in Fig. 6, there was no significant difference between conditions in hip joint angles at T1, which indicates that the seat height had no significant effect on the hip joint angle. However, there was a significant difference in the COP–COG at T1 between the two conditions; the change in hip joint angle was thus less than the change in COP–COG. Therefore, we inferred that hip angle had little effect on stability in the high and low seat conditions. As shown in Fig. 6, there were significant differences between conditions in the angles of the knee and ankle joints at T1, indicating that the seat height had a significant impact on the knee and ankle joint angles. There were also significant differences in COP–COG values at T1 between the two conditions, suggesting that the knee joint angle and ankle joint angle influenced STS stability.

Joint angles, COP (ap), and COP–COG under low (L) and high (H) seat conditions at T1, T2, and T3
We further compared the effects of the ankle and knee joints on stability. As shown in Fig. 6, at T1, the ankle joint angle was 75° during the low seat condition and 79° during the high seat condition. Because the ankle angle at T1 was positively correlated with the COP–COG and the COP–COG in the low seat condition was smaller than the COP–COG in the high seat condition, STS stability could be considered better under the low seat condition. However, at T1, the knee angle during the low seat condition was 159° and the knee angle during the high seat condition was 152°. Knee joint angle and COP–COG were positively correlated at T1, and the COP–COG in the low seat condition was larger than the COP–COG in the high seat condition, which would indicate a better STS stability in the high seat condition. Based on the results presented in Table 2, at T1, the COP–COG was small when the seat was low; therefore, we can infer that the ankle joint angle had a larger influence on stability.
Our results showed that body posture at T1 and T3 affected STS stability. For people with poor muscle strength and balance ability, STS stability can be improved by changing body posture during rehabilitation training. For example, when performing STS from a high seat, the patient can consciously increase the forward tilt of the trunk at T1, bringing the body's center of gravity closer to the ankle joint and thereby improving stability at T1. Additionally, the enhancement of stability effectively mitigates the risk of falls during STS movement for the elderly or individuals with mobility challenges. The incorporation of high seats and distant armrests in the design of rehabilitation chairs enables patients to voluntarily increase the forward tilt of their torso, bringing the center of gravity of the human body closer to the ankle joint, thereby improving the stability of STS movement. The rehabilitation chair can assist the patient in sit-stand conversion rehabilitation training and walking training, so as to improve muscle strength and delay the degeneration of muscle strength. In addition, clinicians should focus on modifying ankle joint angles when formulating rehabilitation training plans and guiding rehabilitation training to optimize STS stability. For example, the patient could use the position of the foot closer to the chair to reduce the angle of the ankle joint at T1, improve the stability at T1, and prevent the occurrence of 'seatback' failure.
Correlation analysis results indicated that the COP–COG at T3 was negatively correlated with the angles of the ankle and knee joints at T3. Therefore, their ankle angles should be increased as much as possible at T3, perhaps by attempting to maintain the shank perpendicular to the ground, to reduce the COP -COG and prevent the occurrence of 'seatback' failure.
Based on the results, we came to the following conclusions: First, STS stability from the low seat was better than from the high seat during Phase III. Second, STS stability from the low seat was better than from the high seat at T1, and STS stability was similar in the two conditions at T3. Third, lower limb joint angles at T3 and COP (ap) during Phase III were negatively correlated, while lower limb joint angles at T1 and COP–COG at T1 were positively correlated. Fourth, the ankle joint angle had more influence than other lower limb joints on STS stability at T1.
This study had certain limitations. First, all subjects in this study were healthy young adults. There are significant differences in muscle strength among different populations, and elderly and recovering patients are often less likely to sit to stand from lower seat heights. Therefore, the data obtained cannot be generalized to other populations, such as the elderly and rehabilitation patients. Future studies should include older adults, convalescent patients, and high body mass index to improve the generality of the conclusions. Second, only two seat heights were studied in our research. Previous studies have shown that the tilt of the chair surface and the position of the body on the chair surface could affect STS (Suriyaamarit and Boonyong 2020; Yoshioka et al. 2014; Janssen et al. 2002); The tilt angle of the chair surface and the position of the human body sitting on the chair surface can cause changes in the angles of various joints during the STS movement of the human body. Consequently, the findings of this research are exclusively applicable when the chair surface is level and individuals assume identical seating positions. Subsequently, we will ascertain the positioning of the human body on the chair surface and the impact of the chair surface's inclination on stability. Finally, the number of participants in this study is 30, and each participant is required to conduct four different trials. In the video processing stage, we extract image frames from the video, each with 44 image frames, and select the coordinates of four joint points in each image frame. Data processing mainly includes: joint trajectory, angle, angular velocity, angular acceleration, joint velocity, acceleration, motion time, and joint torque; In addition, it is necessary to calculate the pressure center based on the ground reaction force. This is a significant workload, and extensive data processing work limits the number of repetitions in experiments, which has a certain impact on the reliability of the data. We will solve this problem in the future work.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Aberg, A.C., Frykberg, G.E., Halvorsen, K.: Medio-lateral stability of sit-to-walk performance in older individuals with and without fear of falling. Gait Posture 31(4), 438–443 (2010)
Akram, S.B., McIlroy, W.E.: Challenging horizontal movement of the body during sit-to-stand: impact on stability in the young and elderly. J. Mot. Behav. 43(2), 147–153 (2011)
Arborelius, U.P., Wretenberg, P., Lindberg, F.: The effects of armrests and high seat heights on lower-limb joint load and muscular activity during sitting and rising. Ergonomics 35(11), 1377–1391 (1992)
Brech, G.C., et al.: Correlation of postural balance and knee muscle strength in the sit-to-stand test among women with and without postmenopausal osteoporosis. Osteoporos Int. 24(7), 2007–2013 (2013)
Buurke, T.J.W., van de Venis, L., den Otter, R., et al.: Comparison of ground reaction force and marker-based methods to estimate mediolateral center of mass displacement and margins of stability during walking. J. Biomech. 146, 111415 (2023)
Danion, F., Latash, M.L.: Motor Control: Theories, Experiments, and Applications. Oxford University Press, New York (2011)
Frykberg, G.E., Häger, C.K.: Movement analysis of sit-to-stand—research informing clinical practice. Phys. Ther. Rev. 20(3), 156–167 (2015)
Fujimoto, M., Chou, L.S.: Dynamic balance control during sit-to-stand movement: an examination with the center of mass acceleration. J. Biomech. 45(3), 543–548 (2012)
González-Estrada, E., Cosmes, W.: Shapiro–Wilk test for skew normal distributions based on data transformations. J. Stat. Comput. Simul. 89(17), 3258–3272 (2019)
Honda, K., Sekiguchi, Y., Sasaki, A., et al.: Effects of seat height on whole-body movement and lower limb muscle power during sit-to-stand movements in young and older individuals. J. Biomech. 129, 110813 (2021)
Janssen, W.G.M., Bussmann, H.B.J., Stam, H.J.: Determinants of the sit-to-stand movement: a review. Phys. Ther. 82(9), 866–879 (2002)
Jeon, W., Jensen, J.L., Griffin, L.: Muscle activity and balance control during sit-to-stand across symmetric and asymmetric initial foot positions in healthy adults. Gait Posture 71, 138–144 (2019)
Jones, G.D., James, D.C., Thacker, M., et al.: Sit-to-walk and sit-to-stand-and-walk task dynamics are maintained during rising at an elevated seat-height independent of lead-limb in healthy individuals. Gait Posture 48, 226–229 (2016)
Medeiros, D.L., et al.: The influence of seat heights and foot placement positions on postural control in children with cerebral palsy during a sit-to-stand task. Res. Dev. Disabil. 43–44, 1–10 (2015)
Millor, N., et al.: Kinematic parameters to evaluate functional performance of sit-to-stand and stand-to-sit transitions using motion sensor devices: a systematic review. IEEE Trans. Neural Syst. Rehabil. Eng. 22(5), 926–936 (2014)
Munro, B.J., et al.: A kinematic and kinetic analysis of the sit-to-stand transfer using an ejector chair. J. Biomech. 31(3), 263–271 (1997)
Pavão, S.L., Santos, A.N., Oliveira, A.B., et al.: Postural control during sit-to-stand movement and its relationship with upright position in children with hemiplegic spastic cerebral palsy and in typically developing children. Braz. J. Phys. Ther. 19, 18–25 (2015)
Pena Cabra, O.D., Watanabe, T.: Experimental evaluation of balance prediction models for sit-to-stand movement in the sagittal plane. Comput. Math. Methods Med. 2013, 592328 (2013)
Pozaic, T., et al.: Sit-to-stand transition reveals acute fall risk in activities of daily living. IEEE J. Transl. Eng. Health Med. 4, 2700211 (2016)
Rapp, K., et al.: Epidemiology of falls in residential aged care: analysis of more than 70,000 falls from residents of bavarian nursing homes. J. Am. Med. Dir. Assoc. 13(2), 187.e1-187.e6 (2012)
Riley, P.O., Krebs, D.E., Popat, R.A.: Biomechanical analysis of failed sit-to-stand. IEEE Trans. Rehabil. Eng. 5(4), 353–359 (1997)
Rodosky, M.W., Andriacchi, T.P., Andersson, G.B.: The influence of chair height on lower limb mechanics during rising. J. Orthop. Res. 7(2), 266–271 (1989)
Sadeh, S., Gobert, D., Shen, K.H., et al.: Biomechanical and neuromuscular control characteristics of sit-to-stand transfer in young and older adults: A systematic review with implications for balance regulation mechanisms. Clin. Biomech. 109, 106068 (2023)
Sloot, L.H., et al.: Slow but steady: similar sit-to-stand balance at seat-off in older vs younger adults. Front Sports Act Living 2, 548174 (2020)
Suriyaamarit, D., Boonyong, S.: Comparison of the effects of chair height and anterior seat inclination on sit-to-stand ability in children with spastic diplegic cerebral palsy. J. Biomech. 113, 110098 (2020)
Wang, Y., Zhao, J., Yang, C., et al.: Remaining useful life prediction of rolling bearings based on Pearson correlation-KPCA multi-feature fusion. Measurement 201, 111572 (2022)
Yamako, G., et al.: Quantification of the sit-to-stand movement for monitoring age-related motor deterioration using the Nintendo Wii Balance Board. PLoS ONE 12(11), e0188165 (2017)
Yang, S., Yi, Z., Zhou, B., et al.: Effect of initial foot angle (IFA) on kinematics and dynamics of body during sit-to-stand transfer. Medicine 102(10), e33184 (2023a)
Yang, S., Huang, X., Zhou, J., et al.: Application of robotic lower limb orthosis for people with lower limb dysfunction. Rev. Sci. Instrum. 94, 4 (2023b). https://doi.org/10.1063/5.0140319
Yoshioka, S., et al.: Peak hip and knee joint moments during a sit-to-stand movement are invariant to the change of seat height within the range of low to normal seat height. Biomed. Eng. Online 13(1), 27 (2014)
Acknowledgements
We would like to acknowledge the funding agencies for the support of the work.
Funding
This research was funded by Key Project of Tianjin Natural Science Foundation, Grant Number 19JCZDJC33200.
Author information
Authors and Affiliations
Contributions
Conceptualization, S.Y. and Q.X.; methodology, P.J.; validation, S.Y., Q.X. and S.Z.; investigation, P.J. and S.Z.; resources, S.Y., Q.X. and J.P.; data curation, J.P. and N.Z.; writing—original draft preparation, S.Z. and S.Y.; writing—review and editing, Q.X. J.P.; All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Academic Ethics and Scientific Ethics Committee of the Academic Committee of Tianjin University of Science and Technology. All subjects provided informed consent prior to participation.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yang, S., Jia, P., Zhao, N. et al. Effect analysis of seat height on sit-to-stand movement stability in healthy young adults. Int J Intell Robot Appl (2024). https://doi.org/10.1007/s41315-024-00368-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41315-024-00368-5